Part 4: from April 2014 and ongoing
THE POST-JERUSALEM ERA: Back in the Bay Area
|

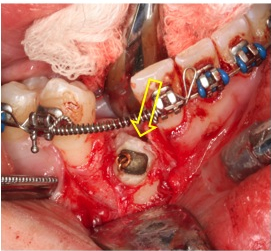
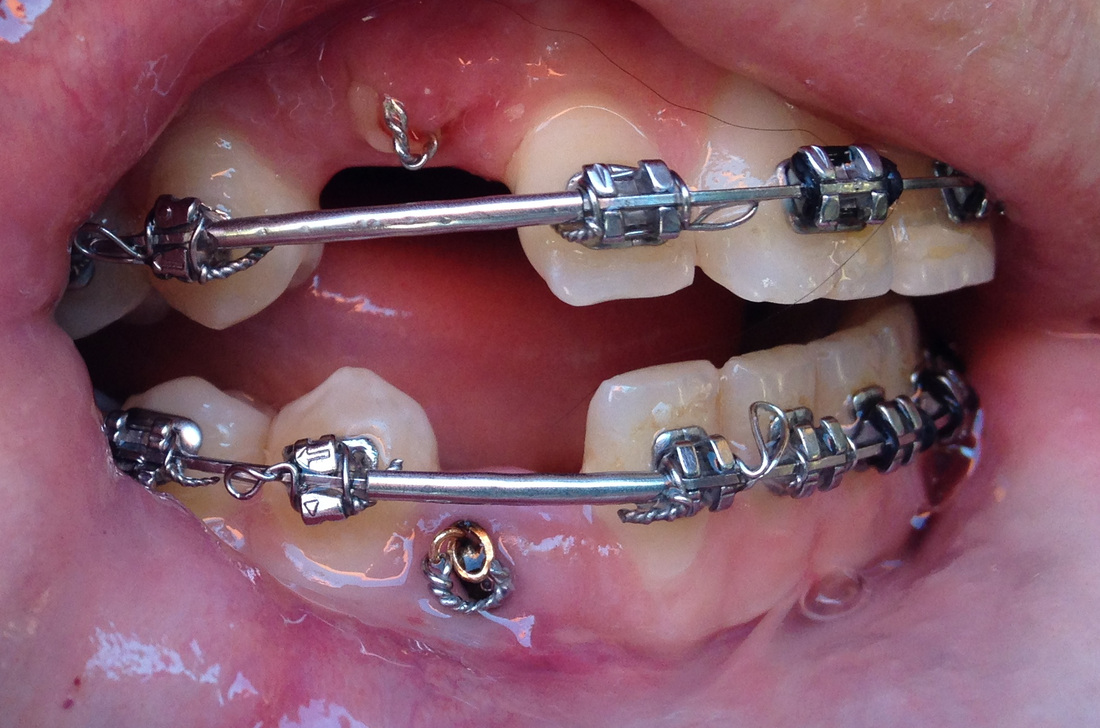
March 6, 2014. One day post surgery #3.
|
|
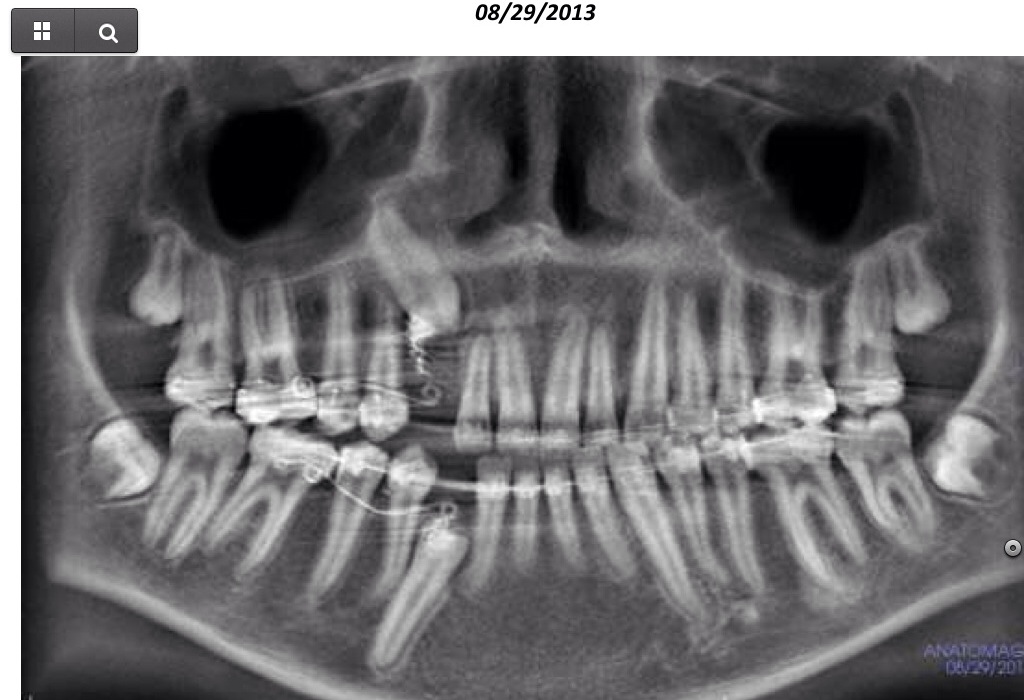
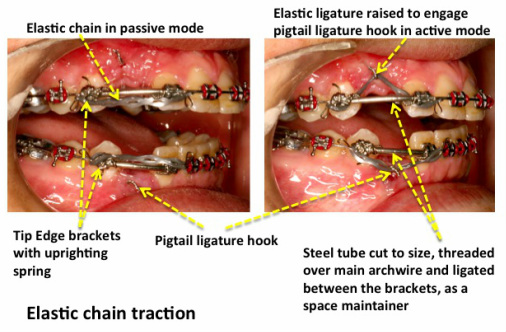
The set-up: Sam's third expose & bond included repairing the (atypical) PEIR with glass ionomer, under the theory that the osteoblast/osteoclast activity in the resorption was impeding the extrusion, similar to ICRR. (Dr Becker took a biopsy, that was unfortunately lost). The attachment on the upper canine was found to be loose at surgery, so there is a new one there, the lower one is from the 2012 surgery. Dr Becker put new brackets on the premolars to have them uprighted. The space for the teeth that had diminished under Dr. Nelson's treatment are now kept open with 'space maintainers', to give the canines room in the arch. Dr. Becker recommends changing the elastic chain every 10-14 days since because of material fatigue. |
("The Beamreader' analysis of the CBCTs was that "the available interproximal space for #6's propoer eruption/traction was not enough due to #6's angulation/position."
"The biomechanic direction of the forced eruption should be considered as a contributor factor for the slow eruption process". ' |

|
We thankfully have a new orthodontist*, Dr James Chen in San Mateo (not to be confused with our first Dr James Chen at UCSF in Part 2). I am hoping this will be a fresh new start!
First visit with Dr. Chen, April 2: 4 weeks post-op, and 2 weeks after Dr. Becker's last adjustment in Jerusalem and the photos above. The lower elastic slacking a bit. Sam lost the Kobayashi hook on the upper lateral incisor the day before, so it had to be replaced. Dr. Becker's plan was that "any progress that hopefully occurs will be recognized by the fact that the hook be rolled up and shortened in line with this progress and a new chain substituted every 10-14 days." |

|
Visit April 16: 6 weeks post-op
The elastic dropped off the lower hook yesterday, and Sam couldn't get it back on. Dr Chen is trying a wire that goes through the eyelet on #27. |
|
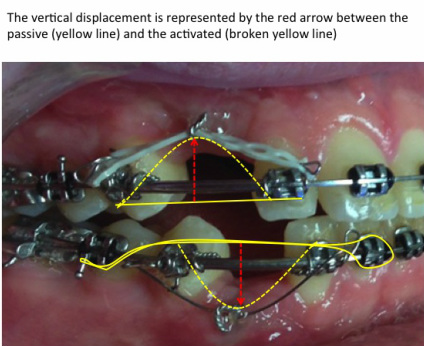
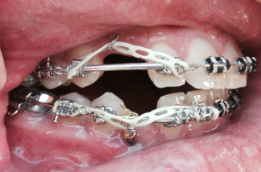
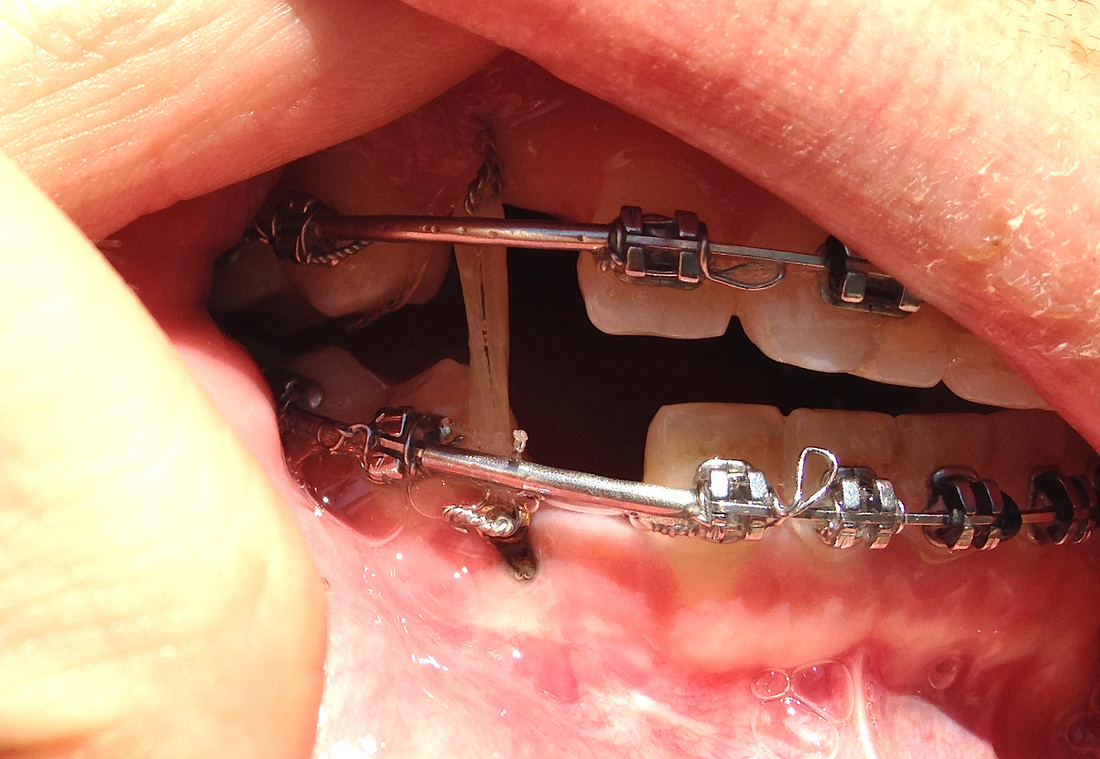
Dr. Becker looks at the photos from April: The most important factor for a horizontal elastic or wire to be able to generate adequate vertical traction is to have a reasonable height differential between the horizontal passive state of the elastic/wire and the vertical displacement when engaged in the hook. I agree that the April 2 picture does not have much of a vertical displacement and the new wire is better. It would be better still if it had been threaded above the bracket on the first premolar and the lateral incisor. The most important attribute of the wire (nickel-titanium) is that it must run freely in the other brackets, otherwise the vertical displacement will jam in the brackets and not not provide any vertical force. I am a great believer in simplicity and, although elastic chains lose their elasticity over a period (which is why I recommended changing them every 10-14 days) I would now place a chain from the lower hook on the second premolar and run it above the brackets of the first premolar and lateral incisor (to increase the vertical displacement) and stretch the last link of the chain on the next tooth, the central incisor. Similarly, in the upper jaw, you will notice that the Kobayashi hooks are now gingival, whereas I had placed them incisally. This has lessened the vertical displacement. |

Sam: April 16, 2014
|
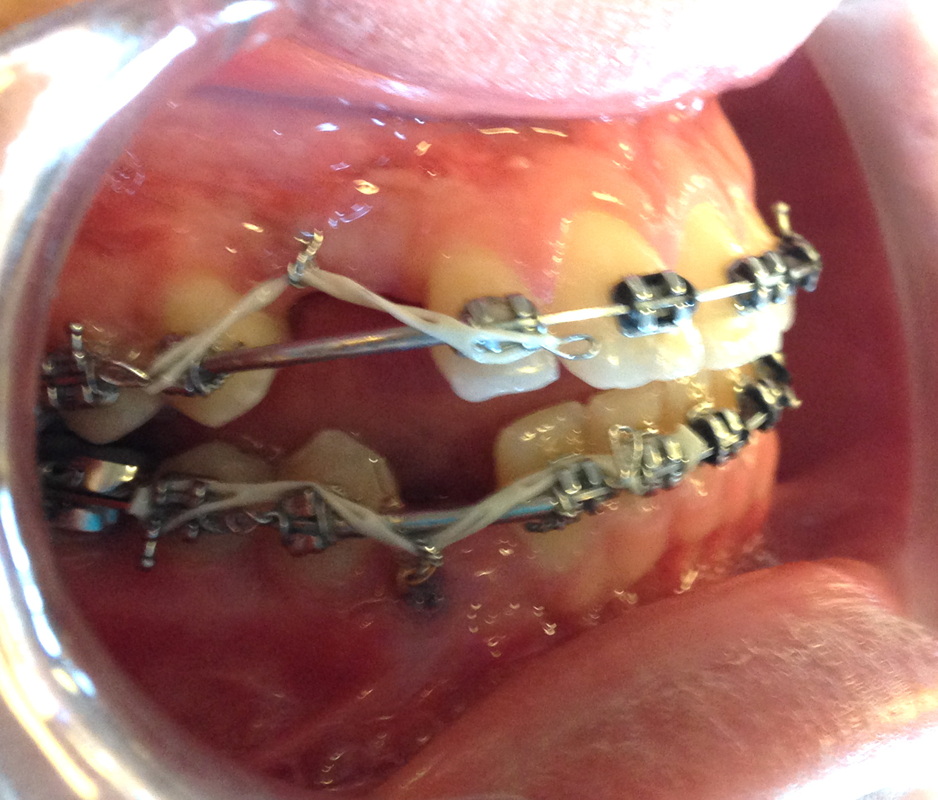
The purple outlines Sam's auxilary wire. I can't see how far the wires extend in each direction (Sam isn't about to let me poke around),but Dr. Chen says they go all the way along the arch wire. |

Sam: April 23, 2014
|
Visit April 23: 7 weeks post op
Changing back to the power chain. Trying to get the elastic chain on the lower hook. |

Sam: May 1, 2014.
Dr Becker's image, not Sam.
|
Image May 1st, 2014. 8 weeks post op.
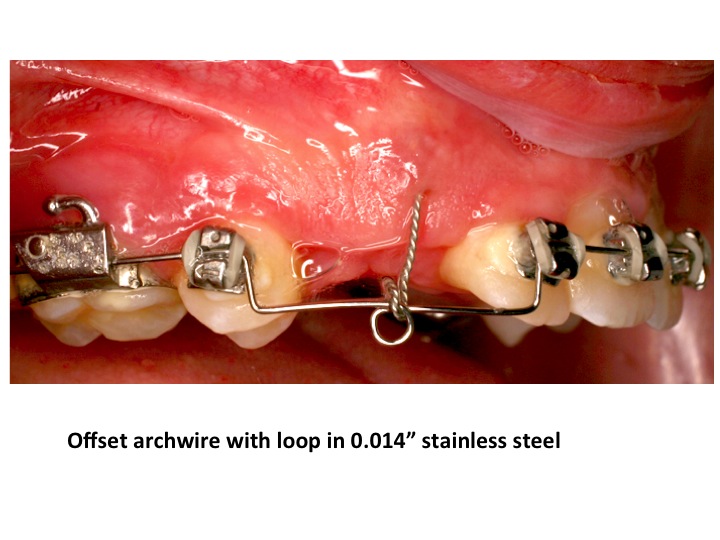
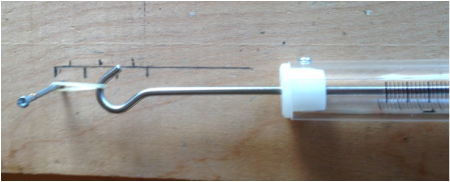
Lower elastic chain now slack, hopefully a sign of progress, but we have no extruding force! Dr. Becker's advice: Vertical traction can be re-established in 2 ways: 1. The lower chain is removed and the twisted steel ligature hook is rolled down on itself, to create a greater height differential and a new chain placed as before or better still, tied on the occlusal (upper) wing of the brackets of the adjacent teeth. 2. changing the archwire to a 0.018" round stainless steel wire or equivalent rectangular wire with a pair of vertical and horizontal right angle bends against the two adjacent teeth, thereby raising that section of the archwire a little higher and bending a small circle in it. The tie would then be made with elastic thread direct to the circle in the mid-section of that wire. Alternatively, an 0.014" round wire may be bent in this way and the tie being made with a steel ligature - see figure herewith. Either way, it would be a good idea to start getting round to finding a way to supplement these forces with vertical elastics, as in the past. I would hope and expect that there will not be any need for further surgery and simply opening up the gum will not be advantageous. In the meantime we must wait to see some encouraging signs from the upper canine. The eyelet is far easier from several points of view than placing a bracket at this stage. I would only substitute the eyelet for a bracket when the tooth has fully erupted to the occlusal level - to do whatever finishing may be necessary. ... The pigtail is firm enough and should not unravel. The vertical legs of the offset will hold the space and activating the offset by ligating with elastic or stainless steel will actually increase it. |
|
Visit May 7th, 9 weeks post op.
New chains. The lower canine also got a transparent elastic going from the eyelet to the arch wire. The lower chain goes on top of the adjacent brackets, so hopefully that gives more traction. Dr Chen wants to put a wire in next time. |


|
Sam, 10 weeks post op.
|
11 weeks post op, Visit: May 20.
|

Sam 11 weeks post op
|
Dr Chen:
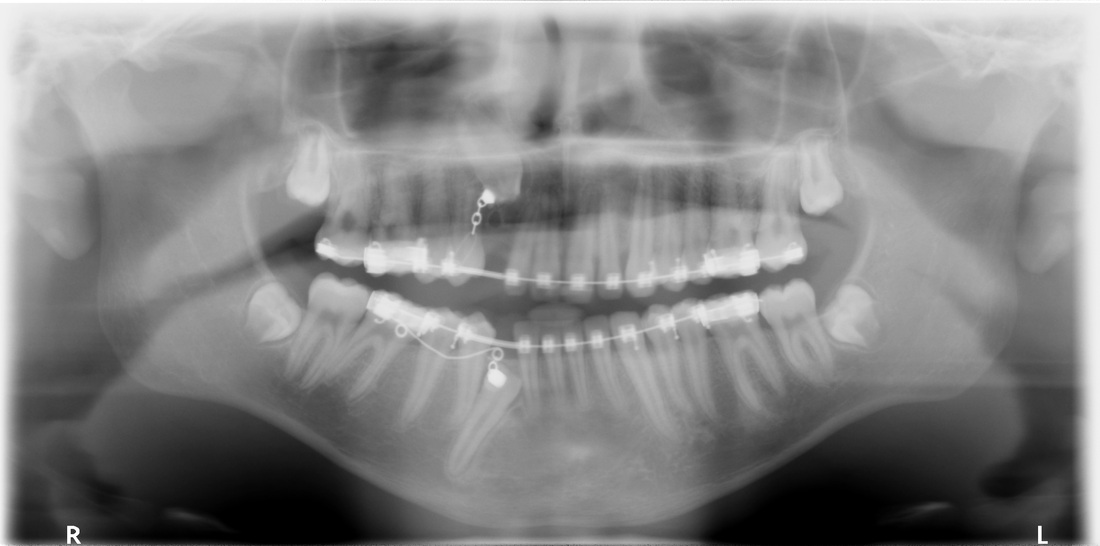
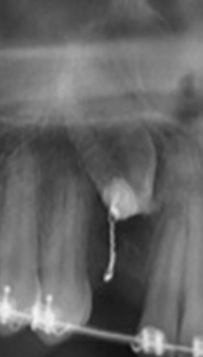
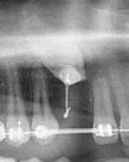
I took a pano for Sam today. Compared with his previous pano, it looks like the lower impacted canine has been extruded out of socket. Hopefully there will be more promising result to come.
Dr Becker:
This is excellent news. The tooth is not being pulled out of its socket. What is happening is that the tooth is responding to the orthodontic traction and new bone is filling in behind the advancing tooth. This bone is young and relatively hypocalcified in its early stages and, therefore, largely radiolucent, giving the impression of being drawn out of its socket. This will calcify as the bone matures and the visible outline of the former socket will become more and more blurred.
I am, however, concerned regarding the maxillary canine which does not seem to have moved - although comparison with the January 2014 film (clearly taken at a different positional setting) and the CBCT is a little misleading. Please keep on going!
I took a pano for Sam today. Compared with his previous pano, it looks like the lower impacted canine has been extruded out of socket. Hopefully there will be more promising result to come.
Dr Becker:
This is excellent news. The tooth is not being pulled out of its socket. What is happening is that the tooth is responding to the orthodontic traction and new bone is filling in behind the advancing tooth. This bone is young and relatively hypocalcified in its early stages and, therefore, largely radiolucent, giving the impression of being drawn out of its socket. This will calcify as the bone matures and the visible outline of the former socket will become more and more blurred.
I am, however, concerned regarding the maxillary canine which does not seem to have moved - although comparison with the January 2014 film (clearly taken at a different positional setting) and the CBCT is a little misleading. Please keep on going!
Extract, extrude or erupt - ortho lingo
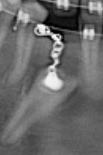
#27 has left the socket, the radiolucency around the apex makes it look like a ship leaving its berth. This can be interpreted alternatively as 'deleterious changes' and 'bad' 'extrusion out of socket' if new bone is not filling in the space behind # 27, or as a positive effect of traction, if there is new bone following the canine up, and it is about to erupt...I deduct that 'extrude' can be good or bad, extract bad, and 'erupt' good...
Hopefully this is the good kind like Dr Becker says. (Funny how 'more promising' can actually mean two very different things depending on how you emphasize it.)
The gap in beween the upper and lower teeth on the right side is a 'lateral open bite'. This can be prevented/treated by putting intermaxillary (in between the jaws) elastics. Dr Chen says he is waiting for the canines erupt before doing anything to Sam's open bite.
Problem with panoramas is the distortion. Is there enough room for the #27 to erupt?
#27 has left the socket, the radiolucency around the apex makes it look like a ship leaving its berth. This can be interpreted alternatively as 'deleterious changes' and 'bad' 'extrusion out of socket' if new bone is not filling in the space behind # 27, or as a positive effect of traction, if there is new bone following the canine up, and it is about to erupt...I deduct that 'extrude' can be good or bad, extract bad, and 'erupt' good...
Hopefully this is the good kind like Dr Becker says. (Funny how 'more promising' can actually mean two very different things depending on how you emphasize it.)
The gap in beween the upper and lower teeth on the right side is a 'lateral open bite'. This can be prevented/treated by putting intermaxillary (in between the jaws) elastics. Dr Chen says he is waiting for the canines erupt before doing anything to Sam's open bite.
Problem with panoramas is the distortion. Is there enough room for the #27 to erupt?
|
|




|
12 weeks post op
|

|
Visit June 3, 13 weeks post op
Dr Chen discontinued the power chains and is only doing a 'fish line' elastic string. He did not say why. I asked about the vertical elastics for the open bite. Dr Chen said they would not work now. The force would not be enough working against the two main arch wires. |
|
Dr Becker's suggestions:
I am not concerned about the open bite, because this will close down rapidly if and when up-and-down elastics are used. The likelihood of later need for surgery to close it down is virtually nil. Still the most important aim must be directed at bringing down the canines. It seems to me that both twisted ligature hooks from the impacted canines are easily accessible now. I think the system should be changed with Sam and/or mother taught to place a vertical elastic directly from one hook to the other. If there is some difficulty, the hooks may be altered in shape or rolled up slightly to achieve this. If the hooks begin to irritate the cheek mucosa, then they may be coated with composite material to stiffen them and to offer a smooth non-irritant outline. Then Sam could place 3/16" medium |
or heavy elastics in up-and-down fashion himself and change the elastics daily. This would give a good extrusive force of wide range and renewed on a daily basis to overcome force degradation that is present with the ties on the picture, which are of very short range and quickly neutralized.The big advantage of this is that there are no reactive forces on the neighboring teeth and, therefore, no adverse effect tending to further open the bite. If he gets on well with these, then he could additionally place a second up-and-down elastic (1/4" or 5/16" medium) around the 4 Kobayashi hooks on the lateral incisors and first premolars, to close down the bite - but I consider this to be of secondary importance at the present time and could be delayed till later. |
The exact traction force is not critical, but continuous 24/7 pull, including during meals, certainly is.
Summer of 2014 and the long search for orthodontist...oral surgeon...
6/12/2014: STATE OF EMERGENCY!
Unexpected turn of events. Email from Dr Chen. Turns out he has considered his treatment to be of a 'transitional' character and he can no longer help us: "I feel there are discrepancies in both clinical and practical perspectives that I did not forsee and now feel it is hard to work out....I am very sceptical about extruding his upper canine" He writes he took Sam on because of his case being connected to UCSF. To Dr Becker he wrote that he worked on Sam because of 'academic interest'.
What orthodontist walks away, when an impacted canine, Sam's lower canine, is about to erupt after 3.5 years! (Or rather, for the purpose of finding a new orthodontist, how am I supposed to explain that we were abandoned at this point!)
I believe Dr Chen has forgotten about his ethical obligation to a patient. We are in a very difficult situation now trying to find a new orthodontist asap! Sam has no orthodontist, and as the AAO transfer protocol says:
"Of paramount importance is the identification of an orthodontist who will accept the patient and successfully complete the treatment"
6/12/2014: STATE OF EMERGENCY!
Unexpected turn of events. Email from Dr Chen. Turns out he has considered his treatment to be of a 'transitional' character and he can no longer help us: "I feel there are discrepancies in both clinical and practical perspectives that I did not forsee and now feel it is hard to work out....I am very sceptical about extruding his upper canine" He writes he took Sam on because of his case being connected to UCSF. To Dr Becker he wrote that he worked on Sam because of 'academic interest'.
What orthodontist walks away, when an impacted canine, Sam's lower canine, is about to erupt after 3.5 years! (Or rather, for the purpose of finding a new orthodontist, how am I supposed to explain that we were abandoned at this point!)
I believe Dr Chen has forgotten about his ethical obligation to a patient. We are in a very difficult situation now trying to find a new orthodontist asap! Sam has no orthodontist, and as the AAO transfer protocol says:
"Of paramount importance is the identification of an orthodontist who will accept the patient and successfully complete the treatment"
(Pursuing a note Nov 13, 2013 by Dr Nelson that Dr Eraso at Beamreaders had suggested he'd do a 'digital image' 'Anatomodel', that evidently Dr Nelson didn't follow up on, I had contacted Dr Eraso to get this done. Dr Eraso said would cost an extra $ 100, but it required a referral from treating orthodontist, which is why he wrote an email to Dr Chen on June 12th, 3 hours after Dr Chen wrote to cancel his services, so nothing came of this...)
|
DIY Ortho
We used old 4mm elastics that Sam had since his days at UCSF. He could hook it on himself on the upper hook. The lower hook has been cut down I think by Dr Chen to the point where it is useless. We have to use fishing line to tie the elastic onto the eyelet. Making the fish line just long enough is the trick. There has to be tension when the jaws are together, but Sam still has to be able to eat and talk. I've ordered a dynamometer to get more scientific (not that I've ever seen an orthodontist actually measure the force of traction, but in the literature it says that that you need about 50-60 grams.) This is probably the last thing a 16-year-old needs. His mom hovering above his face, and in his mouth, with tweezers and sewing scissors. As Dr Chen wrote after dismissing us: Best of Luck |

|
6/14. Second day of DIY Orthodontics. Dr Becker isn't happy about the situation.
The main objective until someone professional takes over: The exact traction force is not critical, but continuous 24/7 pull, including during meals, certainly is. We are doing as best we can. We've been put in an emergency situation. Sam thought the 4 mm superheavy was a bit too much yesterday, so we are trying some other old leftover elastics, 6 mm heavy 4 oz (1/4"). Also trying a second oblique elastic to pull in the direction of the long axis of #6. It breaks when Sam eats. Takes 20 minutes to get a new elastic on. |
6/16. Sam saw a new dentist today, my dentist for the last 15 years, Dr Giannotti. As we left our house, Sam yawned and the elastic broke. I couldn't get the lateral on today. It's hard getting anything on the hook, without scratching the gum.
Dr Giannotti, thought that there isn't enough room for #27 to emerge. When I asked Dr Chen #2 before, he said it would have no problem, if there wasn't room it would emerge on the outside of the arch. Actually, I think it is rotated, so it will probably come up and need a 90 degree rotation. Dr Gianotti noted that Sam's canines on the right side have a blunted end, they don't have the shape of a canine. Very curious! She wondered if anyone had filed on it, and if he grinds his teeth, no to both, as far as we know.
Dr Giannotti, thought that there isn't enough room for #27 to emerge. When I asked Dr Chen #2 before, he said it would have no problem, if there wasn't room it would emerge on the outside of the arch. Actually, I think it is rotated, so it will probably come up and need a 90 degree rotation. Dr Gianotti noted that Sam's canines on the right side have a blunted end, they don't have the shape of a canine. Very curious! She wondered if anyone had filed on it, and if he grinds his teeth, no to both, as far as we know.

|
We are using Sam's old 6 mm (1/4"), heavy 4 oz. elastics.
Got dynamometer today. Pulling 1.0 cm = 30 g 1.5 cm = 55 g 2 cm = 88 g 2.5 cm =100 g 3 cm =125 g (that would be a yawn!) According to literature we should be somewhere between 50-100 g. Sam also has old 4 mm (3/16"), superheavy 6 oz. elastics. 1 cm with those is 100 g. Distance between archwires when teeth together is 0.9 mm. |
The elastic broke in the evening. The tissue around the upper hook is getting irritated and the hook embedded so you have to pull it out with tweezers, which irritates the tissue...
Working on the orthodontist issue, but there is a lot of 'don't take mid treatment patients' and two months' waits for an appointment.

|
6/17/2014:
We have to keep going until we have an orthodontist! Meanwhile we can't go off on vacation, Sam can't go off by himself. It's a pretty dismal situation for a 16-year-old who has soldiered on and been through 3 surgeries. For me, as mom, it is completely devastating to end up like this! |

6/20/2014
|
|

IS #6 MOVING???
Ok...I spend a lot of time staring as these images and I might just get lost in the angles, different sizes etc...but...maybe the UCSF curse is broken. Comparing the upper pigtail length in the top images and the latest images, it seems that if the wire was straightened out it would now reach below the archwire, which is would not do in the upper...cautious optimism...We have an orthodontist appointment, but in two weeks, so we'll just keep tugging...
Surgery March 5th
|
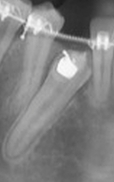
Pano March 6th, 1 day post op
|

7 weeks post op. Bottom of hook is at the line of the top of the neighboring teeth.
|
Pano May 20, 11 weeks post op
|

16 weeks post op. Bottom of hook a couple of mm under the upper tooth line + more medial with oblique elastic added
|
Awaiting local orthodontist help, I've asked Dr Becker some questions, about what we need done:
It is a shame that the twisted ligature in the lower canine has been cut, but you seem to have overcome that by directly threading the eyelet. If that is stable and holds the elastic, it will be fine. The new orthodontist will be able to thread it more securely with 0.012" or 0.014" soft stainless steel ligature wire. However, the use of direct vertical traction is good. The exact traction force is not critical, but continuous 24/7 pull including during meals certainly is. I cannot advise you exactly on which elastic to use, because these can each be used in specific cases and they need to be evaluated for the force level produced - again an orthodontist's input on the spot. He might decide to add a second elastic from the upper canine to the Kobayashi hook that ties the archwire into the lateral incisor. This oblique-directed elastic would add a mesial component to the traction direction, more in line with the long axis of the tooth. It should also be remembered that impacted teeth have a degree of resistance to their eruption from their surrounding tissues and so a stronger pull than for moving teeth along an archwire is usually needed.
If the pigtail is now 5mm long, it is an indication of positive extrusion of the tooth, but is uncomfortable to Sam. It needs to be cut shorter and the end turned over to form a new hook closer to the tissues – opening it a little for ease of access.
We get more room by placing a coil spring on the wire (substituting for the tube space maintainer that I placed) compressed between the brackets on the two adjacent teeth, which must be strong enough to move the teeth, plus an additional indeterminate force to overcome the friction between the main archwire and the bracket slots, to make it free-sliding. In my first letter of referral to the orthodontist, which I presented to you before you left Jerusalem, I wrote of the later need to expand the spaces for both canines. However, there was no point in my attempting this at the time, since it would have markedly complicated the appliance work and would only be relevant after positive improvement in the canines position could be seen.
It is a shame that the twisted ligature in the lower canine has been cut, but you seem to have overcome that by directly threading the eyelet. If that is stable and holds the elastic, it will be fine. The new orthodontist will be able to thread it more securely with 0.012" or 0.014" soft stainless steel ligature wire. However, the use of direct vertical traction is good. The exact traction force is not critical, but continuous 24/7 pull including during meals certainly is. I cannot advise you exactly on which elastic to use, because these can each be used in specific cases and they need to be evaluated for the force level produced - again an orthodontist's input on the spot. He might decide to add a second elastic from the upper canine to the Kobayashi hook that ties the archwire into the lateral incisor. This oblique-directed elastic would add a mesial component to the traction direction, more in line with the long axis of the tooth. It should also be remembered that impacted teeth have a degree of resistance to their eruption from their surrounding tissues and so a stronger pull than for moving teeth along an archwire is usually needed.
If the pigtail is now 5mm long, it is an indication of positive extrusion of the tooth, but is uncomfortable to Sam. It needs to be cut shorter and the end turned over to form a new hook closer to the tissues – opening it a little for ease of access.
We get more room by placing a coil spring on the wire (substituting for the tube space maintainer that I placed) compressed between the brackets on the two adjacent teeth, which must be strong enough to move the teeth, plus an additional indeterminate force to overcome the friction between the main archwire and the bracket slots, to make it free-sliding. In my first letter of referral to the orthodontist, which I presented to you before you left Jerusalem, I wrote of the later need to expand the spaces for both canines. However, there was no point in my attempting this at the time, since it would have markedly complicated the appliance work and would only be relevant after positive improvement in the canines position could be seen.

|
6/29/2014.
I turned up the upper hook slightly to keep the 'vertical displacement' at least 1.5 cm, but it's a bit hard without the right tools. The elastics break a lot, they supposedly expired in May. |
To make long story short: The eyelet broke off and put an end to traction on July 12.
The search for orthodontist went on though, and became a wild goose chase. I tried emails, most didn't answer, one that did, eventually said that he was not experienced enough and cancelled the appointment. Our dentist helped us find one, but he would not commit, he said we first needed images and that appointment was 5 weeks away (because we would get no special favors just because we were desperate to maintain traction), after the images there would be a conference...(according to a 'yelp', the process of getting started could take months). I tried appointments, they would get cancelled, suddenly the doctor was not taking new patients. Turned out some orthodontists don't even deal with metal braces, and thus not impactions at all (the receptionist said the Dr only wanted too handle 'slightly crooked teeth' ).
I dragged Sam to appointments, which were no fun, because he would just be sitting there in the chair, nobody hardly looked at him or his teeth. Consultation ($75). One Dr obviously had his mind set to wish us good luck somewhere else from the outset, but went through the charade of an appointment. He had an assistant sit by the computer, typing the whole conversation. He said, he would have gone through the same trouble if it was his son, but we were too much of a liability. At least we got a free pano out of that visit. Another one got a blanker and blanker expression as I went through Sam's history, then said a couple of 'I feel for you, buddy', to Sam. He made a note of looking up PEIR, said he wanted to be paid before looking through images and full price ortho, since Sam is not a regular transfer. He said we'd be in touch, and was never heard from again.
One Dr did mention that it was 'not standard' to take a patient and not do a cast, nor a cephalogram, as happened at UCSF. Nor did they make any periapicals that showed the root (=periapical area) of the teeth before Dr Becker asked for it before his surgery in March 2014.
Pretty dismal results as far as finding an orthodontist, until Dr Becker gave us the name of a Professor in Portland, who gave us the name of one orthodontist, who gave us the name of another orthodontist...
Conclusion is that orthodontics is composed of different components, and differently minded orthodontists. There is the business side, you need to have a good flow of patients throughout the day; not too many hiccups, not too many inquisitive parents. There is generally no real difference in price for the common cases and the impacted canines, so absolutely no incentive to take on something that has proven itself difficult, that might end with extraction, if you are all business oriented.
Then there is what apparently is another generation of orthodontist, which doesn't calculate quite so singlemindedly in dollars, time and trouble, but, has the instinct to help as a health care provider, and an interest in solving a problem, and in the science of orthodontics. I think it is worthwhile to find out beforehand if an orthodontist Board Certified and belongs to the Angle Society, which seems to be a way to find this latter kind of orthodontist (however, not a total guarantee).
At least, the DIY ortho managed to pull up #27 a bit further before the eyelet broke, see below. Looks like the archwire needs a spring at this point. Unfortunately, #6 seems to still be in the same spot!
The search for orthodontist went on though, and became a wild goose chase. I tried emails, most didn't answer, one that did, eventually said that he was not experienced enough and cancelled the appointment. Our dentist helped us find one, but he would not commit, he said we first needed images and that appointment was 5 weeks away (because we would get no special favors just because we were desperate to maintain traction), after the images there would be a conference...(according to a 'yelp', the process of getting started could take months). I tried appointments, they would get cancelled, suddenly the doctor was not taking new patients. Turned out some orthodontists don't even deal with metal braces, and thus not impactions at all (the receptionist said the Dr only wanted too handle 'slightly crooked teeth' ).
I dragged Sam to appointments, which were no fun, because he would just be sitting there in the chair, nobody hardly looked at him or his teeth. Consultation ($75). One Dr obviously had his mind set to wish us good luck somewhere else from the outset, but went through the charade of an appointment. He had an assistant sit by the computer, typing the whole conversation. He said, he would have gone through the same trouble if it was his son, but we were too much of a liability. At least we got a free pano out of that visit. Another one got a blanker and blanker expression as I went through Sam's history, then said a couple of 'I feel for you, buddy', to Sam. He made a note of looking up PEIR, said he wanted to be paid before looking through images and full price ortho, since Sam is not a regular transfer. He said we'd be in touch, and was never heard from again.
One Dr did mention that it was 'not standard' to take a patient and not do a cast, nor a cephalogram, as happened at UCSF. Nor did they make any periapicals that showed the root (=periapical area) of the teeth before Dr Becker asked for it before his surgery in March 2014.
Pretty dismal results as far as finding an orthodontist, until Dr Becker gave us the name of a Professor in Portland, who gave us the name of one orthodontist, who gave us the name of another orthodontist...
Conclusion is that orthodontics is composed of different components, and differently minded orthodontists. There is the business side, you need to have a good flow of patients throughout the day; not too many hiccups, not too many inquisitive parents. There is generally no real difference in price for the common cases and the impacted canines, so absolutely no incentive to take on something that has proven itself difficult, that might end with extraction, if you are all business oriented.
Then there is what apparently is another generation of orthodontist, which doesn't calculate quite so singlemindedly in dollars, time and trouble, but, has the instinct to help as a health care provider, and an interest in solving a problem, and in the science of orthodontics. I think it is worthwhile to find out beforehand if an orthodontist Board Certified and belongs to the Angle Society, which seems to be a way to find this latter kind of orthodontist (however, not a total guarantee).
At least, the DIY ortho managed to pull up #27 a bit further before the eyelet broke, see below. Looks like the archwire needs a spring at this point. Unfortunately, #6 seems to still be in the same spot!
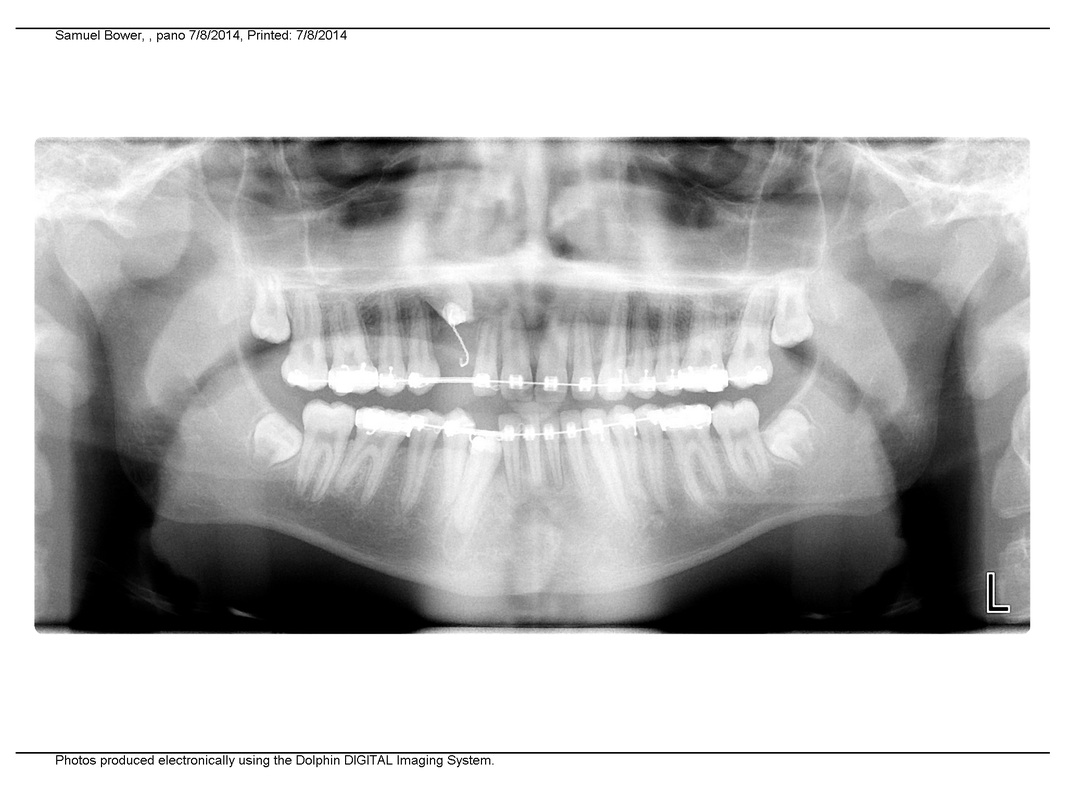
Pano 7/8/14

|
|