Progressive Condylar Resorption (PCR) - or Idiopathic Condylar Resorption (ICR): a Tempero Mandibular Joint (TMJ) problem
(or Progressive Mandibular Retrusion, or 'Adolescent Internal Condylar Resorption, or 'Cheerleader's Syndrome' etc. which is probably an illustration of how little is known about this/these condition/s.
What the etiology is, what the patofysiology is and what to do about it)
Normally eating and speaking is something we do without giving it much thought. But, imagine if every time you open your mouth you have pain, or it clicks, or with ersosion of the mandibular condyle, imagine having your jaw literally drop, and loose your chin.
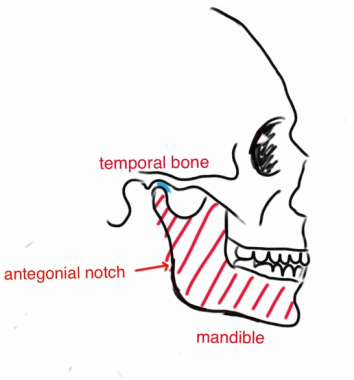
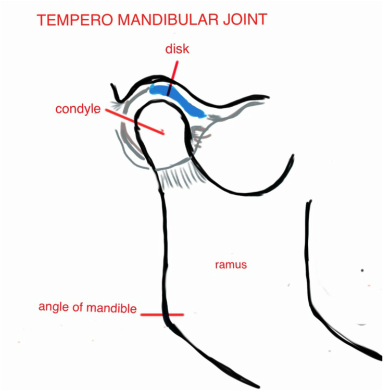
Opening the mouth is done by involving the tempero mandibular joint (TMJ) and it's different parts: the mandibular condyle, a disc, ligaments and muscle.
|
|
Naturally the body is constantly remodeling parts of the body fixing and adapting. With PCR the fibrocartilage of the condyle is broken down, and then resorption continues in the bone. The condyle length is reduced.
The disc, is a shock absorber and lubricator. The disc can get displace, with or without symptoms.
The disc, is a shock absorber and lubricator. The disc can get displace, with or without symptoms.
Just like the resorption in teeth (ICR, PEIR) this resorption is described in literature as 'not clearly understood'.
It's unusual enough that you will not be very familiar with it unless you specialize and take a special interest.
Clearly, if you end up with a patient developing this problem, you should take a special interest for your patient's sake and educate yourself enough that you can get the patient proper care.
It's unusual enough that you will not be very familiar with it unless you specialize and take a special interest.
Clearly, if you end up with a patient developing this problem, you should take a special interest for your patient's sake and educate yourself enough that you can get the patient proper care.
Some statements from 'Progressive/ Idiopathic Condylar Resorption' (3):
PCR...is an uncommon degenerative disease of the temperomandibular joint (TMJ) of an aggressive nature that
is seen mostly in female adolescents and young women. Pathognomic features of this condition include a loss of
condylar mass, thereby decreasing the height nof the ramus and length of the mandible, and opening rotation
of the mandible resulting in a Class II open bite.
PCR is also nicknamed 'cheerleader's syndrome' because it is 8:1 affecting women, and some of them have an identified trauma to the face/chin area, and it's mainly teens and young adults. In total it affects about 1 in 5000 according to (3). 'There appears to be an unexplained "burnout" of the resorption process in afflicted individuals sometime in the mid-20s, although resorption can extend into the early 30s.
The disease is not clearly understood and neither is the etiology. Different causes could be:
a) Mechanical overloading:
- trauma. In this case the effects of PCR can turn up at any time after the trauma.
- third molar extractions
b) Orthognatic surgical procedures (mandibular advancement over 5 mm).
c) Orthodontic treatment
d) Radiation
e) Hormone imbalances, as lack of natural estradiol
f) Inflammatory arthritis
g) Iatrogen
h) Idiopathic
PCR...is an uncommon degenerative disease of the temperomandibular joint (TMJ) of an aggressive nature that
is seen mostly in female adolescents and young women. Pathognomic features of this condition include a loss of
condylar mass, thereby decreasing the height nof the ramus and length of the mandible, and opening rotation
of the mandible resulting in a Class II open bite.
PCR is also nicknamed 'cheerleader's syndrome' because it is 8:1 affecting women, and some of them have an identified trauma to the face/chin area, and it's mainly teens and young adults. In total it affects about 1 in 5000 according to (3). 'There appears to be an unexplained "burnout" of the resorption process in afflicted individuals sometime in the mid-20s, although resorption can extend into the early 30s.
The disease is not clearly understood and neither is the etiology. Different causes could be:
a) Mechanical overloading:
- trauma. In this case the effects of PCR can turn up at any time after the trauma.
- third molar extractions
b) Orthognatic surgical procedures (mandibular advancement over 5 mm).
c) Orthodontic treatment
d) Radiation
e) Hormone imbalances, as lack of natural estradiol
f) Inflammatory arthritis
g) Iatrogen
h) Idiopathic
The patofysiology that breaks down the condyle seems to be shared by the the different causes:
Cytokine-activated osteoblasts promote the recruitment and activity of osteoclasts that, in turn, result in the
secretion of enzymes that are responsible for the breakdown of hydroxyapatite and collagen. (4)
Cytokine-activated osteoblasts promote the recruitment and activity of osteoclasts that, in turn, result in the
secretion of enzymes that are responsible for the breakdown of hydroxyapatite and collagen. (4)
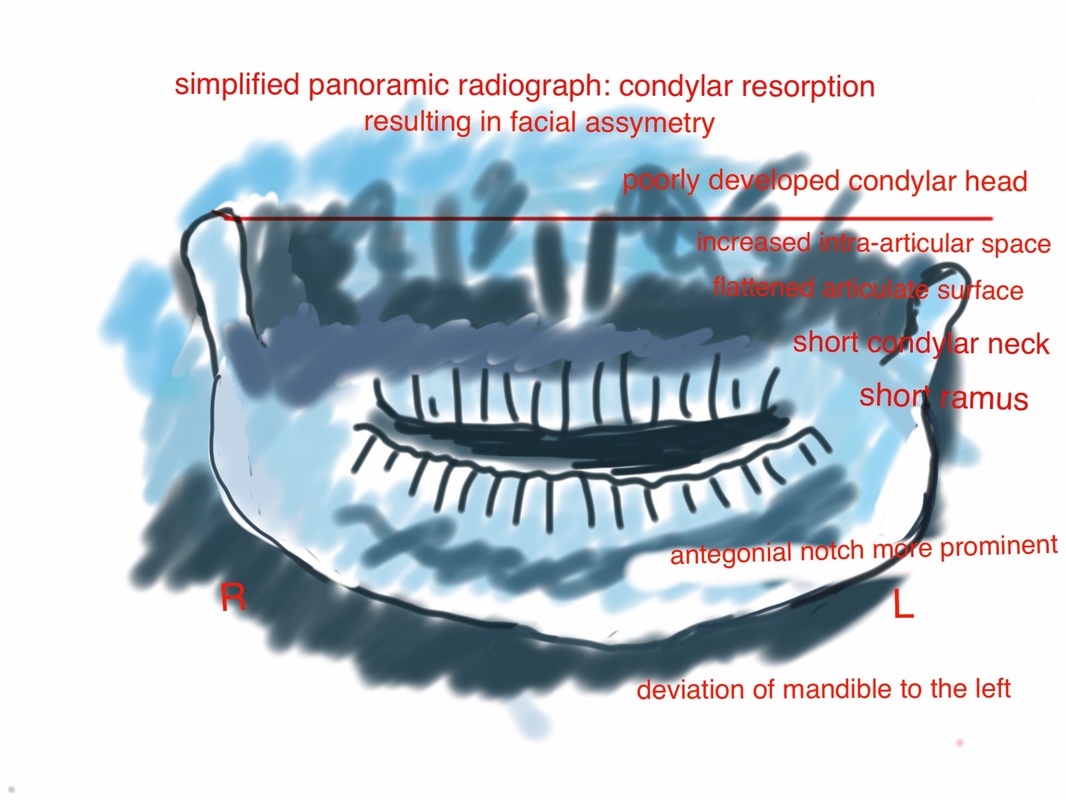
Diagnostic methods:
- Panoramic x-ray
- Cephalogram. 'Serial cephalometric radiographs are profoundly diagnostic of active ICR'.(3)
- CBCT
- Panoramic x-ray
- Cephalogram. 'Serial cephalometric radiographs are profoundly diagnostic of active ICR'.(3)
- CBCT
The findings will be:
- decreased ramus height
- decreased condylar height
- altered volume of the condyle
- decreased SNB angle and mandibular plane angle
- a retrognathic profile
- decreased ramus height
- decreased condylar height
- altered volume of the condyle
- decreased SNB angle and mandibular plane angle
- a retrognathic profile
'Progressive/Idiopathic Condylar Resorption' (3) writes:
'Suspicion of PCR/ICR requires that a history should be taken followed by certain clinical procedures. Study
models should either be mounted or stabilized with polyvinylsiloxane bite to register the open bite. Obviously,
cephalometric radiographs should be taken both before and during treatment, and superimposition should be
analyzed. The OPG [panorama x-ray] may be suggestive of ICR, but a CBCT is also indicated to get a clearer
picture.
...
collaboration with a team of experts: an oral radiologist (to submit a written report on the CBCT scans), an
oral surgeon with extensive experience with orthognatic surgery and ideally with experience in dealing with
PCR/ICR cases, and referral to a rheumatologist for blood tests to rule out autoimmune and rheumatoid
diseases.
...
The number-1 rule that has emerged from both clinical and medicolegal experience is this: discontinue
treatment and retain. However, continue to monitor the patient every 6 months and take annual
cephalometric radiographs and CBCT scans; all of this should be in conjunction with your professional
colleagues who will be involved in this case. Once the condyle has healed and the occlusion is stable,
discussion orthodontic treatment options should be conducted with all parties, with the patient being part of
the decision-making. Both emphatic communication that "you really care" and careful record keeping will
minimize the chance of legal liability. (3)
'Suspicion of PCR/ICR requires that a history should be taken followed by certain clinical procedures. Study
models should either be mounted or stabilized with polyvinylsiloxane bite to register the open bite. Obviously,
cephalometric radiographs should be taken both before and during treatment, and superimposition should be
analyzed. The OPG [panorama x-ray] may be suggestive of ICR, but a CBCT is also indicated to get a clearer
picture.
...
collaboration with a team of experts: an oral radiologist (to submit a written report on the CBCT scans), an
oral surgeon with extensive experience with orthognatic surgery and ideally with experience in dealing with
PCR/ICR cases, and referral to a rheumatologist for blood tests to rule out autoimmune and rheumatoid
diseases.
...
The number-1 rule that has emerged from both clinical and medicolegal experience is this: discontinue
treatment and retain. However, continue to monitor the patient every 6 months and take annual
cephalometric radiographs and CBCT scans; all of this should be in conjunction with your professional
colleagues who will be involved in this case. Once the condyle has healed and the occlusion is stable,
discussion orthodontic treatment options should be conducted with all parties, with the patient being part of
the decision-making. Both emphatic communication that "you really care" and careful record keeping will
minimize the chance of legal liability. (3)
Ideas on farmacological treatment presented in (4):
- cytokine control such as TNF-alfa inhibitorer. There has been a trial for intra-articular injections in the TMJ.
- MMP inactivation by tetracyclines. Atrial using doxycycline twice a day for 3 months suppressed MMP activity in patients diagnosed with advanced ostoarthritis of the TMJ.
- inhibition of prostanoids and leukotrienes by omega-3 fatty acids. Studies have shown beneficial effects in RA patients.
- inhibition of prostanoids and leukotriene production by cyclooxygenase and lipoxygenase inhibitors.
When TMJ inflammation is suspected(eg. joint effusion, slight posterior open bite with localized preauricular
pain, and rapidly progressive condylar resorption), then initiation of nonsteroidal anti-inflammatory drug therapy
should be considered. On the basis of current information, 20 mg of piroxicam daily is appropriate unless
contraindicated.(4)
- statins
- RANKL (a cytokine) inhibitor
- IL-6 receptor inhibitor
- Monoclonal antibodies
- cytokine control such as TNF-alfa inhibitorer. There has been a trial for intra-articular injections in the TMJ.
- MMP inactivation by tetracyclines. Atrial using doxycycline twice a day for 3 months suppressed MMP activity in patients diagnosed with advanced ostoarthritis of the TMJ.
- inhibition of prostanoids and leukotrienes by omega-3 fatty acids. Studies have shown beneficial effects in RA patients.
- inhibition of prostanoids and leukotriene production by cyclooxygenase and lipoxygenase inhibitors.
When TMJ inflammation is suspected(eg. joint effusion, slight posterior open bite with localized preauricular
pain, and rapidly progressive condylar resorption), then initiation of nonsteroidal anti-inflammatory drug therapy
should be considered. On the basis of current information, 20 mg of piroxicam daily is appropriate unless
contraindicated.(4)
- statins
- RANKL (a cytokine) inhibitor
- IL-6 receptor inhibitor
- Monoclonal antibodies
SURGICAL OPTIONS
-orthognathic (corrective jaw) surgery - high % of relapse or TMJ dysfunction
- condylectomy with costochondral grafting
-orthognathic (corrective jaw) surgery - high % of relapse or TMJ dysfunction
- condylectomy with costochondral grafting
(1) http://www.arnettgunson.com/education-materials/tmj/condylar-resorption - Dr Arnett.Gunson
His TMJ medication page is 'under construction'
(2) http://www.drlarrywolford.com - Dr Wolford is a surgeon at the Baylor University Medical Center in Dallas
(3) Handelsman C., Greene C. Progressive/Idiopathic Condylar Resorption: An Orthodontic Perspective. Seminars in Orthodontics. June 2013. https://www.researchgate.net/publication/257483241_ProgressiveIdiopathic_Condylar_Resorption_An_Orthodontic_Perspective
(4) Gunson M., Arnett W., Milam S. Pathophysiology and Pharmacologic Control of Osseous Mandibular Condylar Resorption. . J Oral Maxillofac Surgery 70:1918-1934, 2012
(5) Y.H. Shen, Y.K. Chen, S.Y. Chuang. Condylar resorption during active orthodontic treatment and subsequent therapy: report of a special case dealing with iatrogenic TMD possibly related to orthodontic treatment.Journal of Oral Rehabilitation. Vol 32, Issue 5, May 2005.