Autotransplantation provide patients with all the benefits of a natural tooth,
but is seldom considered as a treatment option,
in large part because of lack of knowledge about periodontal tissue or the anatomy of teeth.(12)
but is seldom considered as a treatment option,
in large part because of lack of knowledge about periodontal tissue or the anatomy of teeth.(12)
AUTO TRANSPLANTATION, AUTOGENOUS TRANSPLANTATION or ADT=Autogenic Dental Transplantation
Besides Dr Brånemark and implants, another Swede was a pioneer of auto transplantaton of teeth (1915),
Dr Vidman, a surgeon. But, from what I've read, it already made sense, at least in theory, to Egyptian pharaohs, who tried using slaves as donors.
Dental trauma of different kinds must be something that has given a lot of experience as to how well a tooth
responds to being moved and then put in place and stabilized, it is not to far off to purposely taking out a tooth and reimplanting it, but in this case a new site needs to be prepared.
Besides Dr Brånemark and implants, another Swede was a pioneer of auto transplantaton of teeth (1915),
Dr Vidman, a surgeon. But, from what I've read, it already made sense, at least in theory, to Egyptian pharaohs, who tried using slaves as donors.
Dental trauma of different kinds must be something that has given a lot of experience as to how well a tooth
responds to being moved and then put in place and stabilized, it is not to far off to purposely taking out a tooth and reimplanting it, but in this case a new site needs to be prepared.
|
Auto transplantation is moving a tooth surgically to a new position.
If the osteotomy's purpose is to help and loosen the tooth a bit, this is to radically take the tooth out, but carefully minding the periodontal ligament. Then prepare a socket to place it in asap, in slight infra occlusion so it can erupt. The transplant is held in place with 'suture splint', resin or a temporary bridge. Results are better if the root is only between 50 and 75% formed (5) according to one author, Dr. Pamela L. Alberto***. If the root is fully developed it sounds as if a root canal is performed two weeks after the transplantation. |
http://www.intelligentdental.com/2012/01/18/impacted-teeth-part-2/ (this is a weird website, with scattered, unsubstantiated information, no reference of where it comes from or who is behind it and down-right misinformation - the blessings and downfall of the web! don't get caught in it! - but I thought the image worthwhile)
|
As you can read below, several authors want to make auto transplantation an option when solving the problem of absent teeth and impacted teeth. The 'Practitioner's corner' of the pcsortho.org interviewed Dr Jim Janakievski
(periodontist at University of Washington) about it in the Fall issue 2010:
There are many studies on tooth autotransplantation. It has been most extensively studied in Scandinavia. A
recently published long-term review of cases had a follow-up range of 17 to 41 years (5). The success rate
was over 90%, which is similar to that of dental implant-supported restorations.
There are descriptions of a premolar taking the place of a traumatically lost maxillary central incisor, and an impacted central incisor where the tooth was just transplanted down. On the question of where you can take a course in auto transplantation the answer was:
There are no courses available at this time. I have been invited to present on this topic to several study clubs
and academies. We are hoping to put together a course in the next 2 years that would cover the surgical,
orthodontic, and restorative aspects of autotransplantation.
'Survival and success of maxillary canine autotransplantation: a retrospective investigation' (3) from 2010 is a review of 63 maxillary canine autotransplantations in 49 subjects, mean age of subjects 21.8 years, range 13-42.1. The survival rate was 83% with an average duration of 14.5 years in situ. 38% were deemed succesful.
'All teeth were transplanted when root development was complete'.
With the introduction of osseointegrated implants and advanced dental adhesives for resin retained bridges,
autotransplantation has increasingly been overlooked as a treatment option,; however, both these restorative
options have problems associated with them...
An important question is whether a role for maxillary canine autotransplantation still exists, particularly when
reported success rates for osseointegrated implants range from 79.2 to 98.5 per cent over a 4-8 year period
and when non-invasive resin retained bridges can be recemented or replaced without deleterious effects on
adjacent teeth. This study found that 38 per cent of autotransplanted canines were successful, displaying no
signs of resorption or mobility and sound periodontal tissues, while 83 per cent were still in situ. Theses teeth
were transplanted with closed apices and were still present on average after after 14.5 years. This is
comparable to a 79.2-98.5 per cent over a 4-8 year period and better than the survival rate of less than 10
years for resin retained bridges. However, even with this comparable survival, a success rate of 38 percent
must be regarded as low, especially when single-tooth implants are associated with success rates of 90 per
cent or more. However, there are currently few long-term studies evaluating implant performance in the
maxillary canine region.
Conclusion:
Autotransplantation of impacted maxillary canines may be indicated in selected circumstances, but a low
long-term success rate should be expected. Individual success is difficult to predict and patients must be
informed of the potential for failure and associated risks before undergoing such a
procedure.Autotransplantaion of canines should be considered in patients who are unwilling to undergo
lengthy orthodontic treatment to accommodate ectopic canines, particularly if there is an otherwise mild
malocclusion as this approach could obviate the need for orthodontic treatment. The procedure is technique
sensitive and success rates are higher in teeth with an open apices. Autotransplantation can be considered
an interim measure to maintain bone levels during facial growth prior to the placement of osseointegrated
implants.
So even a canine that eventually fails will hold the place for a future implant if necessary.
Autogenous Tooth Transplantation: An Alternative to Dental Implant Placement? (4) from Toronto 2001 presents 3 cases of molars that are replaced with other molars because of impaction, caries and periodontitis.
They also report other articles' finds on the subject:
The literature reports excellent success rates following tooth transplantation when the appropriate protocol is
followed. Andreassen found 95% and 98% long-term survival for incomplete and complete root formation of
370 transplanted premolars observed over 13 years. Lundberg and Isaksson had success in 94% and 84% of
cases for open and closed apices respectively in 278 autotransplanted teeth over 5 years. Kugelberg achieved
success rates of 96% and 82% for 45 immature teeth transplanted into the upper incisor region over 4 years.
Cohen showed success rates in the ranges of 98-99% over 5 years and 80-87% over 10 years with
transplanted anterior teeth with closed apices. Nethander found 5-year success rates of over 90% for 68
immature teeth transplanted with a 2-stage technique. Josefsson found 4-year-success rates of 92% and
82% respectively for premolars with incomplete and complete root formation.
They write of the importance of alveolar support:
The most important criteria for success involving the recipient site is adequacy of bone support. There must
be sufficient alveolar bone support in all dimensions with adequate attached keratinized tissue to allow for
stabilization of the transplanted tooth. In addition, the recipient site should be free from acute infection and
chronic inflammation.
According to the article the main reason for failure is chronic root resorption.
Conclusion:
Although autotransplantation has not been established as a traditional means of replacing a missing
tooth, the procedure warrants more consideration. Recent studies clearly demonstrate that
autotransplantation of teeth is as succesfull as endosseous dental implant placement. Minimum acceptabel
success rate for endosseous dental implants are 85% after 5 years and 80 % after 10 years. For younger
patients, autotransplantation may also be considered a temporary measure. The transplant can replace
missing teeth to ensure preservation of bone until growth has ceased and then, if necessary, the patient can
become a candidate for implants. With appropriate patient selection , and presence of a suitable donor tooth
and recipient site, autogenous transplantaion should be considered a viable optiion for treatment of an
edentulous space.
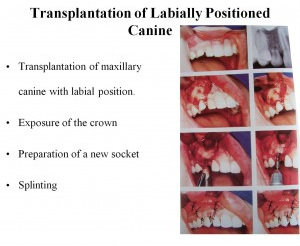
Even though transplantation doesn't seem a new thought or technique a power point presentation by Dr Suhasis Mondal (Kolkata, India) titled AUTOGENIC DENTAL TRANSPLANTATION - THE NEW ALTERNATIVE TO PROSTHETIC REPLACEMENTS.Slideshare.net shows some points (from OOOOE, Journal of Oral Surgery Oral Medicine Oral Pathology, Volume 106, Nov 4) of
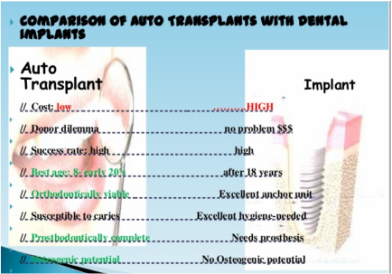
From Dr Mondal's slideshare
|
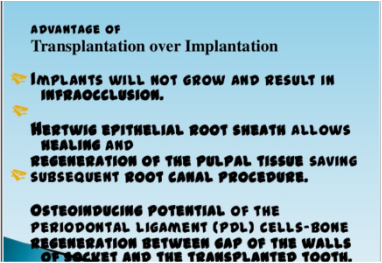
From Dr Mondal's slideshare
|
'Tooth Autotransplantation as a Treatment Option: A Review" by Dr Jae Park et al.looks at mostly Japanese and Swedish articles on transplantation. (12). It mentions an article on maxillary canines (2) where a 5 year follow up 32 canines in 30 subjects, showed a 93.5% survival rate and the conclusion that maxillary transplantation can be a reliable treatment option. Dr Park et al. concludes their review of literature with:
Autotransplantation of teeth offers a new treatment option for some clinical situations. It permits tooth
movement to distant or opposite sides of the same dental arch, as well as the opposite jaw.
Furthermore, transplantation offers other potential benefits such as bone induction and the reestablishment of
a normal alveolar process in addition to tooth replacement. Even if the transplant fails later, there is an intact
recipient area that could be used for an implant. A prerequisite is for this method, however, is a thorough
knowledge of the factors that influence the long-term success rate. If done properly, this method may
supplement and or be used as a viable treatment option in present day clinical practice.
(I wrote Dr Park and asked him, as editor of the magazine for the Pacific Coast Society of Orthodontists, www.pcsortho.org, and to put in a letter from me asking for an effort to get transplantation as an available option for teens with impacted canines. He replied he'd take it under consideration, but never published anything.
I think it is unfortunate that a patient's perspective is not welcome, I think it could have been an eye opener to
the dental professionals, if they tried to understand the conseqence of not having a proper treatment plan and
team efforts when dealing with impacted canines.
An expert on dental transplantation is Dr. Jens O. Andreasen an oral surgeon in Copenhagen. He is mainly a specialist in trauma and has a wonderful website: dentaltraumaguide.org for when you are a parent faced with this problem.
Dr. Heithersay, an endodontist in Adelaide, Australia, renowned for his work on different resorptions in teeth, describes two cases of transplantation in patients with PEIR, if you look under 'Sam's case'.
In our endodontic clinic we have treated two cases with similar histories of frustrated orthodontic treatment
where no movement could be activated despite similar coronal exposure as that carried out for Sam . One
of these cases also had pre-eruptive invasive coronal resorption. After a multidisciplinary consultation
involving an orthodontist, and a peridontist and our endodontic group, it was decided in both cases to treat
the unerupted teeth be intentional transplantation, with concurrent treatment of the resorptive defect and
endodontic treatment in the case with pre-eruptive invasive coronal resorption. The teeth were very carefully
removed surgically with special attention to avoid damage to the root surface. Before the teeth were
transplanted into a newly created socket site, the root sufaces were treated with Emdogain and after
transplantation, the bone defect was filled with a combination of Bio-oss and Collagen and the area was then
covered with Bioguide which is a resorbable membrane. In the tooth without the pre-eruptive invasive
coronal resorption, endodontic treatment was commenced prior to the transplantation, but an intra-canal
dressing was placed incorporating a cortico-steroid antibiotic combination as this has been shown to control
potential resorption. The tooth will be root filled after some weeks.
The patient with the pre-eruptive resorption has been followed up for two years to date and there has been
excellent progress.
Transplantation of unerupted canines is not a new technique- it has been used for many years- an
orthodontist named Moss published an impressive series in the early 70's while an extensive study has been
carried out by Dr Jens Andreasen of Copenhagen- he and his surgical team have very impressive results.
Actually it doesn't seem that autotransplantation is much of a thing in the US, but I find quite a few Swedish articles on the subject, for example:
'Autotransplantation of Teeth in 215 Patients' from the the Orthodontic Department in Jönköping , Sweden, 2010. 81 % were successful, 19 % unsuccessful. 31 of the teeth were impacted maxillary canines, the success rate was 84%. (10)
Dr Björn Zachrisson describes a case of traumatic loss in an 11-year-old girl in 'International Dentistry SA'(1). The teeth were first put back in but then deemed ankylosed and removed.The canine is moved to sub for a central and lateral incisor and the premolar takes the place of the canine the photos post treatment look very good.
A British paper from the University in Leeds, 2012:
Background: Tooth auto-transplantation has been successfully performed for over 50 years and yet the procedure has still to receive the widespread acceptance that it deserves.
AIM: This study demonstrates the numerous clinical situations in which auto-transplantation can be used in order to give a child or adolescent an excellent biological long-term replacement.
INDICATIONS: Seven cases are presented that demonstrated the versatility of auto-transplantation in a range of clinical situations. The aim was to show that this technique is not only useful for replacing teeth that are lost due to trauma but has applications for the replacement of teeth that are developmentally missing, or teeth with otherwise poor long-term prognosis. TREATMENT: All cases presented were managed with autotransplantation and included patients with hypodontia, trauma, dilacerated incisors, ankylosis, failed endodontic treatment and aesthetic management of a patient with cleft lip and palate. FOLLOW-UP: Medium and long-term outcomes were demonstrated. CONCLUSION; Auto-transplantation provides an excellent outcome in a growing child with the advantage that it is a biologically compatible method of tooth replacement, which promotes pulp and periodontal healing and enables orthodontic movement if necessary. (13)
All of these testimonies, 50 years of experience, so why not???
(1) Björn Zachrisson. Planning esthetic treatment after traumatic avulsion of maxillary incisors
J Am Dent Assoc, 139:1484-1490, 2008.
(10) Kvint S, Lindsten R, Magnusson A, Nilsson P, Bjerklin K. Autotransplantation of Teeth in 215 Patients. The
Angle orthodontist: May 2010, Vol 80, No 3, pp 446-451)
(2) Anrikan F et al. 5-year-longitundinal study of survival rate and periodontal parameter changesat site of
maxillary canine autotransplantation. J Period, 79: 595-602, 2008.
(3) Sonal Patel et al. The European Journal of Orhtodontics.DOI:http://dx.doi.org/10.1093/ejo/cjq071
The authors are British.
(4) Clokie C et al. Autogenous Tooth Transplantation: An Alternative to Dental Implant Placement?' J Can Dent
Assoc 2001; 67:92-6
(12) Jae Hyun Park, Kiyoshi Tai, Daisuke Hayashi. Tooth Autotransplantation as a Treatment Option: A Review. J
Clin PEDIATR DENT 35(2); 129-136, 2011.
(13) K. Waldon et al. Indications for the use of autotransplantation of teeth in the child and adolescent.
European Archives of Paediatric Dentistry. August 2012, Vol 13, Issue 4, pp 210-218.
Study from Leeds Dental Institute, Leeds, England.
(5) Czochrowska EM, Stenvik A, Bjercke B, Zachrisson BU. Outcome of tooth transplantations: survival and
success rates 17-41 years posttreatment. Am J Orthod Dentofac Orthop. 2002;121(2):110-119.
(9) http://www.actiradentes.com.br/revista/2012/textos/12RevistaATO-Canine_Transplantation-2012.pdf
J Am Dent Assoc, 139:1484-1490, 2008.
(10) Kvint S, Lindsten R, Magnusson A, Nilsson P, Bjerklin K. Autotransplantation of Teeth in 215 Patients. The
Angle orthodontist: May 2010, Vol 80, No 3, pp 446-451)
(2) Anrikan F et al. 5-year-longitundinal study of survival rate and periodontal parameter changesat site of
maxillary canine autotransplantation. J Period, 79: 595-602, 2008.
(3) Sonal Patel et al. The European Journal of Orhtodontics.DOI:http://dx.doi.org/10.1093/ejo/cjq071
The authors are British.
(4) Clokie C et al. Autogenous Tooth Transplantation: An Alternative to Dental Implant Placement?' J Can Dent
Assoc 2001; 67:92-6
(12) Jae Hyun Park, Kiyoshi Tai, Daisuke Hayashi. Tooth Autotransplantation as a Treatment Option: A Review. J
Clin PEDIATR DENT 35(2); 129-136, 2011.
(13) K. Waldon et al. Indications for the use of autotransplantation of teeth in the child and adolescent.
European Archives of Paediatric Dentistry. August 2012, Vol 13, Issue 4, pp 210-218.
Study from Leeds Dental Institute, Leeds, England.
(5) Czochrowska EM, Stenvik A, Bjercke B, Zachrisson BU. Outcome of tooth transplantations: survival and
success rates 17-41 years posttreatment. Am J Orthod Dentofac Orthop. 2002;121(2):110-119.
(9) http://www.actiradentes.com.br/revista/2012/textos/12RevistaATO-Canine_Transplantation-2012.pdf
If Sam had been living in Canada, Australia, Denmark or some other place with an auto transplantation interested orthodontis & surgeon team, maybe his upper canine could have been transplanted after one or two attempts of traction and it would have saved many years, many dollars...What makes the US so intent on putting implants in every one.
Faced with a 14-year-old and an impacted maxillary canine, why would not a try at autotransplantation be worth it compared to waiting 4, or 5, or more years, while the alveolar bone wasted away, to put in an implant. 'Lack of knowledge about periodontal tissue or the anatomy of teeth'...really! Patients, children, are being denied this
treatment because American dental professionals don't understand teeth!
Faced with a 14-year-old and an impacted maxillary canine, why would not a try at autotransplantation be worth it compared to waiting 4, or 5, or more years, while the alveolar bone wasted away, to put in an implant. 'Lack of knowledge about periodontal tissue or the anatomy of teeth'...really! Patients, children, are being denied this
treatment because American dental professionals don't understand teeth!