PART 2: UCSF - April 2012 to February 2014
Dr James Chen* and Dr Janice Lee**
"Unsightly..."
2012 I spent spring break researching impacted canines and trying to get a second opinion at UCSF, I finally succeded in getting an orthodontist and an oral surgeon appointment.
(* there are several Dr James Chen in the Bay Area, do not confuse. This Dr Chen was board certified in 2012, assistant adjunct professor at UCSF, and then moved on to be part of an orthodontist group at iSmiledental in
Mountain View.
** Dr. Janice Lee was a professor at UCSF department of Oral and Maxillofacial Surgery, and then left for the National Health Institute and the Dental and Craniofacial Research)
I asked Dr Tso for something to bring along to our UCSF appointments, he gave me copies of x-rays and this sentence: 'Since there was only a thin layer of bone overlying the impacted canine crowns at the time of
surgery, ankylosis of the crowns was not apparent.
I asked Dr Wong to write the formal referral. He wrote: "impacted canines".
April 27th, 2012. At UCSF, Dr Chen proposed to try pulling a bit more. New angle. Dr Lee scoffed when I presented my case and related how we ended up at UCSF. She evidently thought it presumtive I had sought advice from Dr. Becker. She consistently scoffed at everything and left us bewildered and uneasy. It felt like we were in the wrong place and with a situation that elicited disdain for some reason. It sounded like surgery was a favor she was doing Dr Chen. She said she could clear bone for the teeth to erupt and put on new brackets if needed. The surgeon sounded more grim than positive, at one point said 'unsightly' talking of possible outcomes, the word stayed with me. (I tried changing surgeon, but Dr Chen assured us that she nevertheless was very good and was the surgeon he worked with.)
From Dr Lee's pre-surgery notes on April 27, 2012:
There is evidence of orthodontic chains protruding through the buccal mucosa in front of 6 and 27. There does not appear to be sufficient
space for these teeth.
We reviewed the Panorex over the course of the past two years to the most recent image, and there does not appear to be significant change.
It is difficult to tell whether there has been any root resorption and difficult to see if an osseous track was created for these teeth. Additionally,
tooth #17 and 18 are impacted. 18 appears to have periodontal disease and pocketing on the medial aspect and is mesially tipped. No other
abnormalities
...
I think one thing we should do, however, is to get a cone-beam CT and to determine the exact positioning of the teeth.
....
I had a chance to speak with Dr. Chen, and he agrees that a cone-beam CT will be taken in the next few weeks and he would like to reevaluate the
exact position of these teeth. If possible, he will try to bring them back into the arch orthodontically using the current wires, and I would recommend
possibly elastic traction on 6 and 27 to one another. This may avoid opening up of the anterior bite. If there is bone in the way of the normal
movement of 6 and 27, I would recommend creating an osseous track or an osteotomy at the time that #17 is extracted and #18 is uprighted. He
agrees and will reevaluate the cone-beam CT at their next visit.
(Money aspect: $3 500 for orthodontia, $ 1580 for surgery)
Images from 9/15/2011, taken by Dr Tso pre-surgery that were on a CD for Dr Lee and Chen:
|
|

|

|
|
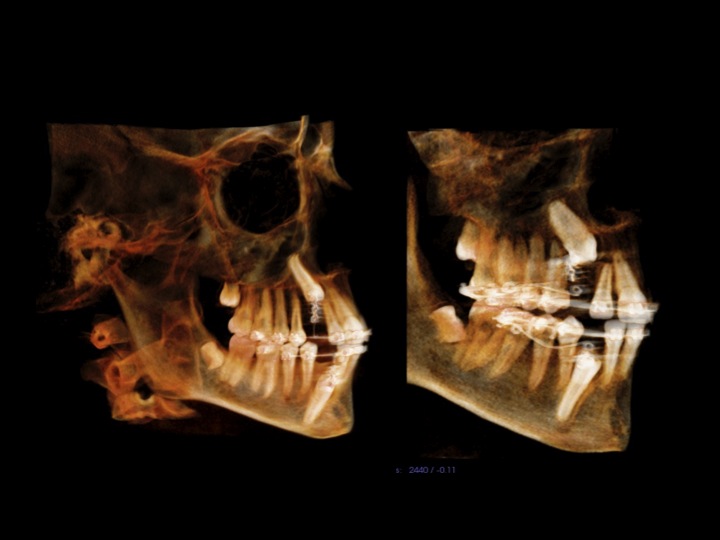
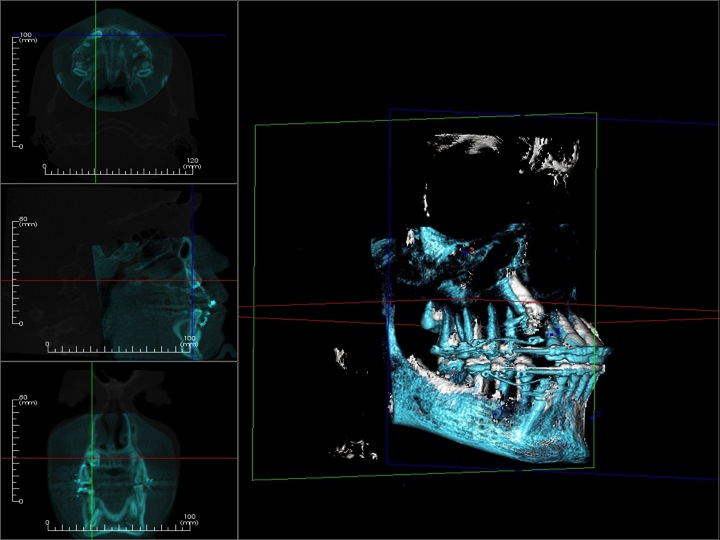
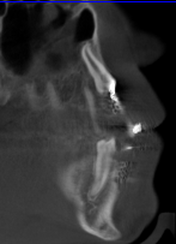
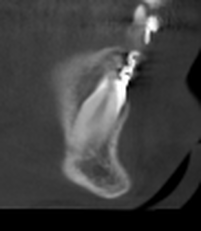
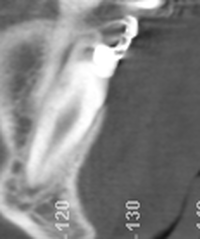
CBCT #1, May 10, 2012 (Cone Beam Computer Tomography)
(Money aspect: $ 388) 25 µSiv for Sam (Wouldn't you know, the first time we showed up, the newly installed newer model had just broken down.) |
CBCT at UCSF
For the referral form: clic
According to the form:
The cost of scan is $350 which includes: One 3-D scan session, processed images printed on photo paper
quality paper, a CD of archived images/video clips, and a basic dental radiologist report.
A detailed patology-specific radiologist report is an additional $ 35.
(We paid $388, and the orthodontist showed the above images. I never saw a radiologist report. The oral surgeon never looked at the images even though she ordered them. The orthodontist never studied them, saying they were for the benefit of the surgeon...
My letter to consumerwatchdog.org.
For the referral form: clic
According to the form:
The cost of scan is $350 which includes: One 3-D scan session, processed images printed on photo paper
quality paper, a CD of archived images/video clips, and a basic dental radiologist report.
A detailed patology-specific radiologist report is an additional $ 35.
(We paid $388, and the orthodontist showed the above images. I never saw a radiologist report. The oral surgeon never looked at the images even though she ordered them. The orthodontist never studied them, saying they were for the benefit of the surgeon...
My letter to consumerwatchdog.org.
More traction
First available appointment to start traction was June 22. Dr Chen continued over 3 months, with visits every 5 weeks, to pull on the canines without success . A new operation was scheduled. The plan at this point was to hope that the canines could still be pulled into position, but even if they turned out to be ankylosed, which actually seems to be very rare in children, the teeth would be left in place until Sam's mouth and teeth were fully developed so that the integrity of the arc was preserved up to when implants could be considered.
"Oh, CBCT...Did you bring it?"
Expose & Bond # 2, 9/21/2012
(Money aspect: expose & bond x 2 = $ 1160, sedation = $ 370, total: $ 1580)
Arriving for the surgery in the morning, Dr. Lee was looking at the old panoramas (from 2010 and April 2012). I got an uneasy feeling and tried: 'we did do the CBCT'. Her response was: 'oh, did you bring it.'
It was very disconcerting to find that the surgeon was unaware of the CBCT, had not studied it, and had not had some sort of conference with Dr Chen. She could not access the CBCT images from the operating room. (Oral surgery is on the first floor, orthodontics on the third and the radiology is also on the first floor of the same building.) Besides all of that, a CBCT is not something you review scalpel in hand!
Dr Lee looked at the couple of CBCT images on my iPad. (The irony is that we initially sought this surgeon, because I saw her name connected to a paper on CBCT so I thought it was something she would think worthwhile.)
I regret that I let the surgeon operate under the circumstances. If I had known what I know now, I would have taken my son and walked out.
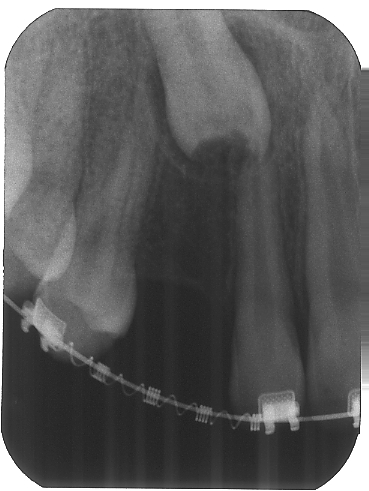
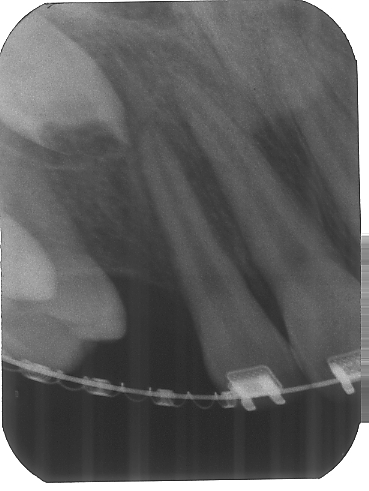
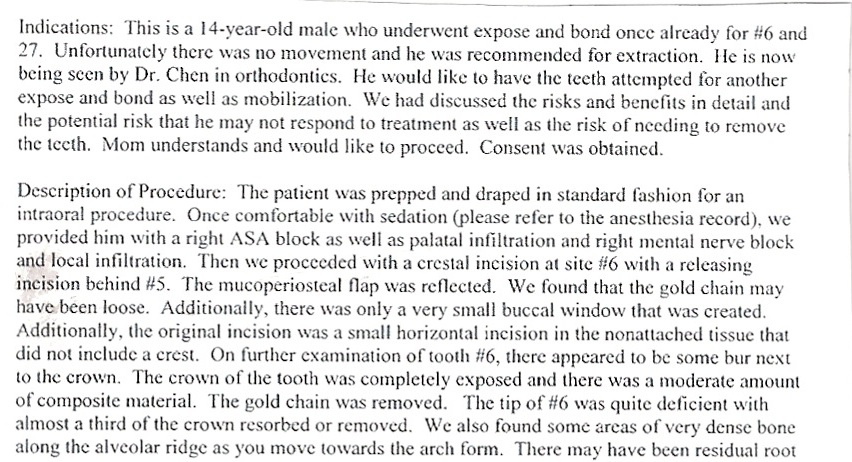
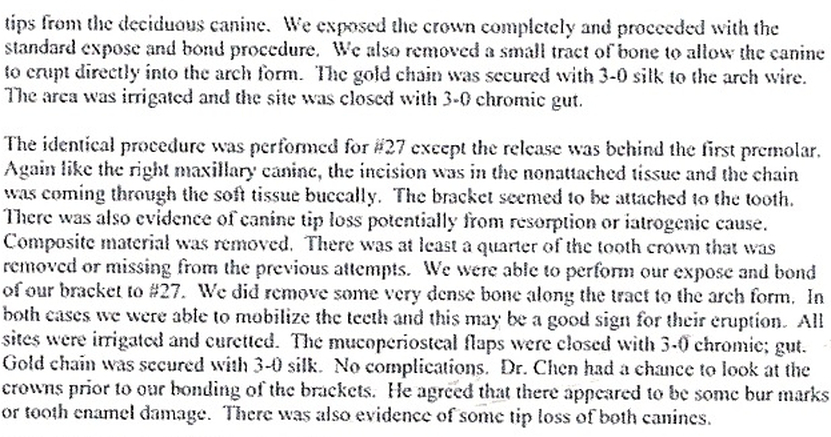
Sam's surgery took two hours. Surgery notes:
First available appointment to start traction was June 22. Dr Chen continued over 3 months, with visits every 5 weeks, to pull on the canines without success . A new operation was scheduled. The plan at this point was to hope that the canines could still be pulled into position, but even if they turned out to be ankylosed, which actually seems to be very rare in children, the teeth would be left in place until Sam's mouth and teeth were fully developed so that the integrity of the arc was preserved up to when implants could be considered.
"Oh, CBCT...Did you bring it?"
Expose & Bond # 2, 9/21/2012
(Money aspect: expose & bond x 2 = $ 1160, sedation = $ 370, total: $ 1580)
Arriving for the surgery in the morning, Dr. Lee was looking at the old panoramas (from 2010 and April 2012). I got an uneasy feeling and tried: 'we did do the CBCT'. Her response was: 'oh, did you bring it.'
It was very disconcerting to find that the surgeon was unaware of the CBCT, had not studied it, and had not had some sort of conference with Dr Chen. She could not access the CBCT images from the operating room. (Oral surgery is on the first floor, orthodontics on the third and the radiology is also on the first floor of the same building.) Besides all of that, a CBCT is not something you review scalpel in hand!
Dr Lee looked at the couple of CBCT images on my iPad. (The irony is that we initially sought this surgeon, because I saw her name connected to a paper on CBCT so I thought it was something she would think worthwhile.)
I regret that I let the surgeon operate under the circumstances. If I had known what I know now, I would have taken my son and walked out.
Sam's surgery took two hours. Surgery notes:

Post surgery on 9/21/12.
When I ask Dr. Chen for the image he replies:
I don't have the post op X-rays, so you will have to ask Dr. Lee.
Dr Lee commented after the operation about how she had had to remove a lot of debris that looked like filling material around the two canines. She found damage to the crowns of #6 (1/3 of the crown) and also #27 (1/4 of the crown). The origin of this was unclear, but she seemed to suspect surgeon #1 and iatrogen damage. I commented that x-rays in 2010 showed an irregular upper canine prior to the first operation. Surgeon #2 then said said that it was probably bits of the baby teeth roots that had been left behind when extracted.
She said there was absolutely no way that the trauma to the upper front teeth could have affected the permanent canines causing the damage to the crowns of the canines on the right side. When asked, she said that the pulp was not exposed. The surgeon also criticized where the surgeon #1 had made his incision, "not standard", and the original direction of traction.
Unfortunately, the surgeon did not take a biopsy even though she evidently was taken a back by the resorption she found clinically. Dr. Hossaini writes in the 'Surgical Treatment of Impacted Teeth Other than Third Molars' (2)(from the title you can deduct it is from an oral surgeon's point of view, I don't think an orthodontist would talk about 'impacted canines' like that):
Identification of pathological findings such as cysts or tumors is critical, since the differential diagnosis of
these findings can dictate overall patient management. large lesions can often irreversibly affect the eruption
of a tooth or its longterm prognosis. The treatment may range from a simple biopsy during the surgical
exposure to complete resection of the affected area, including the impacted tooth.(p 261)
(Sam's dentist was very upset to hear that the baby teeth roots had been implicated and wanted to discuss surgeon #2's interpretation. He tried calling surgeon #2, who did not return his call.)
New try with traction
The good news was that the teeth passed 'the wiggle test', did not hear about the 'tap test', and that an explanation for the teeth not moving could be that the chains were loose/not attached properly. The frustrating part, that we had lost 11 months pulling on teeth hopelessly). I asked why the chains would not come out when you pulled on it, if they were not attached, but the reply was that 'that was hard to tell'.
Dr Chen started traction again, using 'fishlines' to get at the teeth from a new angle.
At Sam's visit on November 30th, a renewed x-ray showed indications according to Orthodontist #2 that both the upper and lower canines were beginning to move (hooray!?).

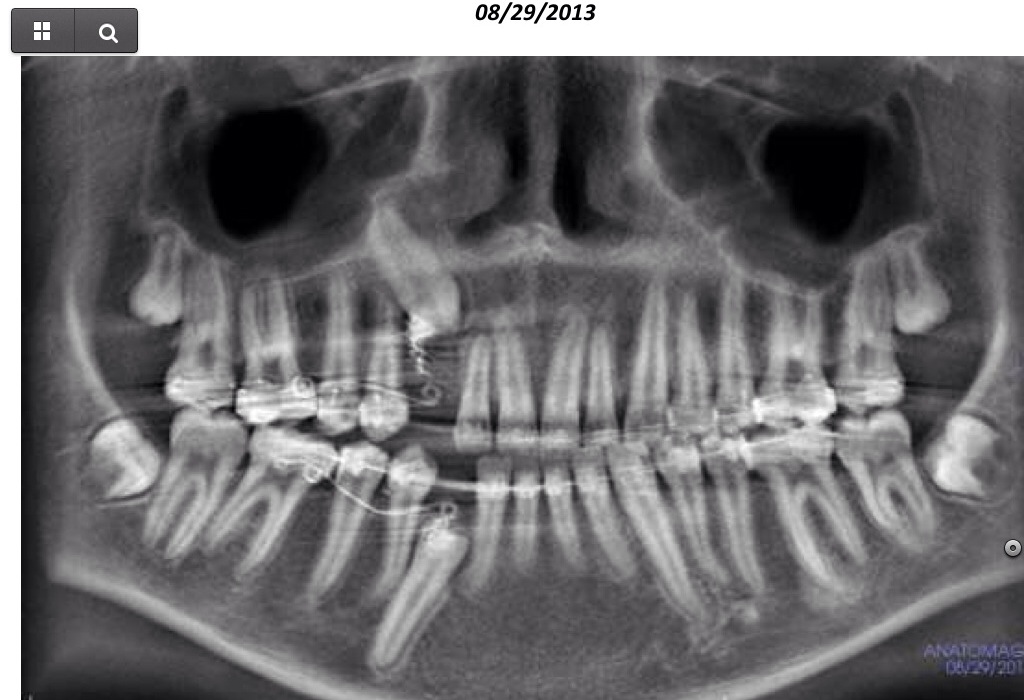
Nov 30, 2012. Sam is 14 years and 9 months.
|

Nov 30, 2012
|
Feb 24, 2013
|

|
Visit March 8, 2013: Disappointment and Reevaluation
New x-ray showed no progress, since Nov 30, 3 months ago.Very disappointing. Instead of 5 week intervals between appointments and applying tension, we are now going with 3 weeks, and pulling a bit more outward.
Seems to be a big disadvantage that the progress of pulling cannot be reliably followed by counting the number of links taken off a chain. After the first operation, October 2011, there were links taken off at the beginning of traction, but then, the x-ray in April showed no radiological evidence of of any change before and after traction.
After the second operation, September 2012, until November 2012, the canines did move, but then stopped.
Sam has the special case of his canines, for some reason, having damaged crowns, which might make the attachment to the canine come lose over time? Are the crowns resorbing further? Should they be repaired in situ?
(Dr Lee thinks that Dr Tso damaged the crown of the canines in 2011, or that they were damaged by roots of baby teeth left behind at the time of extraction. She conclusively ruled out the trauma in 2006. The dentist who pulled the teeth in 2009, thinks it is definitely the trauma. The damage to the upper canine appear on x-ray in 2010).
New x-ray showed no progress, since Nov 30, 3 months ago.Very disappointing. Instead of 5 week intervals between appointments and applying tension, we are now going with 3 weeks, and pulling a bit more outward.
Seems to be a big disadvantage that the progress of pulling cannot be reliably followed by counting the number of links taken off a chain. After the first operation, October 2011, there were links taken off at the beginning of traction, but then, the x-ray in April showed no radiological evidence of of any change before and after traction.
After the second operation, September 2012, until November 2012, the canines did move, but then stopped.
Sam has the special case of his canines, for some reason, having damaged crowns, which might make the attachment to the canine come lose over time? Are the crowns resorbing further? Should they be repaired in situ?
(Dr Lee thinks that Dr Tso damaged the crown of the canines in 2011, or that they were damaged by roots of baby teeth left behind at the time of extraction. She conclusively ruled out the trauma in 2006. The dentist who pulled the teeth in 2009, thinks it is definitely the trauma. The damage to the upper canine appear on x-ray in 2010).
:Side by side comparison: left 3/8/13 and right 11/30/12
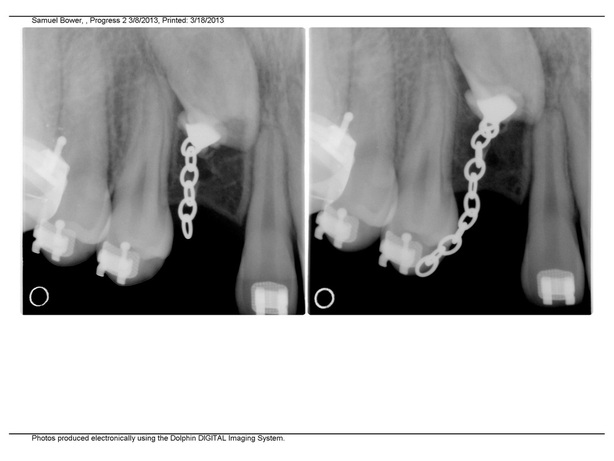

left photo: 3/8/13
right photo:11/30/12
Dr Chen said he showed Sam's case to other professors, and there were 3 different professors with 3 different opinions, (the operating surgeon#2 did not reply to the email):
- extract the teeth (then close gap with neighboring teeth or put in implant)
- try surgery for a 3rd time
- make a soft tissue exploration to visualize the tooth and maybe clear bone on the side of the tooth.
We're going for the third option = Dr Johnson.*
*Actually, as it turns out 6 months later, the upper canine is too high for this option, so I don't know why it was presented as such.
- extract the teeth (then close gap with neighboring teeth or put in implant)
- try surgery for a 3rd time
- make a soft tissue exploration to visualize the tooth and maybe clear bone on the side of the tooth.
We're going for the third option = Dr Johnson.*
*Actually, as it turns out 6 months later, the upper canine is too high for this option, so I don't know why it was presented as such.
Pulling on the chains again on April 12, 2013 compared to February 24,2013.
Visit May 7th: Dr Chen brought in Dr Earl Johnson, with the option #3: soft tissue removal, recommends thicker wire, i.e. pulling harder. Pulling a bit outwards to avoid the bone on the sides of the passage.
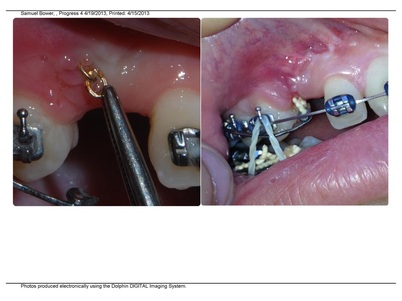
May 10th: Pain and frustration. Sam has to cut off the lower wire which has a sharp end pointing into his cheek that has been very painful.(The end of the upper wire pointed more towards the gum and did not bother him.) (Very frustrating morning and he missed his first class).
The wax provided has never helped Sam much. The sharp ends work their way through pretty much
instantly. Frankly, I can't understand why the orthodontic industry hasn't solved this problem.
Why does the end have to be sharp?
An extra trip, of 80 miles, needed to fix the sharp end.
May 10th: Pain and frustration. Sam has to cut off the lower wire which has a sharp end pointing into his cheek that has been very painful.(The end of the upper wire pointed more towards the gum and did not bother him.) (Very frustrating morning and he missed his first class).
The wax provided has never helped Sam much. The sharp ends work their way through pretty much
instantly. Frankly, I can't understand why the orthodontic industry hasn't solved this problem.
Why does the end have to be sharp?
An extra trip, of 80 miles, needed to fix the sharp end.
Instrument of torture in 21st century orthodontia:
|

|

6/21/2013
|

6/21/2013
|
Visit June 21th: Dr Chen seemed pretty sure that both teeth had been moving, and has reduced the number of links on the chain. An x-ray, though, shows that the upper canine has not budged between March and June.
Over the weekend I have reviewed all of Sam's photos and put them together on top of the page for easy viewing. There is the problem that the camera angle can fool you, but to me it seems that the upper canine actually has moved, cf: September 2011 vs April 2012, April 2012 vs September 2012, November 2012 vs March 2013. ?
Visit July 19 . Seems the lower canine is almost about to erupt and is going to be a success according to Dr Chen. The upper canine more frustrating, and the orthodontist less enthusiastic. Dr Chen: The upper canine is not ankylosed -proven by the fact that it is not pulling on the other teeth and misaligning the bite, it is moving, albeit very hesitantly. No clear answer as to why it is not moving faster. I guess the factors influencing the progress would be: stiffness of wire, or the force; the angle and direction of the force; and some kind of obstruction in the passage. The orthodontist also remarked on the little hook at the end of the root. No recent photos of the root end of the tooth.
Email July 2. Asking Dr Chen about Dr Johnson's soft tissue operation I get the answer:I just spoke with him today. He said it looks fine. We will eventually need to open a little more space, but for now it is ok
Visit July 29: Dr. Johnson and Dr. Chen. Orthodontists feel that the upper canine has made too little progress since expose and bond in September 2012. They feel that having Sam in braces too long might end up harming the the teeth (I'm not sure quite in which aspect? enamel damage? decalcification? caries?). Last effort is a referral to a UCSF oral surgeon for 'reexpose' and possible luxation.
August 3, email to Dr. Chen: Found this article.http://www.dr-adrianbecker.com/page.php?pageId=281&nlid=59
Does it have any bearing on Sam's case?
No response from Dr Chen.
August 5, email to Dr. Chen where I forward Dr. Becker's response from below on PEIR.
Dr Chen's response: It's pretty interesting.
August 21, email asking Dr. Chen about his opinion on PEIR. His response: I will have to
familiarize myself with intracoronal resorption, but there is a very high possibility that it is going on here.
Dr. Chen cancels our appointment for the 23rd and is then on some kind of leave.
Pre-eruptive intracoronal resorption?
(for more on PEIR and resorption, just click)
I read the July newsletter by Dr. Adrian Becker. 'Pre-eruptive intracoronal resorption' (http://www.dr-adrianbecker.com/page.php?pageId=273). Can't say I understand it enough to know if it is relevant to Sam's case, but have not really received a good explanation to why his impacted two canines are damaged the way they are and if this is somehow a reason why they are impacted. I wrote orthodontist #2, no answer, so I emailed Dr. Becker in Jerusalem and had a response within a couple of hours! See Dr. Becker's response below:
Over the weekend I have reviewed all of Sam's photos and put them together on top of the page for easy viewing. There is the problem that the camera angle can fool you, but to me it seems that the upper canine actually has moved, cf: September 2011 vs April 2012, April 2012 vs September 2012, November 2012 vs March 2013. ?
Visit July 19 . Seems the lower canine is almost about to erupt and is going to be a success according to Dr Chen. The upper canine more frustrating, and the orthodontist less enthusiastic. Dr Chen: The upper canine is not ankylosed -proven by the fact that it is not pulling on the other teeth and misaligning the bite, it is moving, albeit very hesitantly. No clear answer as to why it is not moving faster. I guess the factors influencing the progress would be: stiffness of wire, or the force; the angle and direction of the force; and some kind of obstruction in the passage. The orthodontist also remarked on the little hook at the end of the root. No recent photos of the root end of the tooth.
Email July 2. Asking Dr Chen about Dr Johnson's soft tissue operation I get the answer:I just spoke with him today. He said it looks fine. We will eventually need to open a little more space, but for now it is ok
Visit July 29: Dr. Johnson and Dr. Chen. Orthodontists feel that the upper canine has made too little progress since expose and bond in September 2012. They feel that having Sam in braces too long might end up harming the the teeth (I'm not sure quite in which aspect? enamel damage? decalcification? caries?). Last effort is a referral to a UCSF oral surgeon for 'reexpose' and possible luxation.
August 3, email to Dr. Chen: Found this article.http://www.dr-adrianbecker.com/page.php?pageId=281&nlid=59
Does it have any bearing on Sam's case?
No response from Dr Chen.
August 5, email to Dr. Chen where I forward Dr. Becker's response from below on PEIR.
Dr Chen's response: It's pretty interesting.
August 21, email asking Dr. Chen about his opinion on PEIR. His response: I will have to
familiarize myself with intracoronal resorption, but there is a very high possibility that it is going on here.
Dr. Chen cancels our appointment for the 23rd and is then on some kind of leave.
Pre-eruptive intracoronal resorption?
(for more on PEIR and resorption, just click)
I read the July newsletter by Dr. Adrian Becker. 'Pre-eruptive intracoronal resorption' (http://www.dr-adrianbecker.com/page.php?pageId=273). Can't say I understand it enough to know if it is relevant to Sam's case, but have not really received a good explanation to why his impacted two canines are damaged the way they are and if this is somehow a reason why they are impacted. I wrote orthodontist #2, no answer, so I emailed Dr. Becker in Jerusalem and had a response within a couple of hours! See Dr. Becker's response below:
I think your tale of impacted canine treatment is quite remarkable, but I think that Sam's courage and tenacity are even more so!
Comparisons of radiographs taken by different methods - panoramic compared with periapical views and even periapical views compared with other periapical views - is notoriously misleading, since the angle of the x-ray cone is not standardized and movement of the teeth may well be more virtual than actual. From the series of views that you have illustrated, I see little or no movement in either tooth.
As far as my July 2013 bulletin is concerned, I do believe that both canines have undergone 'pre-eruptive intracoronal resorption', and it is entirely possible that this was due to the 2006 trauma. As I wrote in the bulletin, it is generally believed (but not certain) that the resorptive initiation is through an enamel defect in the crown formation which, when it occurs (which is rarely), it is likely to affect the tips of the crowns of permanent canines - as we see here and as I illustrated in the bulletin. Having noted that, does it stop eruption? Apparently not, at least not in my limited experience. Furthermore, having surgically exposed the tooth, the lifeline of the lesion will have been interrupted but closing off the surgical wound completely, without at least filling the resorbed area, will then likely re-ignite the resorption process. This means that the resorption process may still be eating away at the inside of the crown of the tooth. However, it is unlikely to affect the dental pulp - as explained in the bulletin.
From the orthodontic point of view, space has been provided adequately for both teeth and traction has clearly been applied with little complexity. Furthermore, the direction of traction appears to have been correct.
So, in the absence of any other explanation why the teeth have not moved, I have to go with the idea that 'pre-eruptive intracoronal resorption' may indeed prevent movement. That being the case, we now have to look at September's renewed exposure adventure a little differently. I use the word adventure, because the entire raison d'etre or modus vivendi of the advice here is based on this questionable assumption.
My advice to the surgeon, therefore, is as follows:-
1. expose the two canines, check the adequacy of the bond and remove any adhesions of tissue (possibly scar tissue) from the crowns of the teeth, but not to extend the exposure into the CEJ area, at the join between crown and root.
2. identify and superficially clean the mush from the resorbed area of the crown - but not to extend the cavity excavation deeper. Most important: absolutely to leave the deeper area of mush untouched, for fear of exposing the vital pulp. Restore the crown with composite material, to seal off the cavity from the surrounding tissues. While I have no problem with the surgeon checking for mobility of the tooth at this stage, I would argue strongly against his/her pushing elevators down the PDL along the root surface, since this will almost certainly cause an ankylosis, if not already present (there are no signs at present).
3. re-suture the full flap back into place. As the orthodontist, I would want to be present at the surgery, to apply immediate traction to both teeth simultaneously, as before, using vertical intermaxillary elastics to support the anchorage and, thereby, avoid intrusion of adjacent teeth.
4. Depending on the method of traction and its power range will depend how frequently Sam should be seen and you should be guided by the orthodontist in this.
5. I would expect to see positive results within 3-4 months. If nothing happens, then the teeth should be extracted.....in which case, I would like you to have them photographed and sent to me (please!) - or, better still, place them in formalin and send them to me for further examination. If they do move, please tell me. It may help someone else, since I will have learned something new!
CEJ= cemento-enamel junction
PDL= periodontal ligament
The good and the bad??? Definitely bad that Dr. Becker sees "little or no movement" over the past year! Sam's orthodontist suggested a new CBCT that could be compared with the old one to get a better idea of movement.
The anniversary of the second expose&bond is now in September. Good that it seems worthwhile to do a third surgery. Unfortunately, 'pre-eruptive intracoronal resorption' is a diagnosis that Sam's orthodontists and surgeons so far, are not familiar with.
Orthodontist #2 comments on PEIR saying it is "pretty interesting", more than two weeks later he has yet to 'familiarize' himself with the condition.
The science: Pre-eruptive intracoronal resorption (see 'resorption' section)
It is interesting to note that ICCR is a known cause for impeding eruption (see Becker on PEIR), but for PEIR,
it is not yet known if it does or doesn't.
Since PEIR has been a known condition for a long time, but simultaneously neglected and referred to as
a rariety (although it seems that that the very rareness could possibly actually be false). The scarce examples of case studies that I can find , and the total neglect of this diagnosis, makes it hard to know if there is any relation between PEIR and impacted teeth. It's incredibly unfortunate that Sam should have a double whammy of PEIR and
impactation, and that it apparently is an undocumented situation.
I am surprised that a University Clinic isn't finding Sam's case more interesting, there should be a paper in there for somebody. Only Dr. Becker is interested enough to want the canines if they are extracted, to advance science.
Dr. Becker in his response is willing to go along with the presumption that there is a connection between impaction and resorption ("in the absence of any other explanation why the teeth have not moved, I have to go with the idea that PEIR may indeed impair movement") and he recommends a third operation.
I was quite distressed that after having asked several orthodontists, including university professors, and 3 oral surgeons about the resorption going on in Sam's canines since 2010, I have to diagnose the condition myself. Needless to say, no one has ever mentioned the need for an endodontist. The articles on PEIR I find talk about lining the cavities with hydroxylapatite, as I understand it, to protect the pulp from resorption, which Sam's surgeons did not do.
Dr Gerald Nelson
|
Dr Chen vanishes abruptly, New UCSF Orthodontist , Dr Gerald Nelson
Dr. Nelson's treatment notes Dr Chen cancels our August 21st appointment and disappears because of a sudden 'restructuring of the clinic', then it was 'personal'. Visit August 23, 2013: Dr. Nelson says PEIR is a rare condition, and he is not surprised that orthodontists are not familiar with it. In my view, if you have a patient presenting with an unusual condition, what justifies not trying to find out what is, and if it could be the reason why treatment is not working? (I previously tried googling 'trauma', 'resorption', 'crown damage'..., but an orthodontist should be better equipped at finding PEICR if they made the effort. It actually seems to me that it might not be a rare conditon at all, just neglected). The plan now is a second CBCT to decide the basic fact: if the canines have moved or not the last 12 months. |

Tugging along
|
(I'm a bit sceptical since I've never heard the evaluation of the first CBCT. Orthodontist # 2, said it was made for the operating surgeon, but she did not see them before the operating room, when she gave the few pictures on my iPad a perfunctory look.)
Now, the CBCT will tell if the teeth have moved, and give a view of the surfaces of the canines. If the teeth have moved, the orthodontists wants to keep pulling. I hope the CBCT will be useful (it's some 30 microsiewerts,
$ 388, and a 3-4 hour round trip to SF), Dr. Becker did not mention any indication for a CBCT, just the surgery performed according to his tips.
I am worried since the pulp of the canines has not been sealed up, and there are cases where the teeth erupt, but are destroyed to the point that they are not deemed viable, and have to be extracted anyway. If that would be the outcome after 3 years of braces, it would be quite devastating!
Now, the CBCT will tell if the teeth have moved, and give a view of the surfaces of the canines. If the teeth have moved, the orthodontists wants to keep pulling. I hope the CBCT will be useful (it's some 30 microsiewerts,
$ 388, and a 3-4 hour round trip to SF), Dr. Becker did not mention any indication for a CBCT, just the surgery performed according to his tips.
I am worried since the pulp of the canines has not been sealed up, and there are cases where the teeth erupt, but are destroyed to the point that they are not deemed viable, and have to be extracted anyway. If that would be the outcome after 3 years of braces, it would be quite devastating!
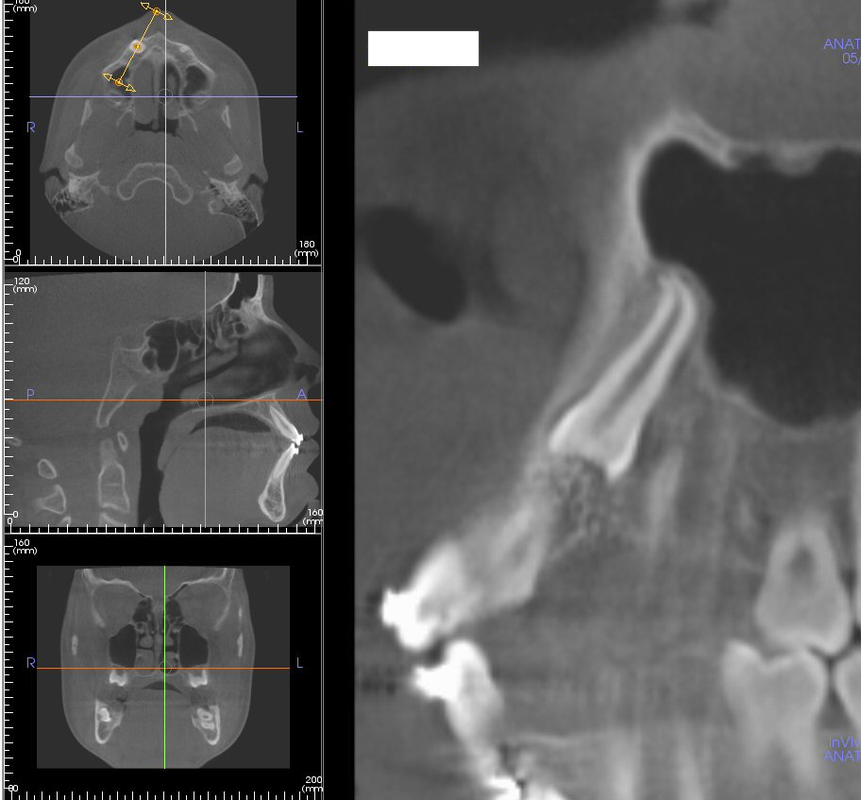
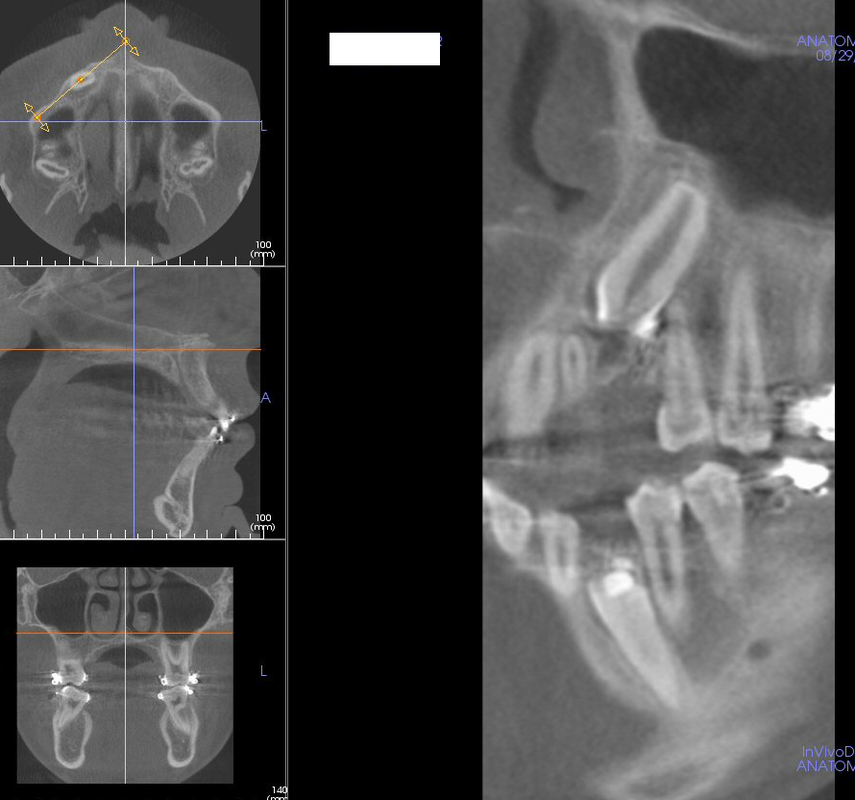
CBCT #2, 8/29/13
15 µSiv for Sam according to technician.
Dr. Nelson never wrote the referral for the CBCT, the desk had to scramble to find another orthodontist who could put in the referral. Couldn't have been easy, since our meeting with Dr. Nelson and the decision to make a CBCT wasn't documented in the journal.
I talked with the radiology technician. Apparently, at the time of Sam's operation, a year ago, the departments of orthodontics and oral surgery did not want to share information and have the x-rays readily accessible, it sounded like x rays risked getting lost or misplaced. Too bad for Sam. The system has since been changed. I also asked about who reviews the CBCTs. The answer was that no radiologist is involved usually. Why?
15 µSiv for Sam according to technician.
Dr. Nelson never wrote the referral for the CBCT, the desk had to scramble to find another orthodontist who could put in the referral. Couldn't have been easy, since our meeting with Dr. Nelson and the decision to make a CBCT wasn't documented in the journal.
I talked with the radiology technician. Apparently, at the time of Sam's operation, a year ago, the departments of orthodontics and oral surgery did not want to share information and have the x-rays readily accessible, it sounded like x rays risked getting lost or misplaced. Too bad for Sam. The system has since been changed. I also asked about who reviews the CBCTs. The answer was that no radiologist is involved usually. Why?
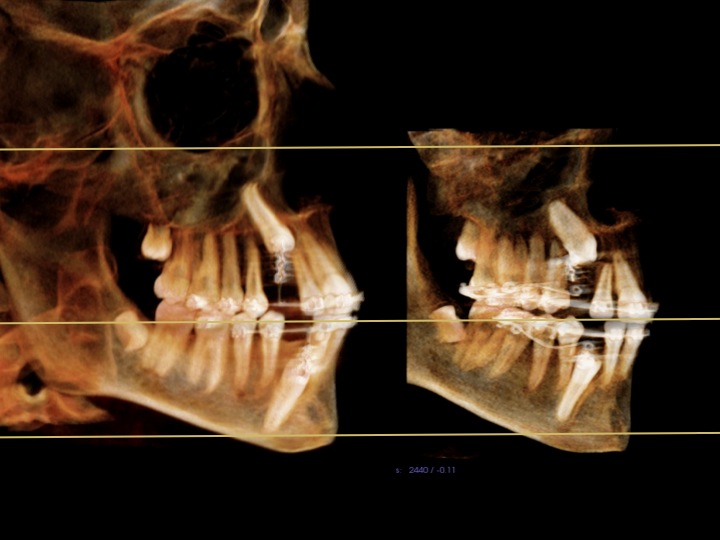
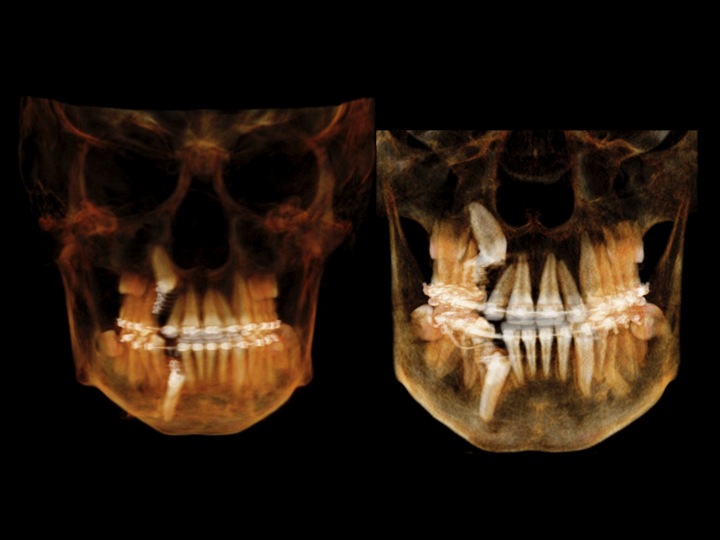
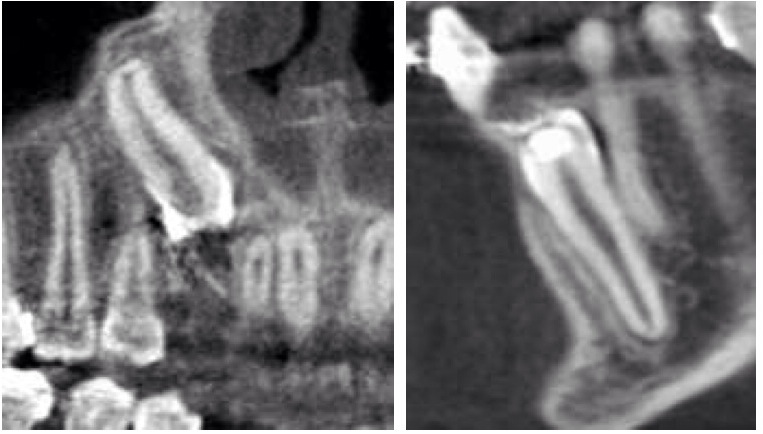
Compare left = CBCT#1 May 2012 and right= CBCT#2 September 2013
Newer CT 'fuzzier'. According to images and orthodontist#3 the teeth have moved a little, the lower more than upper. I tried resizing to make images more directly comparable.
Newer CT 'fuzzier'. According to images and orthodontist#3 the teeth have moved a little, the lower more than upper. I tried resizing to make images more directly comparable.
resized
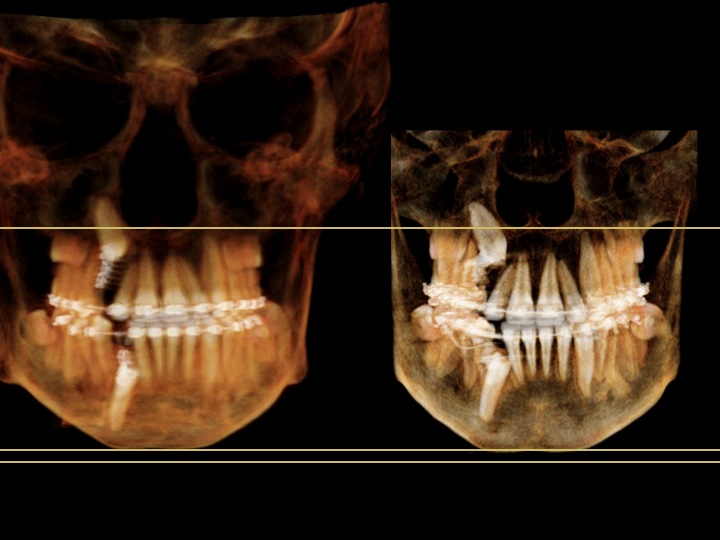
resized
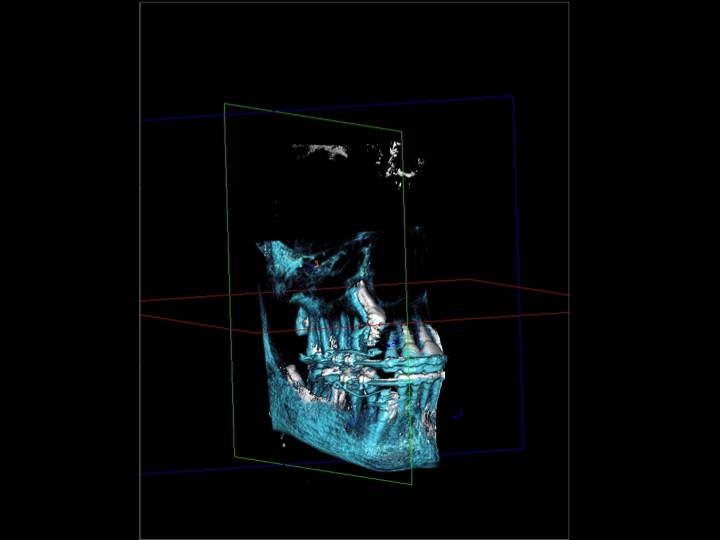
The images below are superimposed, put on top of each other. White is May 2012 and blue is August 2013
Orthodontist # 3 asks an endodontist and an oral surgeon for some team work effort:
UCSF Department of Oral Surgery
Dr Meheran Hosseini, Professor of Oral Surgery:
UCSF Department of Oral Surgery
Dr Meheran Hosseini, Professor of Oral Surgery:
I have to admit, I admire the effort to catalog all these events!!! I am not sure if I would been that interested to research this so extensively.
From my perspective, the first question should be the prognosis of this tooth and why it is not erupting. It seems like everyone more or less has done what they had to do. I won't pretend to understand the cellular pathophysiology of Intra-coronal resorption in unerupted canine. So I cannot intelligently comment if this is a really entity or not. So, before putting this kid through more intervention we should identify our treatment objectives.
If we don't think this tooth can be guided into position, then might as well leave alone. If we don't understand the etiology or cellular pathophysiology of the problem, then I am not sure if endo or restorative treatment would fix it. From the technical perspective, usually gaining access to these teeth is difficult enough, add to it restorative or endodontic procedures!? I know I personally would not be able to gain such an access to this tooth.
If we think this tooth can be guided into position, then why not perform the endodontic and restorative procedures more predictably at a later time?
Anyway, sorry if I cannot provide an intelligent answer.
UCSF Department of endodontics
Dr Jeffrey Janian, Professor of Endodontics:
Dr Jeffrey Janian, Professor of Endodontics:
Regarding the “resorption” of the unerupted #6: This includes resorption of the enamel of the crown. I have
no explanation for it. The crown of the tooth is fully formed before any root formation occurs, so I highly doubt the original trauma affected the crown of tooth #6. The shape of the “resorbed” incisal portion of #6 appears like an artificial
geometric shape, rather than a process the body creates.
I can’t say whether this is resorption or not.
Following the mother’s description of the timeline and the radiographs provided, the way I read it, the only
surgical/dental intervention before the “missing incisal portion” of the crown was: extraction of the primary
canines.
Could a bur have had contact with the incisal edge of #6 removing the primary canines? I can’t imagine this being the case, but I’ve never removed a tooth such as this or even seen it done.
Regarding: Pre-eruptive intracoronal resorption
I’ve never been exposed to this term. Never read it in a textbook or attended a presentation it was spoken of. Due to this I expect is a little know entity. (and I wasn’t sure how much more research/knowledge there is besides the case report.
Most importantly, there is nothing which can be done endodontically unless the canine is exposed. The pulp appears to be functioning properly, as the root has continued to develop. The pulp must be present, viable and healthy for the root to continue development.
So in summary, I’m not sure this is resorption. If it is, its something I’ve never heard of, where enamel is resorbed. Next, if anything endodontically needs to be done. (I’m not convinced of this), the tooth must be exposed, which seems may not be possible. (?)
As a disclaimer, I’ve not examined the patient; this is only my opinion with the knowledge I have; resorption of the enamel of a tooth is not within my area of expertise; and I’ve learned not to be surprised there are issues out there I just am not aware of.
I extend the mother and son the best hope possible.
From Dr Janian's strange description of 'artifical geometric shape' it sounds like Sam has been invaded by some alien material...
Dr. Becker's comment:
I would not consider the upper canine to be surgically inaccessible - my surgeon colleagues here in Jerusalem
would certainly undertake to expose it. I am always present at the operation to apply the directional traction
forces and that gives me an advantage.
Reading the letters from "orthodontist #3" (whom I know) and the surgeon and endodontist has not altered
my view nor my suggestions for treatment. Certainly I recognize that despite everything, it could still fail,
simply because we have all misdiagnosed the cause...... we have merely used (hopefully) intelligent
guesswork.
Dr. Becker still thinks surgery would be possible for Sam...problem is, I have no surgeon here.
As I mentioned in a previous e-mail, this is a remarkable saga, which appears to be coming to a sad finale,
for which I am genuinely sorry. As I explained in my last e-mail, I view the problem a little differently, but
who can be 100% sure of the interpretation that I have given to my observations? although there is nothing
new that convinces me otherwise. The suggestions that I made in my last e-mail remain my own preferred
direction of treatment. (Dr Becker)
|
Dilacerated root - important or not for Sam?
I asked Dr Chen after CBCT#1 what the 'hook' was at the apex of the maxillary canine. I saw it when looking over the image with the technician. Dr Chen did not expand on it, we kept referring to it as 'the hook'. I asked Dr Nelson again about 'the hook' and he said it is a dilacerated root and it is so small it has no importance in Sam's case. This morning I was looking at Dr. Becker's website and found an article on 'The "Classic" Dilacerated Maxillary Incisor' (April 2012). Dilaceration is a developmental disturbance in shape of the tooth, with an angulation, or a sharp bend or curve, in the root or crown which is thought to be due to trauma during the period in which tooth is forming. So it is usually a trauma early on, age 2 or so, but it can be left undetected, because the impact doesn't have to be that bad and can be forgotten. Sam's canines are a mystery, why does #6 have, dilaceration, enamel resorption, dentin resorption and pulp engagement, and why won't it move!? Is #27 going to move in a reasonable amount of time with enamel and dentin resorption, and pulp engagement? |

|
The importance of record keeping
Received Sam's dental record from orthodontist #3. I'm afraid they look nothing like what is described in the Guidelines for Orthodontics and Dentofacial Orthopedics 2008:
The keeping and preserving of a patient's dental record is necessary to the goal of providing high quality
orthodontic treatment. Prudent record keeping s foundation for planning and maintaining the continuity of
care.
This is how a San Francisco lawyer and dentist, Dr. Zinman, describes records.
When you go into court, you will be judged by your records. Remember the three R's of malpractice
prevention: The first is Records, the second is Records, and the third is Records. It is all three D's:
Document, Document, and Documents.(3).
Received Sam's dental record from orthodontist #3. I'm afraid they look nothing like what is described in the Guidelines for Orthodontics and Dentofacial Orthopedics 2008:
The keeping and preserving of a patient's dental record is necessary to the goal of providing high quality
orthodontic treatment. Prudent record keeping s foundation for planning and maintaining the continuity of
care.
This is how a San Francisco lawyer and dentist, Dr. Zinman, describes records.
When you go into court, you will be judged by your records. Remember the three R's of malpractice
prevention: The first is Records, the second is Records, and the third is Records. It is all three D's:
Document, Document, and Documents.(3).
How to interpret CBCT - some confusion
CBCT according to Orthodontist # 3
Initially said both canines had moved, then changed it to only #27 by 3-4 mm
#6 resorption has connection to pulp in 2012 and 2013
#27 looked like the erosion went into pulp in 2012, eyelet is in the way on the 2013 image
Initially said both canines had moved, then changed it to only #27 by 3-4 mm
#6 resorption has connection to pulp in 2012 and 2013
#27 looked like the erosion went into pulp in 2012, eyelet is in the way on the 2013 image
|
|
CBCT according to 'Beamreaders", excerpts
2012
#6's coronal coronal third has been reduced in size to a point close to the coronal portion of its root canal. No suggestive signs of pulpal exposure...
The available interproximal space for #6's proper eruption/traction was not enough due to #6's angulation/position. No suggestive signs of resorption/displacement, pathology and/or ankylosis
#27's coronal thrid has been reduced in size to a point close to the coronal point of its root canal; no suggestive signs of pulp exposure were noted, however, a thin line of enamel/dentin wall was noted at this level.
2013
#6 has similar position, root morphology and relationship
#27 moved slightly coronal and distal towards the middle root third of adjacent # 28
2012 May CBCT 2013 August CBCT
2012
#6's coronal coronal third has been reduced in size to a point close to the coronal portion of its root canal. No suggestive signs of pulpal exposure...
The available interproximal space for #6's proper eruption/traction was not enough due to #6's angulation/position. No suggestive signs of resorption/displacement, pathology and/or ankylosis
#27's coronal thrid has been reduced in size to a point close to the coronal point of its root canal; no suggestive signs of pulp exposure were noted, however, a thin line of enamel/dentin wall was noted at this level.
2013
#6 has similar position, root morphology and relationship
#27 moved slightly coronal and distal towards the middle root third of adjacent # 28
2012 May CBCT 2013 August CBCT

|
|


|
|

|

|
CBCT image by Dr. Vu
2012 on top, 2013 below.
Even though there are not exactly the same slices, Dr Vu thinks #6 has improved in the most recent image. Which seems remarkable.
2012 on top, 2013 below.
Even though there are not exactly the same slices, Dr Vu thinks #6 has improved in the most recent image. Which seems remarkable.
2012 CBCT
2013 CBCT

|
I found this one myself with Osirix.
Dropbox makes it possible to share files and CBCTs. I 'invited' specialists to look and yet again got an answer from Dr. Becker: Whether or not the resorption has stopped in the interim between 2012 and 2013 is irrelevant. The teeth are not erupting and need to be treated one way or another (i.e. extracted or erupted). I am not aware of a lesion like this ceasing its progressive destruction without outside intervention - which means cutting off its nutrient supply line. If the resorption has indeed stopped, the reason could be that the surgical exposure achieved this. As I noted earlier, by re-covering the tissues over the exposed crown, the likelihood is that the nutrient supply line will have been re-established and the progress merely temporarily interrupted and then renewed with healing. Alternatively, the lesion may have been permanently arrested, in which case its resorptive tissue will have become replaced by the surrounding connective tissue. In the absence of a follicle and with connective tissue in direct contact with the dentine, I do not know whether the tooth will respond to orthodontic traction, but probably not. Accordingly, as I see it, logic would suggest surgical re-exposure of the tooth and covering the affected part of the crown with an inert dental restoration (e.g. glass ionomer) in order to separate it from the surrounding connective tissue. This could probably be done in a closed eruption procedure, but preferably, in an open one and then to reapply orthodontic traction. |
Mistakes will come back to haunt you sometimes. Sam's September 2013 CBCT was ordered by an orthodontist scrambled up by the reception. With only Dr. Chen's scant notes to go on. Dr. Nelson did not make a note on our visit or anything on the planned CBCT. According to the technician, 15 µSv dose was used.
It turns out that the resolution isn't enough to know definitely if there is pulp involvement or not.
Apparently, Dr. Nelson did not look at the 2012 CBCT before looking at the 2013 CBCT, which seems unfortunate. If there was suspected pulp involvement in 2012, it seems that a later CBCT could have been designed to address the inadequacies of the previous one. According to Dr. Nelson's reasoning, the pulp engagment is a springing point, see below. (The only treatment that would have been recommended if Dr. Lee could have clearly shown a connection to the pulp would have been extraction)
The periapicals of #27 and #6 and the panorama done in preparation of surgery #3 gave Sam a 50 µSv.
To me it seems undesirable to reduce the dosage of a CBCT to the point where you have to make up for it
afterwards. A CBCT needs to be carefully planned and thought over!
It turns out that the resolution isn't enough to know definitely if there is pulp involvement or not.
Apparently, Dr. Nelson did not look at the 2012 CBCT before looking at the 2013 CBCT, which seems unfortunate. If there was suspected pulp involvement in 2012, it seems that a later CBCT could have been designed to address the inadequacies of the previous one. According to Dr. Nelson's reasoning, the pulp engagment is a springing point, see below. (The only treatment that would have been recommended if Dr. Lee could have clearly shown a connection to the pulp would have been extraction)
The periapicals of #27 and #6 and the panorama done in preparation of surgery #3 gave Sam a 50 µSv.
To me it seems undesirable to reduce the dosage of a CBCT to the point where you have to make up for it
afterwards. A CBCT needs to be carefully planned and thought over!
Sep 9, Dr Nelson on CBCT 2013:
I reviewed the images, and I see movement in both teeth.
Sep 27, Dr Nelson notes:
"Told that superimposing the CBCTs show little to no movement of the upper canine, and 3-4 mm of vertical progress on the lower. Told that cooperation between perio and endo at this point could allow restorative work on the lower canine (if the two specialists agree). ...Good to proceed with this, because in the CBCT it appears that the pulp canal is not involved [talking of #27], but only visual inspection will confirm that"....
Sep 27, visit (5 week intervall):
Dr Nelson now showed us images from the CBCT where it does look like the resorption has worked it's way into the pulp of tooth #6. If it had been bacterial, Sam would have had pain and other symptoms, he does not luckily.
Dr Nelson wants to concentrate on saving tooth#27 before it's too late. He plans to contact a UCSF periodontist so we can get brackets on it. Dr. Nelson explained that the 'hook' on the apex of #6, is a 'dilacerated root' , but small enough not to be of importance.
Oct 2, email Dr. Nelson:
Sees pulp engament in #6 from 2012. Wants us to find local specialist 'out of concern for our travel time'.
I reviewed the CBCT for 2012, and found that the coronal resorption in the upper did connect with the pulp at that initial image as well, and has not changed much. The erosion in the crown of the lower in the initial scan looks like it was also open to the pulp, however I can't see that in the recent CBCT. Could be the eyelet pad is in the way. I don't see that the resorption has progressed from initial to recent, so I'm thinking that if we bring the lower canine get closer to the surface, the treatment provided by the endodontist will involve less risk, since the access would be cleaner and easier. I am convinced that the lesion is sterile, as there is no sign at all of any infection or inflammatory responses. We think the chance of retaining the lower canine is still promising. Do you want to proceed with removal of the upper canine? It is not urgent, but if you do, I can arrange for a consultation with the oral surgeon.
We are concerned about your travel time. When it is time for the endodontic treatment, the procedures might require trips with fairly short turnaround. Have you looked into specialists close to home?
...
It does appear in the 2012 CBCT that there is a connection, but that does not mean Dr. Lee could have seen it. The visual during that surgery is very poor. She reported that she saw no evidence pulp exposure. The slice I found on the CBCT was not easy to locate, and suggests a connection, but remember that the resolution of detail is not super.
The only treatment that would have been recommended if Dr. Lee could have clearly shown a connection to the pulp would have been extraction, since endo at that remote location is not feasible according to the endodontists I spoke with. In any case had she probed around and physically located an opening, that would have contaminated the pulp tissue. As it is, the lesion continues to be quiet. Our recommendation continues to be remove the #6, since it is not moving, and continue to move #27 to the surface until access is safe.
Oct 25, visit (4 week intervall);
Dr Nelson cuts loose #6 because it is misaligning the other teeth.
(Compare this to July 19 when orthodontist #2 said that the fact that the neighboring teeth were not misaligned, which proved that #6 was moving, but slowly),
Treatment plan:
- Continuing moving Sam's lower right canine into the mouth
- When the tooth is available, the endodontist can evaluate the advisability of root canal therapy. If appropriate,
the root canal treatment will be done, and the enamel of the tooth restored. Then we can continue the tooth
movement.
- We will discontinue traction on the impacted #6, and recommend removing it, although this is not urgent.
Replacement of the tooth would be done by a restorative dentist. Implant placement must wait until facial
growth is complete, as the position of the implant would be negatively affected with any growth. Boys can
continue to grow past age 20.
I try getting Sam transferred from UCSF to Dr. Huang in San Leandro, whom I know to be CBCT competent.
(We originally came to UCSF thinking it was the best bet for teamwork, state-of-the art treatment, professional curiosity and CBCTcompetence, but found none of that.) Dr. Nelson says that Dr. Haung declines as long as we
are 'comfortable' at UCSF.
Sep 27, 2013 (visit note): Told that superimposing the CBCTs show little to no movement of the upper canine, and 3-4 mm of vertical progress on the lower. Told that cooperation between perio and endo at this point could allow restorative work on the lower canine…Good to proceed with this, because in the CBCT it appears that the pulp canal is not involved, but only visual inspection will confirm that.
Oct 29, email
From Dr. Nelson:
I had further consultation with Dr. Adrian Becker in Jerusalem, and spent time with Dr. Patel around Sam's current and historical condition. I have provided Dr. Patel with the CBCT. He has agreed to consult with you about the case, will consider first exposing the upper canine with the intent to remove the resorbed coronal material and placing a composite cover. If that goes well, and we can move the tooth, he will consider the same treatment for the lower. He will inform you about the caveats involved. Please call to make an appointment with Dr. Chirag Patel at the Oral and Facial Surgery Center
I reviewed the images, and I see movement in both teeth.
Sep 27, Dr Nelson notes:
"Told that superimposing the CBCTs show little to no movement of the upper canine, and 3-4 mm of vertical progress on the lower. Told that cooperation between perio and endo at this point could allow restorative work on the lower canine (if the two specialists agree). ...Good to proceed with this, because in the CBCT it appears that the pulp canal is not involved [talking of #27], but only visual inspection will confirm that"....
Sep 27, visit (5 week intervall):
Dr Nelson now showed us images from the CBCT where it does look like the resorption has worked it's way into the pulp of tooth #6. If it had been bacterial, Sam would have had pain and other symptoms, he does not luckily.
Dr Nelson wants to concentrate on saving tooth#27 before it's too late. He plans to contact a UCSF periodontist so we can get brackets on it. Dr. Nelson explained that the 'hook' on the apex of #6, is a 'dilacerated root' , but small enough not to be of importance.
Oct 2, email Dr. Nelson:
Sees pulp engament in #6 from 2012. Wants us to find local specialist 'out of concern for our travel time'.
I reviewed the CBCT for 2012, and found that the coronal resorption in the upper did connect with the pulp at that initial image as well, and has not changed much. The erosion in the crown of the lower in the initial scan looks like it was also open to the pulp, however I can't see that in the recent CBCT. Could be the eyelet pad is in the way. I don't see that the resorption has progressed from initial to recent, so I'm thinking that if we bring the lower canine get closer to the surface, the treatment provided by the endodontist will involve less risk, since the access would be cleaner and easier. I am convinced that the lesion is sterile, as there is no sign at all of any infection or inflammatory responses. We think the chance of retaining the lower canine is still promising. Do you want to proceed with removal of the upper canine? It is not urgent, but if you do, I can arrange for a consultation with the oral surgeon.
We are concerned about your travel time. When it is time for the endodontic treatment, the procedures might require trips with fairly short turnaround. Have you looked into specialists close to home?
...
It does appear in the 2012 CBCT that there is a connection, but that does not mean Dr. Lee could have seen it. The visual during that surgery is very poor. She reported that she saw no evidence pulp exposure. The slice I found on the CBCT was not easy to locate, and suggests a connection, but remember that the resolution of detail is not super.
The only treatment that would have been recommended if Dr. Lee could have clearly shown a connection to the pulp would have been extraction, since endo at that remote location is not feasible according to the endodontists I spoke with. In any case had she probed around and physically located an opening, that would have contaminated the pulp tissue. As it is, the lesion continues to be quiet. Our recommendation continues to be remove the #6, since it is not moving, and continue to move #27 to the surface until access is safe.
Oct 25, visit (4 week intervall);
Dr Nelson cuts loose #6 because it is misaligning the other teeth.
(Compare this to July 19 when orthodontist #2 said that the fact that the neighboring teeth were not misaligned, which proved that #6 was moving, but slowly),
Treatment plan:
- Continuing moving Sam's lower right canine into the mouth
- When the tooth is available, the endodontist can evaluate the advisability of root canal therapy. If appropriate,
the root canal treatment will be done, and the enamel of the tooth restored. Then we can continue the tooth
movement.
- We will discontinue traction on the impacted #6, and recommend removing it, although this is not urgent.
Replacement of the tooth would be done by a restorative dentist. Implant placement must wait until facial
growth is complete, as the position of the implant would be negatively affected with any growth. Boys can
continue to grow past age 20.
I try getting Sam transferred from UCSF to Dr. Huang in San Leandro, whom I know to be CBCT competent.
(We originally came to UCSF thinking it was the best bet for teamwork, state-of-the art treatment, professional curiosity and CBCTcompetence, but found none of that.) Dr. Nelson says that Dr. Haung declines as long as we
are 'comfortable' at UCSF.
Sep 27, 2013 (visit note): Told that superimposing the CBCTs show little to no movement of the upper canine, and 3-4 mm of vertical progress on the lower. Told that cooperation between perio and endo at this point could allow restorative work on the lower canine…Good to proceed with this, because in the CBCT it appears that the pulp canal is not involved, but only visual inspection will confirm that.
Oct 29, email
From Dr. Nelson:
I had further consultation with Dr. Adrian Becker in Jerusalem, and spent time with Dr. Patel around Sam's current and historical condition. I have provided Dr. Patel with the CBCT. He has agreed to consult with you about the case, will consider first exposing the upper canine with the intent to remove the resorbed coronal material and placing a composite cover. If that goes well, and we can move the tooth, he will consider the same treatment for the lower. He will inform you about the caveats involved. Please call to make an appointment with Dr. Chirag Patel at the Oral and Facial Surgery Center
UCSF's review of Sam's second surgery : "The operation was a success, but the patient died"
Sam's ordeal is far from over, and we have to move forward. At the same time I do want his case reviewed and I want to know where things went wrong and why. Sam has had two surgeries (and as Dr. Becker writes, even a planned surgery is a trauma) and braces for almost 3 years. I want to know why the CBCT from May 2012 wasn't properly reviewed until now. I asked for Sam's record on 9/27. I've emailed Surgeon #1 and #2 and asked for a comment. I've asked Orthodontist #3 for a treatment plan.
Both Dr James Chen and Dr Janice Lee left UCSF this fall. I've asked the UCSF Dean of the San Francisco School of Dentistry, Dr. Featherstone, to review Sam's case and help answer my questions especially as to how the 2012 CBCT and resorption could be disregarded. He thanked me for my email and then had my questions dismissed by the head of Oral surgery, Dr Anthony Pogrel:
Sam's ordeal is far from over, and we have to move forward. At the same time I do want his case reviewed and I want to know where things went wrong and why. Sam has had two surgeries (and as Dr. Becker writes, even a planned surgery is a trauma) and braces for almost 3 years. I want to know why the CBCT from May 2012 wasn't properly reviewed until now. I asked for Sam's record on 9/27. I've emailed Surgeon #1 and #2 and asked for a comment. I've asked Orthodontist #3 for a treatment plan.
Both Dr James Chen and Dr Janice Lee left UCSF this fall. I've asked the UCSF Dean of the San Francisco School of Dentistry, Dr. Featherstone, to review Sam's case and help answer my questions especially as to how the 2012 CBCT and resorption could be disregarded. He thanked me for my email and then had my questions dismissed by the head of Oral surgery, Dr Anthony Pogrel:
It appears that at the time of the surgery Dr. Lee had available three Panorex-type x-rays which I have examined and
which do appear to be adequate for the purpose of carrying out the recommended surgery. I am aware that at that time
a cone-beam CT as also available and that according to your report you did show one or two of these images to Dr.
Lee. Although I have no doubt these images did have a lot of information in them, it does not appear that this would
have changed the surgical procedure in any way. It does appear that the surgery was carried out successfully, and the
teeth were exposed, bonded, and bone removed to create a passageway for the teeth to erupt. It also appears that Dr.
Lee did use a dental elevator to assess whether the teeth were ankylosed or not, and it was her opinion that they wer
not ankylosed and therefore the treatment had a reasonable chance of success. Sam’s orthodontic resident apparently
came down to witness some of the procedure. Dr. Lee did obtain a postoperative Panorex radiograph on completion of
the surgery which certainly looks very satisfactory. Dr. Lee then saw your son for evaluation one week following the
procedure where everything appeared to be healing well, and I do not believe that he has been seen in our clinic since
that time, so I am obviously unaware of developments since then. Certainly from what I see in the records I see nothing
to indicate that treatment was carried out below the standard of care. I agree with you on the value of cone-beam CT
scans which are certainly a new technology in dentistry in. However, I think like all new technologies it is capable of
abuse and the main issue with cone-beam CT scans is the increased radiation dosage, particularly for growing children. I
am sure you are aware that the New York Times has actually had this issue on their front page on a couple of occasions
with particular reference to cone-beam CTs for pediatric dentistry and orthodontics. Like all new technologies, it must be
used judiciously and appropriately and not misused.
It is hard to understand how resorption does not influence the treatment and planning of surgery. Interesting use of "the recommended surgery", as recommended by whom? "The resident", Faculty Assistant Adjunct Professor. A surgeon does not have to busy themselves with sidetracks like resorption? How do you get around a surgeon writing ' I think one thing we should do, however, is to get a cone-beam CT and to determine the exact positioning of the teeth' and then disregarding the information?
To cite risk of radiation dosage is doubly absurd, since my question concerns an existing CBCT, ordered by orthodontist and surgeon both, but neglected. Furthermore the 2012 CBCT involved 25 µSv, the 2013 CBCT was 15 µSv, while the pointless Panorex that the surgeon did post surgery was 26 µSv.
By Dr Pogrel's reasoning Dr Lee exposed Sam to an unnecessary test with radiation, and our family charged for an expensive test.
The 'dental team' of UCSF then refuses further communication with me according to email from Orthodontist #3: "this will be the last email communication from the dental team in regards to this matter". I ask too many questions: "You asked so many questions in your response that it is really impossible to know where to start."
I never heard from back from Dr Janice Lee either, but then she never responded to communications from Sam's dentist or Dr Chen, so it seems to be the general MO.
Dr Becker specializes in analyzing 'failure' of resolving impaction; he learns from it and advances the science of orthodontics. Scientifically speaking understanding failure is as important as understanding success (patientwise
it's another matter).
Sam and canines in limbo
General quotes from around my website that are painful and poignant when I think of Sam:
The keeping and preserving of a patient's dental record is necessary to the goal of providing high quality
orthodontic treatment. Prudent record keeping is the foundation for planning and maintaining the continuity
of patient care.
A correct diagnosis and an understanding of the aetiology and dynamics of the processes involved in tooth
resorption is critical to effective management.
In my opinion, after 30 years of surgically exposing my cases with impacted cuspids, very, very few are
ankylosed. The most common operator error is insufficient removal of cortical bone necessary to preclude a
“pressure necrosis” between enamel of the erupting tooth and cortical bone during a path of eruption. The
physiologic process of bone resorption ahead of dental eruption has terminated once the dental sac has been
removed around the crown of an ankylosed tooth. Secondly, traction needs to be continuous and renewed
every 2 weeks. If eruption has not occurred in 4 months, another exposure should be performed to remove
scar tissue, expand the path of eruption created through cortical bone, ascertain possible interference with
adjacent roots, and, it is hoped, leave the impacted tooth uncovered.
Complications related to the extraction of palatally impacted canines are numerous: huge bone defects,
damage of adjacent teeth (luxation, comprised parodontium, root fractures) involvement of maxillary sinus,
neuropathies. That is why similar kind of intervention is usually a last clinical approach to ectopic upper
canines. Carried out properly and in close collaboration with a radiologist, a surgeon, and an orthodontist, it
leads to satisfactory results.
To cite risk of radiation dosage is doubly absurd, since my question concerns an existing CBCT, ordered by orthodontist and surgeon both, but neglected. Furthermore the 2012 CBCT involved 25 µSv, the 2013 CBCT was 15 µSv, while the pointless Panorex that the surgeon did post surgery was 26 µSv.
By Dr Pogrel's reasoning Dr Lee exposed Sam to an unnecessary test with radiation, and our family charged for an expensive test.
The 'dental team' of UCSF then refuses further communication with me according to email from Orthodontist #3: "this will be the last email communication from the dental team in regards to this matter". I ask too many questions: "You asked so many questions in your response that it is really impossible to know where to start."
I never heard from back from Dr Janice Lee either, but then she never responded to communications from Sam's dentist or Dr Chen, so it seems to be the general MO.
Dr Becker specializes in analyzing 'failure' of resolving impaction; he learns from it and advances the science of orthodontics. Scientifically speaking understanding failure is as important as understanding success (patientwise
it's another matter).
Sam and canines in limbo
General quotes from around my website that are painful and poignant when I think of Sam:
The keeping and preserving of a patient's dental record is necessary to the goal of providing high quality
orthodontic treatment. Prudent record keeping is the foundation for planning and maintaining the continuity
of patient care.
A correct diagnosis and an understanding of the aetiology and dynamics of the processes involved in tooth
resorption is critical to effective management.
In my opinion, after 30 years of surgically exposing my cases with impacted cuspids, very, very few are
ankylosed. The most common operator error is insufficient removal of cortical bone necessary to preclude a
“pressure necrosis” between enamel of the erupting tooth and cortical bone during a path of eruption. The
physiologic process of bone resorption ahead of dental eruption has terminated once the dental sac has been
removed around the crown of an ankylosed tooth. Secondly, traction needs to be continuous and renewed
every 2 weeks. If eruption has not occurred in 4 months, another exposure should be performed to remove
scar tissue, expand the path of eruption created through cortical bone, ascertain possible interference with
adjacent roots, and, it is hoped, leave the impacted tooth uncovered.
Complications related to the extraction of palatally impacted canines are numerous: huge bone defects,
damage of adjacent teeth (luxation, comprised parodontium, root fractures) involvement of maxillary sinus,
neuropathies. That is why similar kind of intervention is usually a last clinical approach to ectopic upper
canines. Carried out properly and in close collaboration with a radiologist, a surgeon, and an orthodontist, it
leads to satisfactory results.
Oct 2, 2013 (Dr Nelson email): “I reviewed the CBCT for 2012, and found that the coronal resorption in the upper did connect with the pulp at that initial image and has not changed much. The erosion in the in the crown of the lower in the initial scan looks like it was also open to the pulp, however I can’t see that in the recent CBCT. Could be the eyelet pad is in the way.
…
It does appear in the 2012 CBCT that there is a connection, but that does not mean Dr. Lee could have seen it. The visual during that surgery is very poor. She reported that she saw no evidence pulp exposure.
Oct 23, 2013 (Dr Nelson note): Consult with Dr. Chirag Patel. Reviewed records. He recommends ext #6. Says that surgical exposure now would infect the pulp. He can remove #6 when needed.
Oct 28, 2013 (Dr Nelson visit notes): Gave family…Beam Reader Report. Parents note that Radiology report suggests traction vector could be improved – told that we had changed the vector favorably several visits ago. Told my recommendation is to suspend traction for now and #6 will need to be removed, but not urgent. We will continue to move #27 until close enough to the surface to get an endo consult.
Oct 29 2013 (Dr Nelsonemail): I communicated with Dr. John Huang in San Leandro. He recommends that at this time you continue Sam's treatment at UCSF for the time being if you are comfortable doing so.
Nov 13, Dr Nelson notes: Dr E [Radiologist Dr Eraso] ...why#6 is not moving. Dr E thinks it might be vector related, and he will construct a digital proposal.
Nov 18, email:
Dr. Pogrel will not let Dr. Patel operate on Sam. We are without surgeon.
Dr. Pogrel will not let Dr. Patel operate on Sam. We are without surgeon.
Nov 21, concerning pulp involvement:
I tried, unsuccessfully, to get a consensus on pulp involvement or no pulp involvement:
Dr Nelson:
This is an unusual situation in that the canal seems to be continuous, but we don't know whether the stuff in the crown of the tooth has a vascular connection with the pulp. There is no sign of infection.
That is what brings uncertainty both in the diagnosis and how to proceed.
Dr Eraso:
I have to agree with Dr. Nelson, the good news is that there is no signs of an inflammatory process surrounding the canines. As far as connection and pulp exposure, it is very difficult to be certain unless the surgeon at the time of the surgery/canine exposure saw signs of it.
Radiographically, the ability of recognizing a thin layer of enamel/dentin, if any most likely is compromise by many factors (e.g. CBCT resolution, metal artifacts, etc).
Since it does not make any sense to explore the área surgically to find out and I believe that radiographically there is not clear evidence of coronal pulp exposure, I recommend to monitor the area for changes, if any.
Nov 22, 2012, visit (4 week intervall):
Dr. Nelson gives up on #27, because it has moved 'half a mm' in the three months since Dr. Nelson started on Sam. (Considering that it took 1.5 years to go 3 mm, that sounds about right.)
(Dr. Nelson is looking for a surgeon outside of UCSF who can root fill #27. Do you root fill, if there is no pulp involvement?)
Dec 10: We are still waiting to hear from Dr. Nelson about what the surgeon he contacted over 2 weeks ago said, or what we are going to do. Sam is in limbo.
Meanwhile:
I found an interesting article on 'apicotomy' (http://www.hindawi.com/crim/dentistry/2013/168232/):
'Apicotomy as Treatment for Failure of Orthodontic Traction" describes a case of a 10-year-old Brazilian girl with a dilacerated root on her impacted canine, and 'probably apical ankylosis'. After 'an apical fracture' the tooth could be moved into position.
I found another article on piezoelectric surgery http://www.docvadis.it/vittoriogrenga/document/vittoriogrenga/chirurgia_canini_inclusi/fr/metadata/files/0/file/articolo%20piezo.pdf
A precise surgical cut is extremely important when the crown of a palatally impacted max- illary canine is close to the roots
or crowns of the central and lateral incisors, as often occurs. Traditional burs do not distinguish between the min- eralization
and hardness of the bone, the radicular cementum, and the enamel. Piezoelectric surgery is precise enough to account for
such differences, thus avoiding damage to the adjacent teeth.
It is reassuring to read that there are studies, research, and advancements going on. I could only wish that Sam could benefit from it.
Dec 11: I tried Dr Nelson for a third time, and he responded that he thought that he had already responded that Dr. Berger in Berkeley was not interested in the surgery, "the literature is not very strong and he has no experience"...We will have to discuss the option of removing the impactions.
Dec 12: Dr Nelson: I'll let you know as soon as I have a recommendation for you.
Dec 12: The OMFS desk says Dr. Nelson wants Sam to see Dr. Hossaini. (?).
Dec 12, 14, 16, 17 I try to find out from Dr Nelson what Dr. Hossaini can do for Sam.
Dec 17: Dr Nelson: writes we might benefit from Dr. Hossaini's advice.(?)
I tried, unsuccessfully, to get a consensus on pulp involvement or no pulp involvement:
Dr Nelson:
This is an unusual situation in that the canal seems to be continuous, but we don't know whether the stuff in the crown of the tooth has a vascular connection with the pulp. There is no sign of infection.
That is what brings uncertainty both in the diagnosis and how to proceed.
Dr Eraso:
I have to agree with Dr. Nelson, the good news is that there is no signs of an inflammatory process surrounding the canines. As far as connection and pulp exposure, it is very difficult to be certain unless the surgeon at the time of the surgery/canine exposure saw signs of it.
Radiographically, the ability of recognizing a thin layer of enamel/dentin, if any most likely is compromise by many factors (e.g. CBCT resolution, metal artifacts, etc).
Since it does not make any sense to explore the área surgically to find out and I believe that radiographically there is not clear evidence of coronal pulp exposure, I recommend to monitor the area for changes, if any.
Nov 22, 2012, visit (4 week intervall):
Dr. Nelson gives up on #27, because it has moved 'half a mm' in the three months since Dr. Nelson started on Sam. (Considering that it took 1.5 years to go 3 mm, that sounds about right.)
(Dr. Nelson is looking for a surgeon outside of UCSF who can root fill #27. Do you root fill, if there is no pulp involvement?)
Dec 10: We are still waiting to hear from Dr. Nelson about what the surgeon he contacted over 2 weeks ago said, or what we are going to do. Sam is in limbo.
Meanwhile:
I found an interesting article on 'apicotomy' (http://www.hindawi.com/crim/dentistry/2013/168232/):
'Apicotomy as Treatment for Failure of Orthodontic Traction" describes a case of a 10-year-old Brazilian girl with a dilacerated root on her impacted canine, and 'probably apical ankylosis'. After 'an apical fracture' the tooth could be moved into position.
I found another article on piezoelectric surgery http://www.docvadis.it/vittoriogrenga/document/vittoriogrenga/chirurgia_canini_inclusi/fr/metadata/files/0/file/articolo%20piezo.pdf
A precise surgical cut is extremely important when the crown of a palatally impacted max- illary canine is close to the roots
or crowns of the central and lateral incisors, as often occurs. Traditional burs do not distinguish between the min- eralization
and hardness of the bone, the radicular cementum, and the enamel. Piezoelectric surgery is precise enough to account for
such differences, thus avoiding damage to the adjacent teeth.
It is reassuring to read that there are studies, research, and advancements going on. I could only wish that Sam could benefit from it.
Dec 11: I tried Dr Nelson for a third time, and he responded that he thought that he had already responded that Dr. Berger in Berkeley was not interested in the surgery, "the literature is not very strong and he has no experience"...We will have to discuss the option of removing the impactions.
Dec 12: Dr Nelson: I'll let you know as soon as I have a recommendation for you.
Dec 12: The OMFS desk says Dr. Nelson wants Sam to see Dr. Hossaini. (?).
Dec 12, 14, 16, 17 I try to find out from Dr Nelson what Dr. Hossaini can do for Sam.
Dec 17: Dr Nelson: writes we might benefit from Dr. Hossaini's advice.(?)
In San Jose's History Park there is a turn-of-the-19th-century dental office with scary instruments and a chair with leather straps to hold the arms and legs in place, supposedly for when the pain would make it hard for the patient to stay in place. Dentistry has advanced, but when I read the preface to Dr. Becker's opus magnum, from my Bay Area experience, I must say that Dr. Becker is being overly optimistic of where orthodontics is today (my red):
in the light of research and the advent of new technology. These two factors have encouraged the
orthopedic specialist to be more discerning in the diagnosis of pathology and more innovative and
resourceful in the application of directional. Mistaken positional diagnosis and surgical blunders have become
less frequent. At the same time, they have permitted the orthodontist to become more adventurous and to
successfully apply his/her knowledge and experience to treatment of cases where previously the tooth would
have been scheduled for extraction. If this third edition may yet contribute to the furtherance of this
favorable trend in any way, I will consider my mission will have been accomplished.(1)
This is the Silicon Valley, the heart of innovation, experimentation, cutting edge of most everything, but I have not found anyone 'adventurous' enough to try to save Sam's canines. The technology, CBCT, is not standard at UCSF for impacted canines in 2013. When presented with an odd case of resorption nobody bothers researching the implications and what it means for the successful treatment of an impacted tooth. It turns out, in the here and now, at UCSF, it is still extraction that is the end result.
I can see no signs when I google around the US orthodontist/ oral surgery offices, that there is anyone considering doing what Dr. Becker advocates as best practice: the orthodontist and surgeon work as a team during surgery. Standard orthodontic practice is to send the patient off for surgery, and come back for traction in
one or two weeks. Not even at universities, where departments are located in the same building.
in the light of research and the advent of new technology. These two factors have encouraged the
orthopedic specialist to be more discerning in the diagnosis of pathology and more innovative and
resourceful in the application of directional. Mistaken positional diagnosis and surgical blunders have become
less frequent. At the same time, they have permitted the orthodontist to become more adventurous and to
successfully apply his/her knowledge and experience to treatment of cases where previously the tooth would
have been scheduled for extraction. If this third edition may yet contribute to the furtherance of this
favorable trend in any way, I will consider my mission will have been accomplished.(1)
This is the Silicon Valley, the heart of innovation, experimentation, cutting edge of most everything, but I have not found anyone 'adventurous' enough to try to save Sam's canines. The technology, CBCT, is not standard at UCSF for impacted canines in 2013. When presented with an odd case of resorption nobody bothers researching the implications and what it means for the successful treatment of an impacted tooth. It turns out, in the here and now, at UCSF, it is still extraction that is the end result.
I can see no signs when I google around the US orthodontist/ oral surgery offices, that there is anyone considering doing what Dr. Becker advocates as best practice: the orthodontist and surgeon work as a team during surgery. Standard orthodontic practice is to send the patient off for surgery, and come back for traction in
one or two weeks. Not even at universities, where departments are located in the same building.
Dr Heithersay, professor of Endodontics, on PEIR and transplantation
Dec. 14:
I asked orthodontist #2 about transplantation this spring, he smiled and said 'no', I did not know that meant that 'no, not at UCSF', but other places do it.
I wrote Dr. Heithersay at at the Department of Endodontics in Adelaide, Australia, an expert on resorption
and received this reply:
Dec. 14:
I asked orthodontist #2 about transplantation this spring, he smiled and said 'no', I did not know that meant that 'no, not at UCSF', but other places do it.
I wrote Dr. Heithersay at at the Department of Endodontics in Adelaide, Australia, an expert on resorption
and received this reply:
In our endodontic clinic we have treated two cases with similar histories of frustrated orthodontic treatment where no movement could be activated despite similar coronal exposure as that carried out for Sam . One of these cases also had pre-eruptive invasive coronal resorption. After a multidisciplinary consultation involving an orthodontist, and a peridontist and our endodontic group, it was decided in both cases to treat the unerupted teeth be intentional transplantation, with concurrent treatment of the resorptive defect and endodontic treatment in the case with pre-eruptive invasive coronal resorption. The teeth were very carefully removed surgically with special attention to avoid damage to the root surface. Before the teeth were transplanted into a newly created socket site, the root sufaces were treated with Emdogain and after transplantation, the bone defect was filled with a combination of Bio-oss and Collagen and the area was then covered with Bioguide which is a resorbable membrane. In the tooth without the pre-eruptive invasive coronal resorption, endodontic treatment was commenced prior to the transplantation, but an intra-canal dressing was placed incorporating a cortico-steroid antibiotic combination as this has been shown to control potential reesorption. The tooth will be root filled after some weeks. |
You may be able to buy on Amazon his book dealing with this topic. We believe that the methods we have used which have incorporated some recently developed additional biological materials. |
|
I asked Dr Heithersay about the degree of root formation in the transplantaion cases, since Dr. Pamela L. Alberto in SROMS where she states: "Canine transplantation should be planned when the root is 50% to 75% formed...Transplantation of the mandibular canine can also be successful if the apex of its root has not closed."
(http://selectedreadingsoms.com/wpcontent/uploads/2012/03/Alberto19.3.pdf)
Dr. Heithersay's answer:
(http://selectedreadingsoms.com/wpcontent/uploads/2012/03/Alberto19.3.pdf)
Dr. Heithersay's answer:
While planned transplantation of teeth is ideally done before the completion of root development as stated by Dr Alberto- the reason being that such teeth can continue root development in their new site and endodontic treatment can usually be avoided. All the main research related to this procedure can be found in the references I have already sent to you. However this does not preclude transplantation of a tooth with completed root development- but endodontic treatment as part of the process is indicated. This can either be carried out on the extracted tooth before transplantation, with great care not to damage the periodontal ligament. Alternatively it is carried out within approximately 2 weeks post transplantation. In both our cases, it was carried out prior to transplantation, but an intra-canal dressing was placed in both instances and the final root filling delayed for several weeks.
I guess you have already explored the possibility of extracting the unerupted teeth and closing the spaces orthodontically. Premolars can, with a little anatomical modification, successfully provide an aesthetic and functional solution.
Dr. Becker thinks that Sam's resorption is akin to ICCR (Invasive Cervical Root resorption):
The crown resorption that has occurred is due to clastic cells whose origin is the PDL and not the pulp. I see it as analogous in
virtually every detail to invasive cervical root resorption (ICRR) that we published in the Angle Orthodontist earlier this year
(Becker A, Abramovitz I, Chaushu S. Failure of treatment of impacted canines associated with invasive cervical root resorption.
Angle Orthodontist, 2013,83:870-876) and was the subject of our presentation at the AAO meeting in Hawaii last year (it's on
the disk from the meeting). Additionally, pre-eruptive crown resorption was the subject of the July 2013 Bulletin on my
website athttp://www.dr-adrianbecker.com/page.php?pageId=273This is not caries, but resorption. According to the research
(see list of refs in that article), it attacks the body of the dentine but stops short at the predentine, which has a much higher
organic content and probably does not actually get through to expose the pulp. The diagnosis that there is an open connection
was presumably made radiographically, which must be viewed with some suspicion. If the resorption mush is cleared away
meticulously, as if it were caries, instrumentation will certainly push through the predentine layer. Cutting off the lesion by
minimal mush removal and sealing it off (with the deeper mush still inside) with glass ionomer or other filling material, will
effectively stop the resorption by starvation - since its nourishment comes from the PDL and not from the pulp. According to
the same research (and again relying on the high degree of similarity between this form of crown resorption and ICRR), in
advanced stages, bone is deposited in the lesion (see list of references in the article) and I would hazard an informed guess
that this is the factor that stops the tooth from responding to extrusive forces - as in a pure ankylosis.For these reasons, I
have recommended surgery to expose the teeth and to seal off the lesions and then to try again. If I am right, the teeth
should respond to well directed traction. Once the teeth erupt, then endo can be done under ideal conditions - if it is required
for reasons of retention of a crown. Leaving the mush in place and properly sealed, it should not cause a pulpal reaction
during this entire period, because it is sterile, uninfected, and now non-progressive. It is not caries and it should not be
treated as such, because it contains no bacteria and therefore it does not generate pulp inflammation.
It is entirely possible that my conclusions are not as well founded as I like to believe, but these points represent my line of
thinking and are the basis for the recommendations that I made in my correspondence
virtually every detail to invasive cervical root resorption (ICRR) that we published in the Angle Orthodontist earlier this year
(Becker A, Abramovitz I, Chaushu S. Failure of treatment of impacted canines associated with invasive cervical root resorption.
Angle Orthodontist, 2013,83:870-876) and was the subject of our presentation at the AAO meeting in Hawaii last year (it's on
the disk from the meeting). Additionally, pre-eruptive crown resorption was the subject of the July 2013 Bulletin on my
website athttp://www.dr-adrianbecker.com/page.php?pageId=273This is not caries, but resorption. According to the research
(see list of refs in that article), it attacks the body of the dentine but stops short at the predentine, which has a much higher
organic content and probably does not actually get through to expose the pulp. The diagnosis that there is an open connection
was presumably made radiographically, which must be viewed with some suspicion. If the resorption mush is cleared away
meticulously, as if it were caries, instrumentation will certainly push through the predentine layer. Cutting off the lesion by
minimal mush removal and sealing it off (with the deeper mush still inside) with glass ionomer or other filling material, will
effectively stop the resorption by starvation - since its nourishment comes from the PDL and not from the pulp. According to
the same research (and again relying on the high degree of similarity between this form of crown resorption and ICRR), in
advanced stages, bone is deposited in the lesion (see list of references in the article) and I would hazard an informed guess
that this is the factor that stops the tooth from responding to extrusive forces - as in a pure ankylosis.For these reasons, I
have recommended surgery to expose the teeth and to seal off the lesions and then to try again. If I am right, the teeth
should respond to well directed traction. Once the teeth erupt, then endo can be done under ideal conditions - if it is required
for reasons of retention of a crown. Leaving the mush in place and properly sealed, it should not cause a pulpal reaction
during this entire period, because it is sterile, uninfected, and now non-progressive. It is not caries and it should not be
treated as such, because it contains no bacteria and therefore it does not generate pulp inflammation.
It is entirely possible that my conclusions are not as well founded as I like to believe, but these points represent my line of
thinking and are the basis for the recommendations that I made in my correspondence
So what are Sam's theoretical options at this point? (Or rather, this is what should have been considered in March 2013):
1. Re-surgery according to the advice of Dr. Becker
2. Transplantation as described by Dr. Heithersay/ Dr Andreasen
3. Orthodontical closure with premolars
4. Extraction - retainers - implants in 6 years or so
Unfortunately, the only option available at UCSF is extraction.
Dec 20, my email: I would appreciate if you could research and refer us to a US University where they would take an interest in treating Sam according to state-of-the-art, and where they have more than one option for treatment. If there is no one in the US, do ask if Sam can get treatment by Dr. Becker's team in Jerusalem.
Dec 20, 2013 (Dr Nelson email): If you don't want to proceed with my referral to the oral surgeon Dr. Hossaini, then you will need to with another orthodontist. I can provide a report and transfer records.
The logical next step: we'll go to Jerusalem! I contact Dr. Becker.
Jan 8: I inform Dr. Nelson that Dr. Becker has scheduled surgery for Sam in Jerusalem on March 5th. Dr Nelson says 'that is surprising and exciting news', he then cancels our appointment for Jan 10. I ask Dr. Nelson to contact Dr. Huang again, tell him the current treatment p and ask to have Sam transfered there. Dr. Nelson responds that he is sending Dr. Huang an AAO transfer form.
Jan 9, 2014, (Dr Nelson email): I will prepare an AAO transfer form and send it to Dr. Huang with a copy to you
Jan 10: I make an appointment for Sam with Dr. Huang with a sense of relief... We need some x-rays for Dr. Becker
Jan 13: I get a call from Dr. Huang's appointment desk saying he can't take on Sam. (It's the third time I have to deduct change of plans by Dr. Nelson by the call from an appointment desk!) Dr. Huang can still see us for a consultation...weird.
Dr. Huang was very nice, but ill at ease. We talked for half an hour, then I realized that Dr. Huang was not up to date on Sam's case. Turns out Dr. Nelson had not contacted Dr Huang and informed him, nor had he asked him about a transfer! Dr. Huang thought I was trying to force Sam into his office and that I am an unpredictable mother, capable of anything! That explains why Dr. Huang kept an extra person (body guard?) in the room and his very worried look. Dr. Huang has not heard anything about Sam since October!
Sam is not happy about being dragged around.
Jan 16: Dr. Nelson's AAO transferral form to Dr. Huang arrives in the email!?
Jan 17, 2014 (Dr Nelson notes): Mom admitted she does not trust anyone at UCSF.
A Unicorn! You can choose to believe in science, or not...
I realize, thinking back on Dr. Huang and our somewhat awkward conversation, what the problem is. He talked of impaction, ankylosis and even root resorption of adjacent teeth, difficulties, and how extraction is the best course; and I kept trying to get back to PEI resorption and ICR resorption, the importance and possible implications of this kind of resorption on having Sam's canines emerge; the reasoning that Dr. Becker has for wanting to repair the crowns and renew traction. I just couldn't make Dr. Huang linger on PEIR/ICRR, it never stuck.
In the Bay Area, and possibly all of the US, nobody believes in PEIR and ICRR. Even one patient that displays clinical evidence doesn't prove anything, it's just one case and counts for nothing. They just don't believe in it, so they can't even see it! Dr. Chen just smiled when I asked about resorption, and when I asked specifically of PEIR he said 'pretty interesting' and disappeared; Dr. Nelson said it's so rare, it's no wonder nobody's heard of it; when my point was that if you have a patient displaying something peculiar you research it; the UCSF endodontist Dr. Janian insists that he's never been exposed to the term PEIR, never read of it, never heard a presentation...It sounds more like he is denying the very existence of a dubious phenomenon, rather than finding it interesting, and something to look into; Dr. Berger doesn't find the 'literature on the subject strong'; Standford got back to me with 'we don't do that kind of surgery'. It's a blind spot.
My delving into the works by Dr. Becker and Dr. Heithersay, just didn't prepare me to understand that in the here and now, Sam is a unicorn! There is no treatment to be had, because his problem is not real according to
everyday orthodontics. No doubt many unicorns have been sacrificed - i.e. impacted teeth extracted - long before they reach a university clinic, and at the UCSF dental departments, unicorns suffer the same fate as they would have in any private practice that doesn't order a CBCT, or doesn't look at the CBCT, doesn't analyze the complications; because in the end, they don't have any treatment options, it's plain traction or extraction.
The forefront of orthodontics is not in the Bay Area, it's wherever there is someone who chooses to see and believe, and there are precious few of them!
I refer you to Dr. Adrian Becker's January Bulletin for 2014:
1. Re-surgery according to the advice of Dr. Becker
2. Transplantation as described by Dr. Heithersay/ Dr Andreasen
3. Orthodontical closure with premolars
4. Extraction - retainers - implants in 6 years or so
Unfortunately, the only option available at UCSF is extraction.
Dec 20, my email: I would appreciate if you could research and refer us to a US University where they would take an interest in treating Sam according to state-of-the-art, and where they have more than one option for treatment. If there is no one in the US, do ask if Sam can get treatment by Dr. Becker's team in Jerusalem.
Dec 20, 2013 (Dr Nelson email): If you don't want to proceed with my referral to the oral surgeon Dr. Hossaini, then you will need to with another orthodontist. I can provide a report and transfer records.
The logical next step: we'll go to Jerusalem! I contact Dr. Becker.
Jan 8: I inform Dr. Nelson that Dr. Becker has scheduled surgery for Sam in Jerusalem on March 5th. Dr Nelson says 'that is surprising and exciting news', he then cancels our appointment for Jan 10. I ask Dr. Nelson to contact Dr. Huang again, tell him the current treatment p and ask to have Sam transfered there. Dr. Nelson responds that he is sending Dr. Huang an AAO transfer form.
Jan 9, 2014, (Dr Nelson email): I will prepare an AAO transfer form and send it to Dr. Huang with a copy to you
Jan 10: I make an appointment for Sam with Dr. Huang with a sense of relief... We need some x-rays for Dr. Becker
Jan 13: I get a call from Dr. Huang's appointment desk saying he can't take on Sam. (It's the third time I have to deduct change of plans by Dr. Nelson by the call from an appointment desk!) Dr. Huang can still see us for a consultation...weird.
Dr. Huang was very nice, but ill at ease. We talked for half an hour, then I realized that Dr. Huang was not up to date on Sam's case. Turns out Dr. Nelson had not contacted Dr Huang and informed him, nor had he asked him about a transfer! Dr. Huang thought I was trying to force Sam into his office and that I am an unpredictable mother, capable of anything! That explains why Dr. Huang kept an extra person (body guard?) in the room and his very worried look. Dr. Huang has not heard anything about Sam since October!
Sam is not happy about being dragged around.
Jan 16: Dr. Nelson's AAO transferral form to Dr. Huang arrives in the email!?
Jan 17, 2014 (Dr Nelson notes): Mom admitted she does not trust anyone at UCSF.
A Unicorn! You can choose to believe in science, or not...
I realize, thinking back on Dr. Huang and our somewhat awkward conversation, what the problem is. He talked of impaction, ankylosis and even root resorption of adjacent teeth, difficulties, and how extraction is the best course; and I kept trying to get back to PEI resorption and ICR resorption, the importance and possible implications of this kind of resorption on having Sam's canines emerge; the reasoning that Dr. Becker has for wanting to repair the crowns and renew traction. I just couldn't make Dr. Huang linger on PEIR/ICRR, it never stuck.
In the Bay Area, and possibly all of the US, nobody believes in PEIR and ICRR. Even one patient that displays clinical evidence doesn't prove anything, it's just one case and counts for nothing. They just don't believe in it, so they can't even see it! Dr. Chen just smiled when I asked about resorption, and when I asked specifically of PEIR he said 'pretty interesting' and disappeared; Dr. Nelson said it's so rare, it's no wonder nobody's heard of it; when my point was that if you have a patient displaying something peculiar you research it; the UCSF endodontist Dr. Janian insists that he's never been exposed to the term PEIR, never read of it, never heard a presentation...It sounds more like he is denying the very existence of a dubious phenomenon, rather than finding it interesting, and something to look into; Dr. Berger doesn't find the 'literature on the subject strong'; Standford got back to me with 'we don't do that kind of surgery'. It's a blind spot.
My delving into the works by Dr. Becker and Dr. Heithersay, just didn't prepare me to understand that in the here and now, Sam is a unicorn! There is no treatment to be had, because his problem is not real according to
everyday orthodontics. No doubt many unicorns have been sacrificed - i.e. impacted teeth extracted - long before they reach a university clinic, and at the UCSF dental departments, unicorns suffer the same fate as they would have in any private practice that doesn't order a CBCT, or doesn't look at the CBCT, doesn't analyze the complications; because in the end, they don't have any treatment options, it's plain traction or extraction.
The forefront of orthodontics is not in the Bay Area, it's wherever there is someone who chooses to see and believe, and there are precious few of them!
I refer you to Dr. Adrian Becker's January Bulletin for 2014:
In the preface to the first edition of my book which was published in 1998, I pointed out at the time that there were virtually no graduate/postgraduate orthodontic specialty programs that included tooth impaction in their curricula in any didactic or disciplined academic fashion. This situation has not changed in the 15 years since that time. The upshot is that there are few orthodontists out there in the big wide world who are proficient at treating them. In contrast with other areas of our profession, educators in this sphere are few. Following the lamented passing of Samir Bishara in October 2010, of Juri Kurol in October 2011, of Tiziano Baccetti in November 2011 and most recently, of Vince Kokich in July 2013, there remain even fewer of us who actually teach and research the broad subject of impacted teeth. If we add to that the fact that I live, teach and do my research in a dangerous neighborhood, it appears that I belong to an endangered species in a high risk branch of the orthodontic profession!
The orthodontic department of the Hebrew University-Hadassah School of Dental Medicine in Jerusalem is a notable exception to this educational vacuum and, as the direct result, a disproportionately large quantity of the clinical research that has been published in the peer-reviewed orthodontic literature on virtually every aspect related to impacted teeth, has emanated from Jerusalem.
Jan 17, 2014, visit (8 week intervall)
We need x-rays for Dr. Becker. He wants to check for ICRR. We are sent down to radiology. I hear the technician tell Sam he is about to take a full mouth series, 16 periapicals. I stop him. Somehow it is not clear from Dr. Nelson's referral that we only want #6 and #27. (1.65 x 14 = 23.1 µSv saved exposure.)
Dr. Nelson looked at the images and said he thinks #27 could emerge. (Obviously not through Dr. Nelson's efforts, he stopped traction on Nov 22).
We need x-rays for Dr. Becker. He wants to check for ICRR. We are sent down to radiology. I hear the technician tell Sam he is about to take a full mouth series, 16 periapicals. I stop him. Somehow it is not clear from Dr. Nelson's referral that we only want #6 and #27. (1.65 x 14 = 23.1 µSv saved exposure.)
Dr. Nelson looked at the images and said he thinks #27 could emerge. (Obviously not through Dr. Nelson's efforts, he stopped traction on Nov 22).
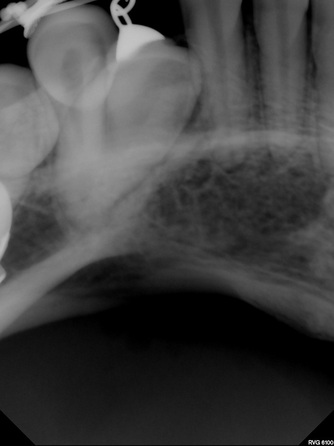
|
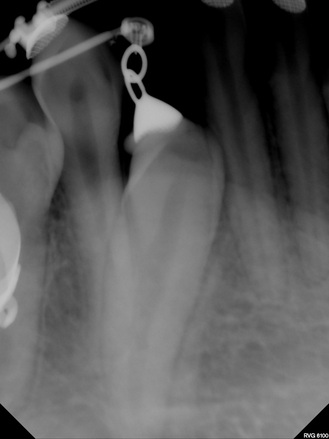
|
|
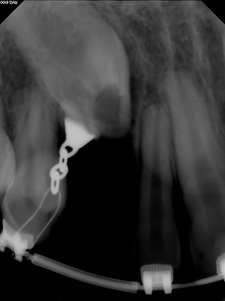

CDental, Menlo Park, each periapical is 9,5 µSv.
|

|
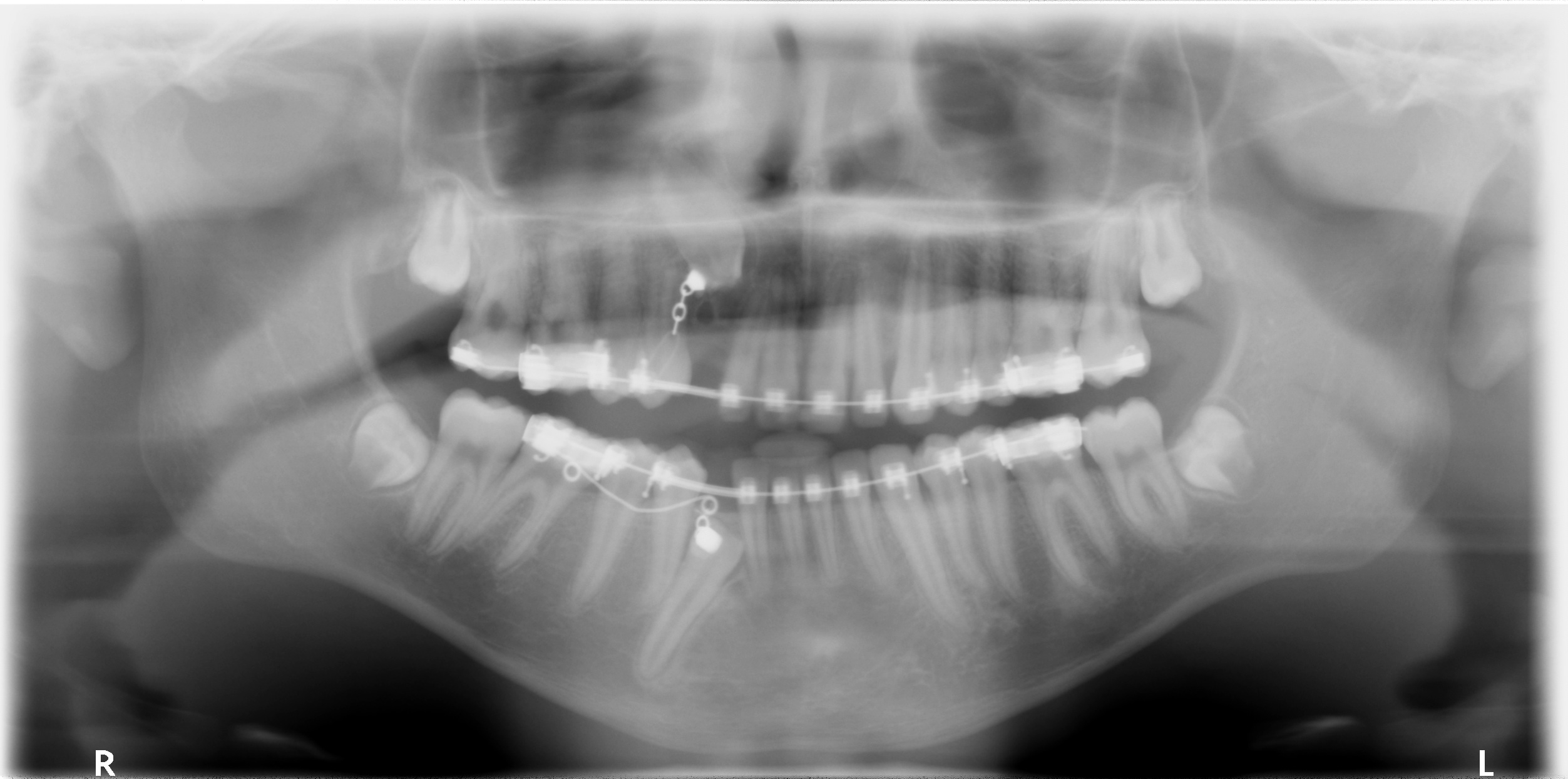
1/17/2014 UCSF panorex, 26 µSv
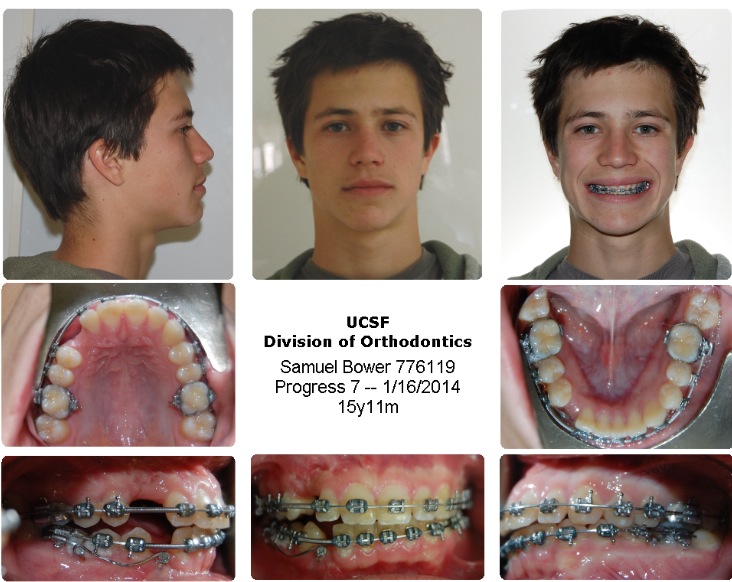
|
|
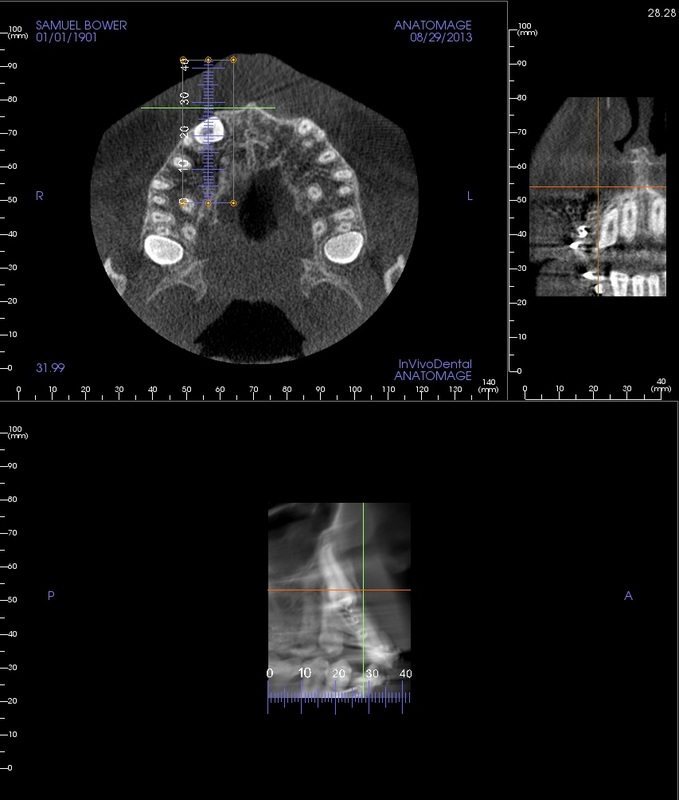
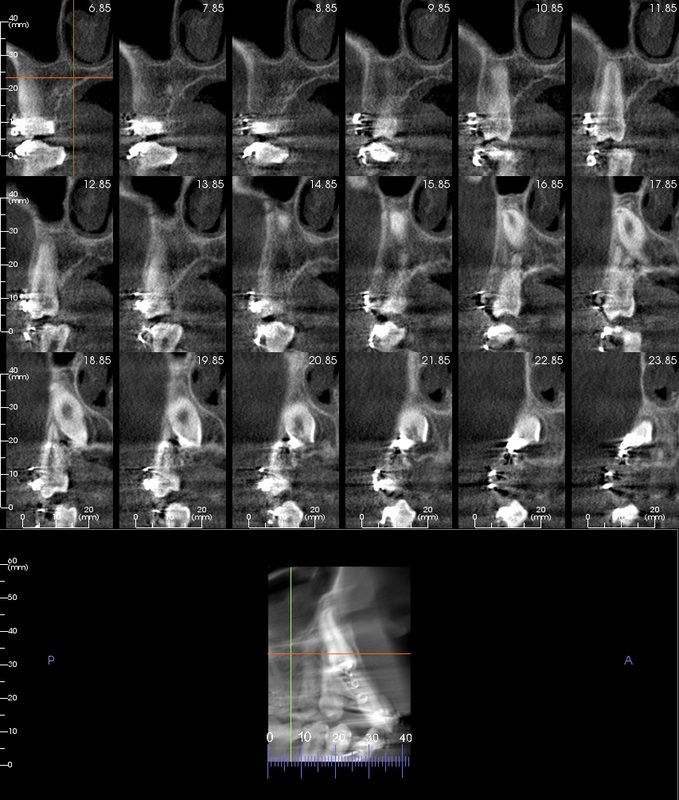
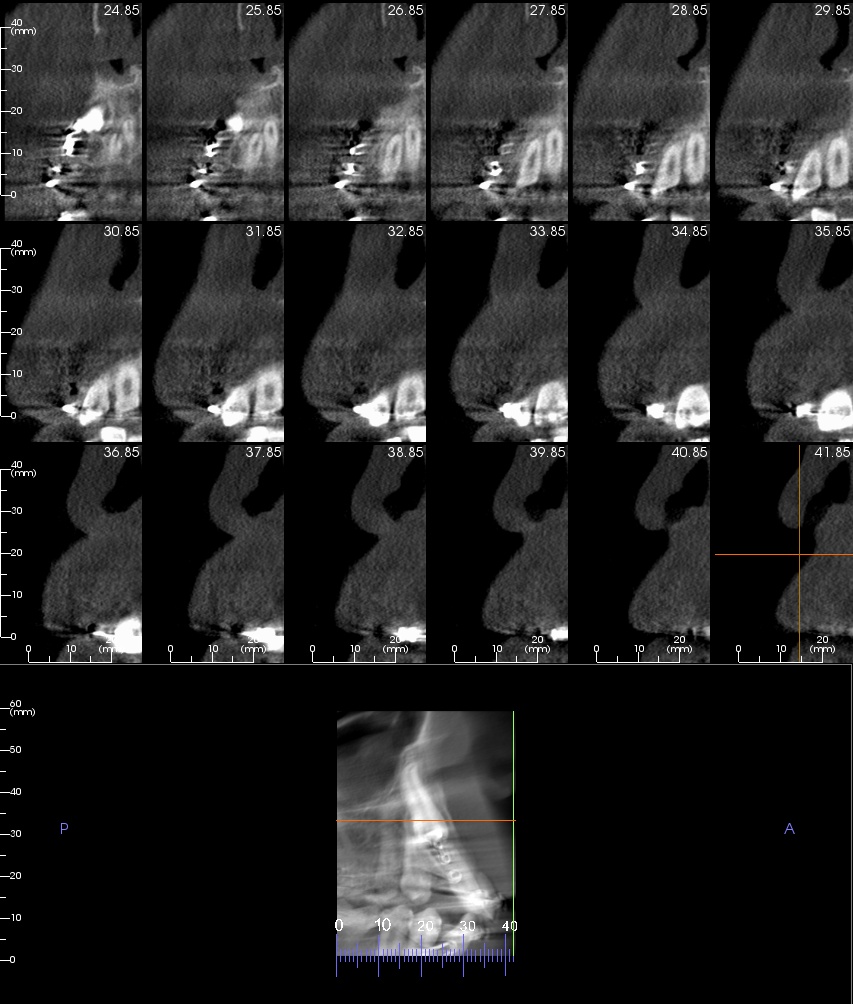
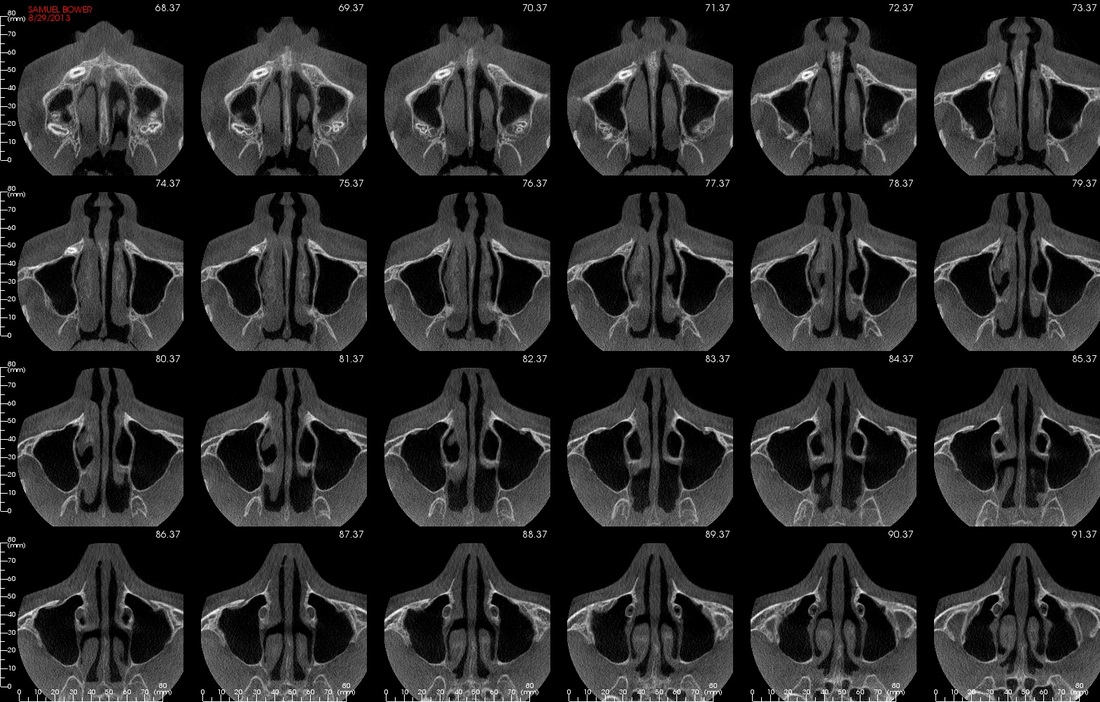
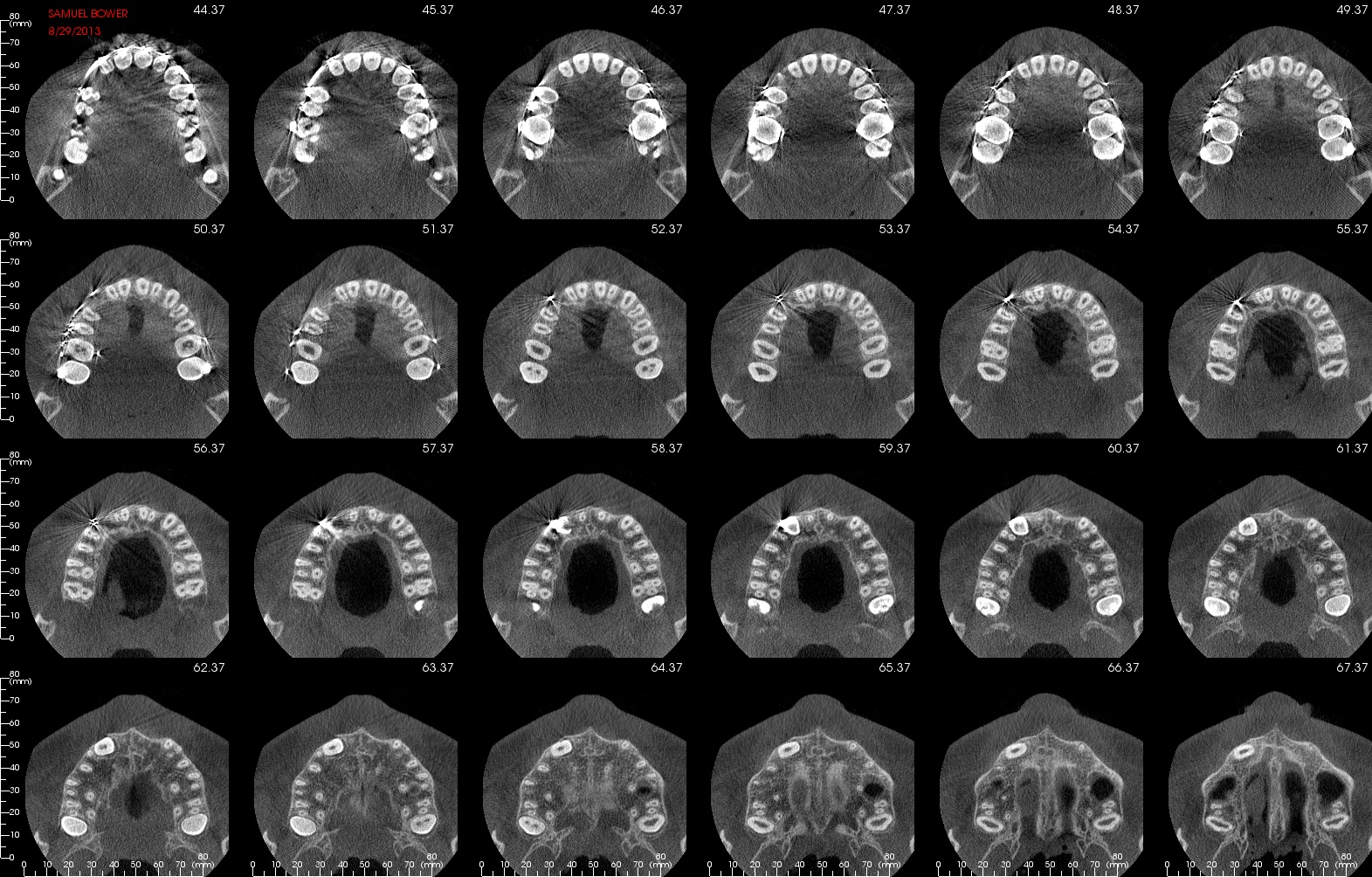
Below: transaxial (vertical) mandibular and maxilliar views of August 2013 CBCT
Looking at the Panorex, it doesn't look to me as if there is enough room for #27 to erupt, it looks like the space is more crowded than previously. (Though, I understand, a Panorex can distort the image. )
(Concerning 'space': After the report from the Beamreaders where it was stated:
(05/12 scan) 'The available interproximal space for #6's proper eruption/traction was not enough due to #6's angulation/position'
Also, in surgeon #2 -Dr. Lee's- pre-surgery notes: 'There does not appear to be sufficient space for these teeth'.
Dr. Nelson's comment when asked about those statements was that they are wrong, there is enough space.)
Jan 20: Had to get new peri-apicals at C-Dental in Menlo Park.
At least I stopped new images of #27, as the referral incorrectly requested, and saved Sam from another 19 µSv.
Total dose for Sam for two periapicals and a panorama comes to 50 µSv.
Unfortunately you can't have the images instantly, as at UCSF, they are 'worked on' before they are released.
Very unfortunate that all the 'peri-apicals' taken at UCSF to track progress, cut off the root part.
If impacted teeth don't move, ICRR needs to be a consideration.
Feb 7, 2014 (Dr Nelson formal letter): [Dr Nelson dismissing Sam from UCSF]
You refused to follow my recommendation for a surgical opinion with the UCSF Oromaxillofacial Surgeon, Dr. Mehran Hossaini.
Dr Bower told me that she does not trust my judgement or competence in treating Sam’s case.
I have recommended an Oral Surgery consultation at UCSF to consider exploratory surgery on both teeth to make the best decision for further recovery effort. Extraction may be indicated. This was not acceptable by you and I am told you want to take Sam to Jerusalem for a consultation with another orthodontist.
Two teeth are impacted, #6 and # 27…Both teeth have internal resorption in the crowns, which may or may not communicate with the pulp canals, and may or may not be the reason for the lack of progress
Please immediately seek the care and treatment of another orthodontist.
…
it is not my responsibility to locate another orthodontist who will be acceptable for your family. You could contact the San Francisco Orthodontic Dental Society
Feb 13, 2014 (Dr Nelson email): I did ask Dr. Orellana to take on the case - she is not willing to do so.
[at the January 16th visit, I had asked for another UCSF orthodontist. I wrote her again and got an anwer on Feb 15, 2014 (Dr Orellana): This is a complex impaction recovery case. I have minimal experience in such cases; therefore, I don't feel comfortable taking on Sam's case. I would recommend that you contact the San Francisco Dental Society as advised in Dr. Nelson's letter.]
March 24, 2014 (Dr Nelson email): From Dr. Becker’s report, he found what he expected and applied his protocol. His reasoning makes sense to me, and I hope that progress will be evident. I forwarded his information to Dr. Hossaini, since he was not familiar with the protocol.
Finding a new orthodontist...
I asked for another UCSF orthodontist. Dr. Nelson said that the only professor available would be Dr. Maria Orellana. Her response was that Sam is a complex recovery case and she doesn't have the necessary experience. They both recommend me to find an orthodontist through the 'San Francisco Dental Society'. When I call there asking for a specialist in impacted canines it turns out they can only provide phone-book-type info in the form of names of orthodontists in general...
What is the use of that? So how do you find a specialist? yelp?
We start off Sam's 4th year of braces by leaving UCSF which has been a disappointment in all respects:
competence and skill, concern and care of Sam as a patient, interdisciplinary teamwork and scientific interest in
orthodontic problems, integrity and accountability.
Summary of 2 years at UCSF ;
- One CBCT that wasn't looked at pre or post surgery #2 (until 15 months later)
- No mold/ imprint made, no cephalogram, no periapical that showed the root (peri apical area) until Dr Becker
asked for it pre op.
- Surgery without planning
- No diagnosis or consideration of resorption before or after surgery by 'the dental team'
- Another CBCT where the results are not conclusive, not ordered by the treating orthodontist.
- $ 5325
I asked for another UCSF orthodontist. Dr. Nelson said that the only professor available would be Dr. Maria Orellana. Her response was that Sam is a complex recovery case and she doesn't have the necessary experience. They both recommend me to find an orthodontist through the 'San Francisco Dental Society'. When I call there asking for a specialist in impacted canines it turns out they can only provide phone-book-type info in the form of names of orthodontists in general...
What is the use of that? So how do you find a specialist? yelp?
We start off Sam's 4th year of braces by leaving UCSF which has been a disappointment in all respects:
competence and skill, concern and care of Sam as a patient, interdisciplinary teamwork and scientific interest in
orthodontic problems, integrity and accountability.
Summary of 2 years at UCSF ;
- One CBCT that wasn't looked at pre or post surgery #2 (until 15 months later)
- No mold/ imprint made, no cephalogram, no periapical that showed the root (peri apical area) until Dr Becker
asked for it pre op.
- Surgery without planning
- No diagnosis or consideration of resorption before or after surgery by 'the dental team'
- Another CBCT where the results are not conclusive, not ordered by the treating orthodontist.
- $ 5325
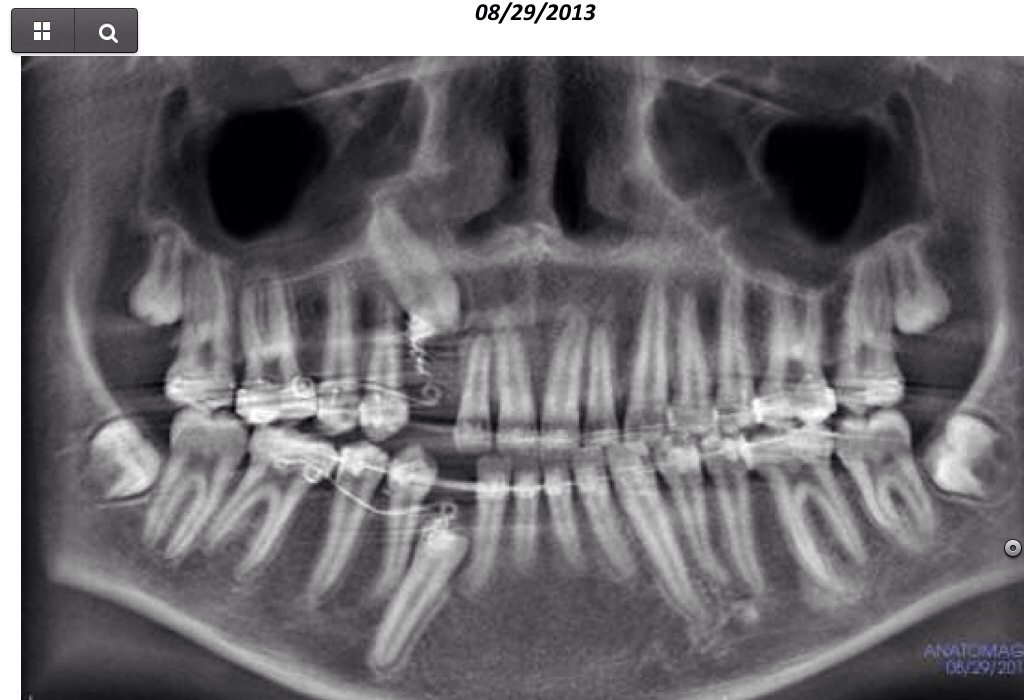
CBCT derived panorama
|

1/17/2014: x-rays ordered by Dr. Becker
|

Sam, 15, summer of 2013. He likes food, windsurfing and waterpolo.
|
|


{kind=link}
(1) Preface to third Edition from 2012 of "On the Treatment of Impacted Canines" by Dr. Adrian Becker.
(2) Dr. Mehran Hossaini in the chapter 'Surgical Treatment of Impacted Teeth Other than Third Molars' in 'Oral
and Maxillofacial Surgery', in 'Oral and Maxillofacial Surgery' from 2010.
(3) http://www.dentalxp.com/content/1222/9d329a8f-a7ee-4dc6-907a-85380e14c627.pdf
(2) Dr. Mehran Hossaini in the chapter 'Surgical Treatment of Impacted Teeth Other than Third Molars' in 'Oral
and Maxillofacial Surgery', in 'Oral and Maxillofacial Surgery' from 2010.
(3) http://www.dentalxp.com/content/1222/9d329a8f-a7ee-4dc6-907a-85380e14c627.pdf