Dilacerated roots and Apicotomy
Note: Below I cite and show Dr Jae Park's slides on Apicotomy from 2014. I contacted Dr Park in 2018 asking if he had any new information on apicotomy based on the 4 years since. I did so after I heard from a mom who had recently had her 15-year-old daughter go through it, with, was sounded like, no success. Dr Park replied, but ignored my question. I think it would be wise to be skeptical of this procedure until there are studies confirming that the reasoning behind it and the surgery itself make sense.
Dilaceration means that the tooth root is curved. The root tip can sit at an angle that makes it impossible to pull the tooth down.
When an impacted canine is complicated by a dilacerated root and/or apical root ankylosis, in some cases, the root tip can be broken to free from the rest of the tooth while still keeping the pulp viable. The forefront of this technique is in Brazil and pioneered by oral surgeon Edela Puricelli, who invented the technique and the special chisel used, in 1987.Even though it seems to be a successful technique, it hasn't spread. I am afraid that the entrance of implants, the primadonna on the dental scene, made the technique a wallflower before it had a chance. (Could have something to do with all the companies with interest in developing different implant screws and materials, while apicotomy is a technique, that only asks for a chisel and skill.)
Note: Below I cite and show Dr Jae Park's slides on Apicotomy from 2014. I contacted Dr Park in 2018 asking if he had any new information on apicotomy based on the 4 years since. I did so after I heard from a mom who had recently had her 15-year-old daughter go through it, with, was sounded like, no success. Dr Park replied, but ignored my question. I think it would be wise to be skeptical of this procedure until there are studies confirming that the reasoning behind it and the surgery itself make sense.
Dilaceration means that the tooth root is curved. The root tip can sit at an angle that makes it impossible to pull the tooth down.
When an impacted canine is complicated by a dilacerated root and/or apical root ankylosis, in some cases, the root tip can be broken to free from the rest of the tooth while still keeping the pulp viable. The forefront of this technique is in Brazil and pioneered by oral surgeon Edela Puricelli, who invented the technique and the special chisel used, in 1987.Even though it seems to be a successful technique, it hasn't spread. I am afraid that the entrance of implants, the primadonna on the dental scene, made the technique a wallflower before it had a chance. (Could have something to do with all the companies with interest in developing different implant screws and materials, while apicotomy is a technique, that only asks for a chisel and skill.)
|
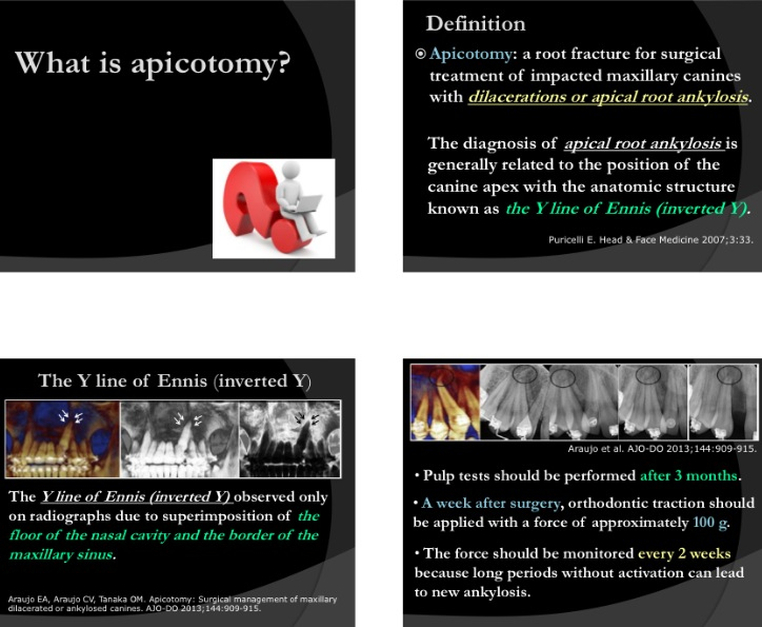
Dr. Puricelli notes that impaction seems to be related to the anatomical position of the root, in what is somewhat mystically named "the inverted Y of Ennis" (a good Harry Potterish title: "Sam Bower and the inverted Y of Ennis"). Anatomically it is "the region where the cortices of the nasal cavity and the maxillary sinus meet"(2).
With Dr Puricelli's technique you are not supposed to damage the nerve and 'kill the tooth', there is no root filling. It is apicotomy, not apicoectomy.**** Dr Puricelli's paper (1) describes 30 cases between 1983 and 2003, where only 3 cases ended in extraction. The article points out the usefulness of CBCT in analyzing dilacerations and ankylosis. |

I borrowed this image from:
http://drgstoothpix.com/2012/06/06/anatomy-on-radiographs-intraoral-radiographs-part-i/
|
|
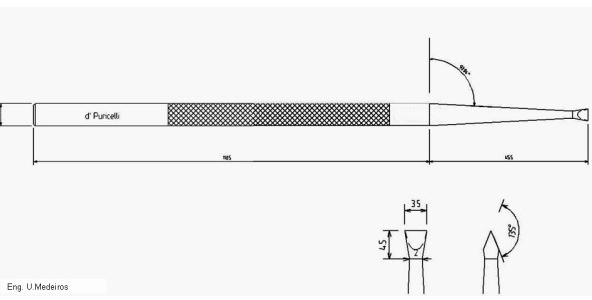
Dr. Puricelli's chisel for selectively taking off the dilacerated part of a root:
A 16.5 mm long, double-bezel chisel with 135˚ angle. It's active region iis 3.5 mm, 4.0 mm thick and 5.0 mm long. (1) The design of the double-bezel chisel proposed by Puricelli is essential for maintenance of integrity of the pulp tissue.(1) Technically, rupture of the pulp tissue is avoided during the induction of fracture and the light movements aiming at inducing luxation in the fracture line. In vitro experiments confirm that the pulp tissue is maintained. The design of the double-bezel chisel proposed by Puricelli is essential for maintenance of integrity of the pulp tissues.(1) |
Dr Puricielli describes her technique: At the apical third she makes a 1.0mm deep grove, then she makes it fracture of with her chisel with a "light hit". You then might make a light luxation to confirm the detachment. The root tip is left in order to help the tooth stay vital. You apply traction (100 g) after a week, check the traction every 2 weeks to keep traction active, and make pulp tests after 3 months.
|
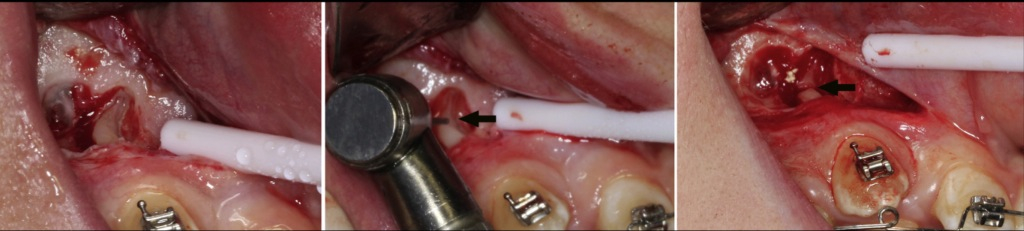
Pictures from Dr. Araújo's article (2)
This is the conclusion of Dr Puricelli's 2007 article:
Apicotomy is a technique which has been successfully used during the past twenty years, for conservative intervention in cases of impacted upper canines with dilaceration or apical root-ankylosis. Currently, it could also be indicated for lower canines. The technique aims at freeing the tooth from its dilacerated or ankylosed portion inducing, thus, its traction and eruption. It was initially indicated after failure of conservative techniques for inducing spontaneous eruption and orthodontic traction. At the moment, image examinations allow precise diagnosis and its indication as a first surgical therapeutic option. The technique is counter-indicated for young patients with incomplete rhizogenesis or for teeth with total root ankylosis. (1)
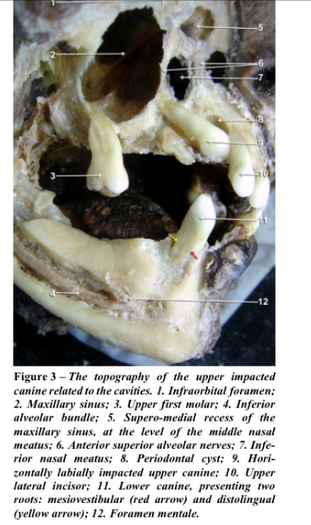
This image is from a dissection of a skull from a 53-year-old man.
The article where I found it is 'Altered anatomy in a case with a buccally impacted maxillary canine' (6).
It is an impacted canine, without dilaceration, but as it looks with the apex ankylosed, and a periodontal cyst next to it. The anatomic reality gives a good idea of the general problem.
The article cautions that if you were going to extract the canine the risk for penetration during surgery would be high because of 'the apical part of the root was incalated between the maxillary sinus and an expanded inferior nasal meatus'.
The article where I found it is 'Altered anatomy in a case with a buccally impacted maxillary canine' (6).
It is an impacted canine, without dilaceration, but as it looks with the apex ankylosed, and a periodontal cyst next to it. The anatomic reality gives a good idea of the general problem.
The article cautions that if you were going to extract the canine the risk for penetration during surgery would be high because of 'the apical part of the root was incalated between the maxillary sinus and an expanded inferior nasal meatus'.

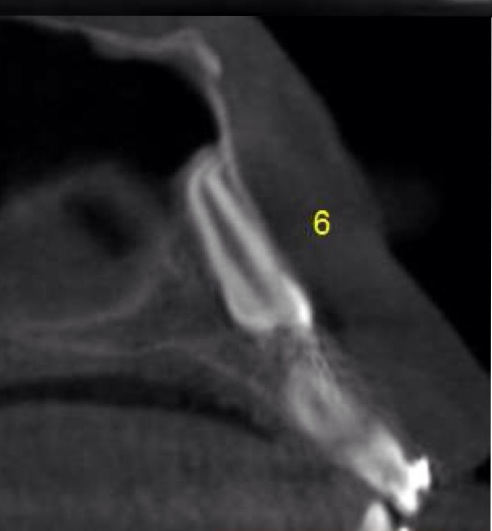
Sam's dilacerated #6
|
|


This is a case report from (5), with a 10-year-old girl.
After apicotomy the tooth could be moved in alignement. It was OK 5 years later.
|

A dilacerated canine. One of the 3 cases described in (2).
Successfully treated with apicotomy.
|
'Apicotomy as Treatment for Failure of Orthodontic Traction"(4) describes a case of a 10-year-old Brazilian girl with a dilacerated root on her impacted canine, and 'probably apical ankylosis'. After 'an apical fracture' the tooth could be moved into position.(http://www.hindawi.com/crim/dentistry/2013/168232/)
Another article from 2013: Apicotomy: surgical management of maxillary dilacerated or ankylosed canines,
by Drs. Eustáquio A. Araújo*, Christina V. Araújo and Orlando M. Tanaka.
This clinical article reports a technique, apicotomy, for managing dilacerated or ankylosed canines. The
records of 3 patients successfully treated with apicotomy are presented. Orthodontists observe clinically
significant incidences of impacted maxillary canines in their daily practices. Several procedures have been
described to bring an ankylosed, impacted tooth into occlusion. Luxation is the most widely used solution, but
there are risks involved with that approach, and the success rate is low. Surgical repositioning has also been
used, but morbidity is high, and the aggresiveness of the procedure might also contraindicte it. Ankylosis
might be related to anatomic position of the canine's root apex and its adjacent anatomic structures.
Apicotomy is a guided fracture of a canine root apex, followed by its orthodontic traction. It is a conservative
surgical alternative for treating impacted canines with dilacerations of apical root ankylosis.(2)
The article relates 3 cases. The surgery is described and the following treatment.
The force [of traction] should be monitored every two weeks because long periods without activation can
lead to new ankylosis.
.....
Traditionally, once a tooth becomes ankylosed, surgical luxation has been the treatment of choice.
After surgical luxation, immediate orthodontic traction is performed. If the tooth does not move during the
next 6 months, the procedure is repeated; if it fails agin, extraction of the tooth is the treatment of choice.
Orthodontic light forces should be immediately applied after luxation to prevent reankylosis, but even with
immediate traction, ankylosis often occurs again.
With contemporary imaging techniques (CBCT), a better diagnosis of the area of ankylosis can be made.
These images were widely used for all patients here described. When properly indicated, as demonstrated in
the 34 cases presented, it is reasonable to consider the apicotomy surgical procedure as a viable therapeutic
option following the failure of other maxillary canine traction mechanics.
I do not have access to this article from 2011 from Brazil: 'Apicotomy and double traction: conservative interventions for impacted teeth" (3)
Apicotomy as Treatment for Failure of Orthodontic Traction (5) is from 2013 and comes out of the Department of Stomatology, Santa Maria, Brazil. It relates a case of a 10-year-old with impacted canine, dilacerated root, a dentigerous cyst, maxillary sinus infection, and presumed ankylosis.
Surgical access to a displaced tooth is the key factor in treatment success, and the intervention should be
carefully planned.
...
The appropriate direction of eruption for a palatally impacted canine is essential for correcting the impaction
and bringing the tooth to its correct position. It is important to remember that the presence of the
periodontal ligament is necessary to allow tooth movement. This way, the main movement direction of the
displaced tooth must be following its long axis, regardless of whether it will occur far from the correct
position. The simple lateral traction of the tooth toward the edentulous alveolar ridge finds immediate
resistance due to the compression of the canine crown against the adjacent palatine bone. The consequence
can be bone necrosis in the crown, and thus, canine enamel damage can occur. These facts should be
observed in order to minimize the orthodontic movement failure, as proposed by Becker et al.[see Becker
'Analysis of failure...']
It the case above the infection was first treated, then the apicotomy was performed. The root length was reduced, but the tooth was still vital at a follow-up after five years.
Dr. Puricelli's technique was included in a talk and power point presentation by Dr. Jae Hyun Park*** at the AAO yearly conference in April 2014, New Orleans, entitled 'Diagnosis and Treatment of Impacted Maxillary Canines' using CBCT'. I wrote Dr Park about the technique, and where you could have it done in the US. His answer was that 'any skilled surgeon' could do it if shown the articles. The question is would they though? When I wrote a Stanford surgeon about the resorption surgery suggested by Dr Becker, a nurse wrote back that 'they don't do that kind of surgery', according to the Berkeley surgeon that Dr Nelson asked, there wasn't enough literature for him to rely on. It sounds like it has to be more text book protocol, than solutions that you invent when confronted by a problem not seen before that doesn't have a textbook solution yet. It is bizarre that so much of estabiished medicine is still more or less anecdotally established practices that too easily go unquestioined, while it would not pass an evidence based test according to a Cochrane Review.
The only other place I've found on the web mentioning the apicotomy technique is: orto-nova.hr
It is described as a routine surgical procedure:
Oral surgery is a discipline of dental medicine that includes a wide range of oral surgical procedures. In our
center we perform implantology procedures (implants installation), apicotomy (surgical removal of the root tip
from the tooth root), bone leveling (straightening the bone structures before surgery), operative extraction of
residual roots, the reconstruction of the aesthetic and functional defects of the mouth and other surgical
procedures in dental medicine.
This clinic is located in Croatia (hr= Republika Hrvatska)!
I asked Dr. Heithersay in Australia for an opinion about this technique, and he wrote that: I am not surprised by Dr Purcinelli's results as the pulp usually survives when an apex of a tooth is sectioned ( often unintentionally) in mandibular or maxillary osteotomies. The likely longer term response will be some calcification within the root canal- which generally is of no consequence.
Powerpoint presentation by DR Jae Park from the 2014 AAO meeting in New Orleans on the subject of 'Diagnosis and Treatment of Maxillary Canines using CBCT' which included a part on apicotomy and DR Puricelli:
|
|
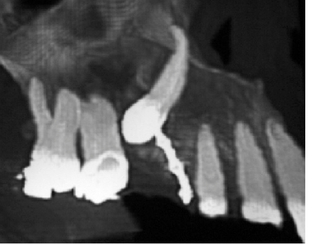
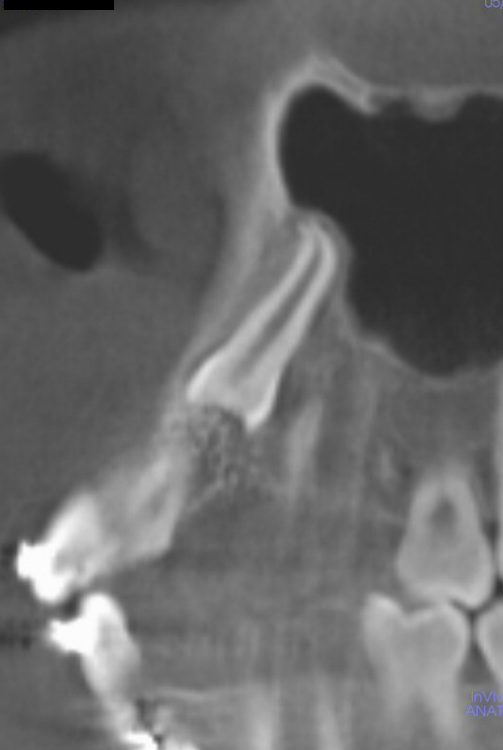
'Sam's case':
Images showing dilaceration (crooked apex) of impacted #6. Apicotomy was tried in September 2014. Traction was not on until after 2 weeks, which could be cause for failure.

|
|

|
|

|
Is apicotomy a valid technique or not?
Dr Becker analyzed 'the chicken and egg' question of apex dilaceration and impaction in his newletter of January
2016: 'Failure of eruption and the hooked root apex - cause and effect'. Dr Becker describes how the 'hook' can
develop biologically because of the tooth being impacted, rather than the tooth being impacted because of the hook. So, apicotomy is not uncontroversial, and as with much of issues with impacted canines and the whys and hows more studies would be welcomed.
2016: 'Failure of eruption and the hooked root apex - cause and effect'. Dr Becker describes how the 'hook' can
develop biologically because of the tooth being impacted, rather than the tooth being impacted because of the hook. So, apicotomy is not uncontroversial, and as with much of issues with impacted canines and the whys and hows more studies would be welcomed.
Partial Maxillary Osteotomy
The object of the Partial Maxillary Osteotomy is to move the whole segment of teeth behind the extracted canine forward. The teeth can stay in their place -not being dragged forward-
More articles by Dr. Puricelli:
'Partial maxillary apicotomy following an unsuccessful forced eruption of an impacted maxilary canine" (5) relates a case of a 17-year-old girl. In this case the canine had been under treatment for 31 months , the canine was extracted and the space was closed by PARTIAL MAXILLARY OSTEOTOMY. (I don't know why they first did not try apicotomy). This is the 'flow chart' for treatment of impacted canines by Dr Puricelli.
Radical treatment is recommended when conservative orthodontic or surgical techniques are unsuccessful or
contra-indicated. Usually when there is little to non-existing space for the canine and nearly acceptable
occlusion, orthodontic traction attempts that require great distal movements of the posterior teeth or
extraction of the first pre-molar should be avoided [1,4,9,15,19]. When orthodontic traction is attempted and
does not succeed, even with no clear observable obstruction, it is usually due to apical root dilacerations,
improper orthodontic force direction, surgical wire retentions or ankylosis 4,6,15,17.
When, after six months of orthodontic force application, the tooth does not show clear evidence of
movement, a re-evaluation is necessary. Orthodontic planning must be accessed. If the tooth is submerged,
surgical re-intervention is recommended [1,4,15]. If the canine's apical third is situated by the Enni's
inverted Y or if signs of apical root dilacerations are visible, an apicotomy, if not yet performed, must be
undertaken 18. If, after all these measures were accounted for with no prognosis of success, radical
treatment by means of extraction is recommended [9,19].
The object of the Partial Maxillary Osteotomy is to move the whole segment of teeth behind the extracted canine forward. The teeth can stay in their place -not being dragged forward-
More articles by Dr. Puricelli:
'Partial maxillary apicotomy following an unsuccessful forced eruption of an impacted maxilary canine" (5) relates a case of a 17-year-old girl. In this case the canine had been under treatment for 31 months , the canine was extracted and the space was closed by PARTIAL MAXILLARY OSTEOTOMY. (I don't know why they first did not try apicotomy). This is the 'flow chart' for treatment of impacted canines by Dr Puricelli.
Radical treatment is recommended when conservative orthodontic or surgical techniques are unsuccessful or
contra-indicated. Usually when there is little to non-existing space for the canine and nearly acceptable
occlusion, orthodontic traction attempts that require great distal movements of the posterior teeth or
extraction of the first pre-molar should be avoided [1,4,9,15,19]. When orthodontic traction is attempted and
does not succeed, even with no clear observable obstruction, it is usually due to apical root dilacerations,
improper orthodontic force direction, surgical wire retentions or ankylosis 4,6,15,17.
When, after six months of orthodontic force application, the tooth does not show clear evidence of
movement, a re-evaluation is necessary. Orthodontic planning must be accessed. If the tooth is submerged,
surgical re-intervention is recommended [1,4,15]. If the canine's apical third is situated by the Enni's
inverted Y or if signs of apical root dilacerations are visible, an apicotomy, if not yet performed, must be
undertaken 18. If, after all these measures were accounted for with no prognosis of success, radical
treatment by means of extraction is recommended [9,19].
(1) Edela Puricelli. Apicotomy: a root apical fracture for surgical treatment of impacted upper canines. Head
Face Med. 2007; 3:33.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2045087/?tool=pubmed
(2) Araújo EA, Araújo CV, Tanaka OM. Apicotomy: Surgical management of maxillary dilacerated or ankylosed
canines. Am J Orthod Dentofacial Orthop. Issue 6, 909-15, Dec 2013. PMID 242896914.
From the Center for Advanced Dental Education, Saint Louis University, St Louis, Mo.
(3) Ponzoni et al. Apicotomy and double traction: conservative interventions for impacted teeth. IJOMS. Vol 40,
issue 10, pp 1132-33, Oct 2011.
(4) Osório et al. Apicotomy as Treatment for Failure of Orthodontic Traction. Case Rep Dent 2013; 2013:
168232.
(5) Edela Puricelli.Partial maxillary osteotomy following an unsuccessful forced eruption of an impacted
maxillary canine. J Appl Oral Sci. 2012 Nov-Dec: 20(6): 667-672.
(6) M.C. Russo et al. Altered anatomy in a case with a buccally impacted maxillary canine tooth. Romanian
Journal of Morphology and Embryology 2010, 51 (4);783-786.
(7) https://www.aaoinfo.org/system/files/media/documents
Edela Puricelli is Professor and Head of the Department of Surgery and Orthopedics, Clinics Hospital of
Porto Alegre, School of Dentistry, Federal University of Rio Grande do Sul, Porto Allegro, Brazil.
*** Dr Jae Hyn Park is Program Director of the Post Graduate Orthodontic Program at the Arizona School of
Dentistry & Oral Health, Mesa, Arizona.
**** Apicoectomy means retrograde root canal treatment, as in killing the nerve and filling
up the pulp, after a root canal treatment has caused inflammation/infection. Dr. Puricelli's method leaves
the root intact and viable.
Face Med. 2007; 3:33.http://www.ncbi.nlm.nih.gov/pmc/articles/PMC2045087/?tool=pubmed
(2) Araújo EA, Araújo CV, Tanaka OM. Apicotomy: Surgical management of maxillary dilacerated or ankylosed
canines. Am J Orthod Dentofacial Orthop. Issue 6, 909-15, Dec 2013. PMID 242896914.
From the Center for Advanced Dental Education, Saint Louis University, St Louis, Mo.
(3) Ponzoni et al. Apicotomy and double traction: conservative interventions for impacted teeth. IJOMS. Vol 40,
issue 10, pp 1132-33, Oct 2011.
(4) Osório et al. Apicotomy as Treatment for Failure of Orthodontic Traction. Case Rep Dent 2013; 2013:
168232.
(5) Edela Puricelli.Partial maxillary osteotomy following an unsuccessful forced eruption of an impacted
maxillary canine. J Appl Oral Sci. 2012 Nov-Dec: 20(6): 667-672.
(6) M.C. Russo et al. Altered anatomy in a case with a buccally impacted maxillary canine tooth. Romanian
Journal of Morphology and Embryology 2010, 51 (4);783-786.
(7) https://www.aaoinfo.org/system/files/media/documents
Edela Puricelli is Professor and Head of the Department of Surgery and Orthopedics, Clinics Hospital of
Porto Alegre, School of Dentistry, Federal University of Rio Grande do Sul, Porto Allegro, Brazil.
*** Dr Jae Hyn Park is Program Director of the Post Graduate Orthodontic Program at the Arizona School of
Dentistry & Oral Health, Mesa, Arizona.
**** Apicoectomy means retrograde root canal treatment, as in killing the nerve and filling
up the pulp, after a root canal treatment has caused inflammation/infection. Dr. Puricelli's method leaves
the root intact and viable.