TRACTION
Actually, the when and hows of traction seems to depend on a traditional consensus rather than science. Since it is no fun to be in braces, the shorter time, as in the faster you can move teeth into the right place, the better for the patient, and presumably for the orthodontist. Also prolonged time in braces might cause root resorption, periodontal problems and white spots.
The main factor here is the PDL = The periodontal ligament, and biomechanics.
An attempt (they concluded it couldn't be done) at a meta-Analysis in 2003 (7) could not recommend an evidence based force level for optimal efficiency. It was too complicated to calculate the distribution of stress and strains on the PDL, how to account for type of tooth movement, the different phases in the tooth movement,, and lastly they pointed to individual differencies. The article conclude:
After more than half a century of research on orthodontic tooth movement, it is disappointing to conclude
that the answer to the question of the optimal force is still far away.
So, the orthodontist pretty much has to make things up as they go, and you have to hope their instincts are leading them right. But do inquire why they do as they do, and if your gut feeling tells you something else,
your gut might be right.
The main factor here is the PDL = The periodontal ligament, and biomechanics.
An attempt (they concluded it couldn't be done) at a meta-Analysis in 2003 (7) could not recommend an evidence based force level for optimal efficiency. It was too complicated to calculate the distribution of stress and strains on the PDL, how to account for type of tooth movement, the different phases in the tooth movement,, and lastly they pointed to individual differencies. The article conclude:
After more than half a century of research on orthodontic tooth movement, it is disappointing to conclude
that the answer to the question of the optimal force is still far away.
So, the orthodontist pretty much has to make things up as they go, and you have to hope their instincts are leading them right. But do inquire why they do as they do, and if your gut feeling tells you something else,
your gut might be right.
When do you start traction after bonding a bracket on an impacted tooth?
- Immediately
According to Dr Becker, Puricelli
- After 1 to 2 weeks
according to the websites of most American oral surgeon and orthodontist offices
- It is preferable not to apply force on the tooth immediately after surgery, but rather to wait until
tissue healing and flap attachment have occurred; otherwise, the risk of postoperative recession
exists.
...
During the closed surgical technique procedure, the orhtodontist bonds an attachment and can
immediately apply the eruptive force to the tooth, in contrast to the open surgical eruption
technique.(4)
How hard do you need to pull?
There is controversy regarding the amount of load applied to surgical-orthodontic traction. Bishara et al.
suggest a load not exceeding 60 g. Odegaard recommends 75 to 100 g, and Cresccini et al 100g. Forces
should be applied by means of springs, elastics, stainless steel ligatures, or a helical-shaped device attached
to the orthodonttic arch.(3)
The magnitude of orthodontic forces used should be minimal - preferably no more than 60 grams - so tooth
movement is accompanied by migration of the periodontal tissues.(4)
It sound like there is an orthodontic point of view and a periodontal one, because they have different main concerns.
Immediately after surgery, you usually apply a lighter force. Pulling too lightly and nothing happens, pulling to hard, you cause damage. Pulling just right, trying to emulate the natural eruption, you supposedly stimulate the bone formation in the wake of the tooth apex, that is going to hold the tooth for the lifetime of the patient.
- Immediately
According to Dr Becker, Puricelli
- After 1 to 2 weeks
according to the websites of most American oral surgeon and orthodontist offices
- It is preferable not to apply force on the tooth immediately after surgery, but rather to wait until
tissue healing and flap attachment have occurred; otherwise, the risk of postoperative recession
exists.
...
During the closed surgical technique procedure, the orhtodontist bonds an attachment and can
immediately apply the eruptive force to the tooth, in contrast to the open surgical eruption
technique.(4)
How hard do you need to pull?
There is controversy regarding the amount of load applied to surgical-orthodontic traction. Bishara et al.
suggest a load not exceeding 60 g. Odegaard recommends 75 to 100 g, and Cresccini et al 100g. Forces
should be applied by means of springs, elastics, stainless steel ligatures, or a helical-shaped device attached
to the orthodonttic arch.(3)
The magnitude of orthodontic forces used should be minimal - preferably no more than 60 grams - so tooth
movement is accompanied by migration of the periodontal tissues.(4)
It sound like there is an orthodontic point of view and a periodontal one, because they have different main concerns.
Immediately after surgery, you usually apply a lighter force. Pulling too lightly and nothing happens, pulling to hard, you cause damage. Pulling just right, trying to emulate the natural eruption, you supposedly stimulate the bone formation in the wake of the tooth apex, that is going to hold the tooth for the lifetime of the patient.

|
Measuring the force. Image from (5):
(The tooth has been pierced and a wire threaded through.) The amount of force is measured from the end of the TMA wire to the surgically accessed canine ligature. The use of a tension gauge to measure the force with enough sensitivity to detect low intensity forces, which according to Grader and Vanarsdall (25) must range between 35 and 60 grams. (TMA= titanium-molybdenum) |
The Nuts and bolts - or in this case, brackets, hooks and wires - and biomechanics
For the formulas concerning vectors and force, see: http://drhungvu.com/biomechanics
The problem of pulling on those pesky canines is basic mechanics, where is it you want the tooth to go?; is there room to go there? is there anything in the way? ; but also, are you hurting something in the way, like the roots of adjacent teeth (root resorption), are you killing the pulp, are you destroying soft tissue, it's the 'bio' side.
The bio side of things is constantly active. There are cells building and deconstruction, shaping and forming all the time.
The problem of pulling on those pesky canines is basic mechanics, where is it you want the tooth to go?; is there room to go there? is there anything in the way? ; but also, are you hurting something in the way, like the roots of adjacent teeth (root resorption), are you killing the pulp, are you destroying soft tissue, it's the 'bio' side.
The bio side of things is constantly active. There are cells building and deconstruction, shaping and forming all the time.
|
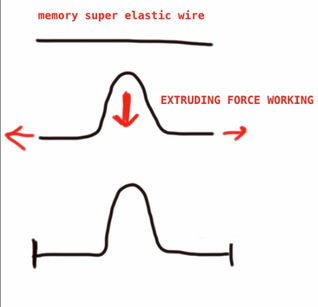
Wire
This is my rendering of the use of superelastic nickel titanium wire --> used in orthodontics. It has 'memory' and will strive to get back to its original shape. This is used to create a force to move teeth. If the wire is attached to the tooth you want to pull down, and the ends of the wire are free to pull outward, you will be using the force of the wire to extrude the tooth. (using Dr Becker's words: The most important attribute of the wire -nickel-titanium- is that it must run freely in the other bracets, otherwise the vertical displacement will jam in the the brackets and not to provide any vertical force). If the ends of the wire are fixed by ligatures as they go through the brackets, you get friction that might reduce or eliminate the extruding force. You have a static wire that is inactive. |
|
|
Kobayashi hooks
|
|

|
Elastic Power chains
Have to be changed often, like the elastic ligatures, because the plastic ages. They can look like: 000000 or 0-0-0-0- or 0--0--0--0 |

Sam's power chains at work
|
|
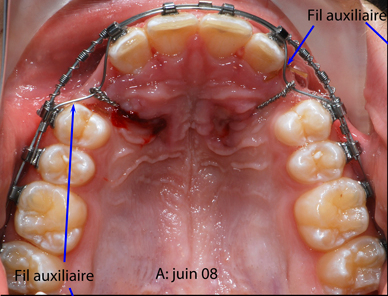
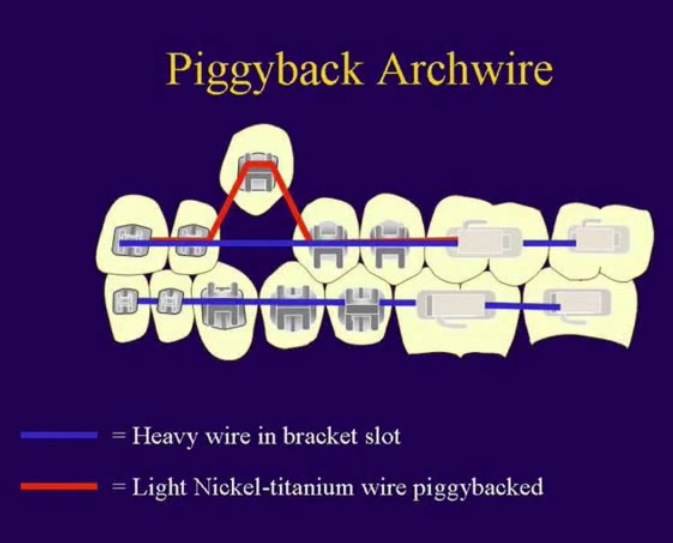
'piggybacking'
It has the main arch wire, that is the stiff part. Then there is a superelastic NiTi (nickel titanium)wire, also called piggyback arch wire The NiTi wire goes through a auxilliary slot in the bracket It works by trying to get back to its original stretched out state, thereby pulling on the impacted tooth. To get the pull effect though, the ends of the elastic wire have to be able to run freely, as Dr. Becker writes |
|
|

|

|
Another illustration of the same idea.
sylvainchamberland.com is an excellent website (in both French and English!) with great photos and illustrations on impacted canines. Do check it out! It does look like the auxiliary wires only extend a short distance from the bend. |
|
Dr Chamberland talks on his website of different ways to pull on the canine:
- traction with fixed appliance and auxilary wire
Like Dr Becker he seems to favor the eyelet and pigtail wire, while the US orthodontist seem to go for the bracket and gold chain at 'expose & bond'.
- traction with removable appliance followed by fixed appliance
- traction with fixed appliance and cantilever arch (wikipedia has information on 'cantilever mechanics (orthdontics).
- traction with fixed appliance and auxilary wire
Like Dr Becker he seems to favor the eyelet and pigtail wire, while the US orthodontist seem to go for the bracket and gold chain at 'expose & bond'.
- traction with removable appliance followed by fixed appliance
- traction with fixed appliance and cantilever arch (wikipedia has information on 'cantilever mechanics (orthdontics).
|
Here's a youtube video about
canines and how to bring them into the arch. The illustrations are teeth that are erupted with brackets (I don't see that it would be different having a chain from a bonded canine.) |
|
|
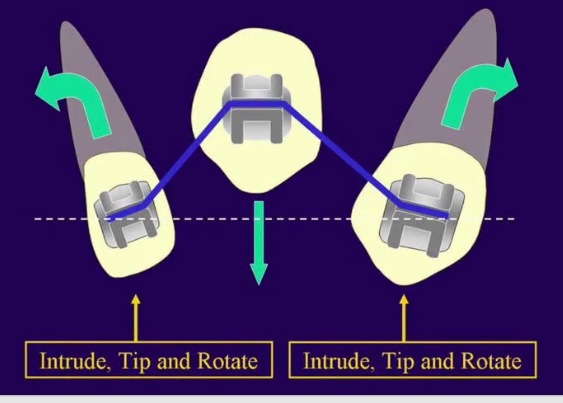
This would be the wrong way to do it according to video:
Using the same NiTi arch wire, the canine is going to be stronger than the teeth next to it and cause 'intrusion, tipping and rotation'. |
|

|
|


|
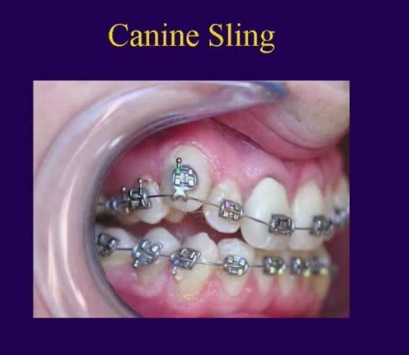
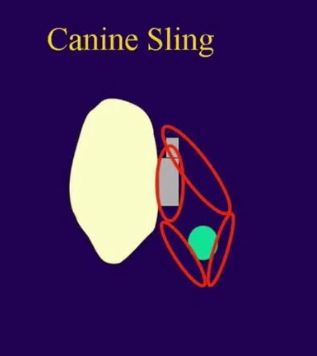
For pulling teeth ithat are close to their destinationn place the video suggests 'the canine sling' : just an elastic power chain going round the NiTi arch wire. This is supposedly not affecting the adjacent teeth.
I'm not sure about how the power and 'vertical displacement' (see Becker comment below for an illustration of the concepton) works in this case. |
|
|
Here's a youtube video by Dr. Abdul Mujeeb showing in time lapse how some palatally impacted canines get in their proper places.
|
|
|
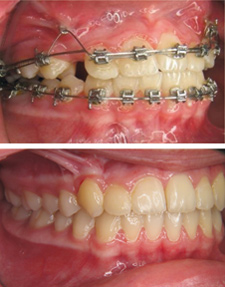
INTER-MAXILLARY VERTICAL ELASTICS
As I understand it, the vertical elastics are used to prevent an 'open bite' from occurring while you are pulling on the canine, or else it might be the canine pulling on the anchor teeth instead. This is how Dr Becker puts it in regards to Sam: Applying traction to these canines has already caused loss of anchorage as witnessed by the lateral open bite on the right side. Accordingly, vertical "up-and-down" elastics are indicated to buttress the anchorage on the right side of the mouth. However, I have not made provisions for this at the moment, in order not to over-complicate things. |

These are intermaxillary elastics going in between upper and lower jaw. (Sam in Feb 2013).
|
In the words of Dr Stella Chu in an article on skeletal anchorage (in this case talking of a palatally impacted canine):
A factor that significantly influences the duration of treatment but is frequently ignored relates to the
additional period needed to to correct deleterious effects created by canine eruption on the adjacent teeth, ie,
loss of anchorage. The eruption of an impacted canine is very taxing on dental anchorage and may cause
deterioration in the positions of the anchor teeth. Thus, in a fully banded case, the reactive forces incurred in
erupting a palatally located canine cause intrusion and flaring of the anterior teeth. The labially directed
traction of the canine towards its place in the dental arch creates lingually directed forces on the adjacent
teeth and may generate a buccal crossbite on the opposite side of the arch, expressed as assymetric skewing
of the dental arch. The anchor teeth must then be realigned, thus increasing the treatment time. Accordingly,
before the attention of the clinician is directed toward the resolution of the impacted tooth, a composite
anchor unit must be created, involving all the available erupted teeth in the same jaw and, often in the
opposite jaw also. This is usually done by the use of as large a base arch as will fill the the slots of the
brackets on all the other teeth, with or without the use of intermaxillary elastics.(1)
A factor that significantly influences the duration of treatment but is frequently ignored relates to the
additional period needed to to correct deleterious effects created by canine eruption on the adjacent teeth, ie,
loss of anchorage. The eruption of an impacted canine is very taxing on dental anchorage and may cause
deterioration in the positions of the anchor teeth. Thus, in a fully banded case, the reactive forces incurred in
erupting a palatally located canine cause intrusion and flaring of the anterior teeth. The labially directed
traction of the canine towards its place in the dental arch creates lingually directed forces on the adjacent
teeth and may generate a buccal crossbite on the opposite side of the arch, expressed as assymetric skewing
of the dental arch. The anchor teeth must then be realigned, thus increasing the treatment time. Accordingly,
before the attention of the clinician is directed toward the resolution of the impacted tooth, a composite
anchor unit must be created, involving all the available erupted teeth in the same jaw and, often in the
opposite jaw also. This is usually done by the use of as large a base arch as will fill the the slots of the
brackets on all the other teeth, with or without the use of intermaxillary elastics.(1)
|
Forces at work
Every force has an equal reactive force! (Newton's third law) Canines are big with long roots and the force pulling on the tooth, if not reckonned with, is going to wreck havoc on the other teeth and the bite as a whole.. Picture (a) and (b) demonstrates this. It's a lateral open bite due to loss of anchorage. This is corrected in (c) by the means of a vertical inter-maxillary bite-closing elastic (blue) and a TAD (temporary anchoring device) in the form of a titanium screw |
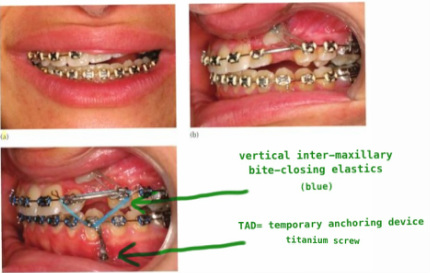
images borrowed from Dr Becker's excellent work:
"Orthodontic Treatment of Impacted Teeth" (my writing in green) |
The bio part of biodynamics
To extrude an impacted canine, is not just the mechanics of forcibly pulling on an object to move it to a location, making room for it and avoiding obstacles as you pull. As the tooth is moving, the movement stimulates cells in the periodontal ligament to cause bone remodeling, removing bone in the direction of travel of the tooth and adding it to the space created. (2)
To extrude an impacted canine, is not just the mechanics of forcibly pulling on an object to move it to a location, making room for it and avoiding obstacles as you pull. As the tooth is moving, the movement stimulates cells in the periodontal ligament to cause bone remodeling, removing bone in the direction of travel of the tooth and adding it to the space created. (2)
TAD = Temporary Anchoring Device
also called mini-screws, mini-implants, micro-implants
Approved by the FDA in 2005. Before that used in Germany and Asia for a decade.
The TAD is commonly a titanium screw that is put into, what is ultimately more stable than the neighboring teeth, the skeleton, as in jaw bone.
There are biomechanical techniques that are useful in some cases, but have to be mastered, such as skeletal anchorage (3). Instead of using anchor teeth that are used as attachments for pulling on the canine, a fixed implant is put into bone. That way you don't risk negative consequences on the neighboring teeth and the arch
when pulling on the canines. The principle is Newton's third law: For every action there is an equal and opposite
re-action. Pulling on a canine, might instead pull on the anchor teeth.
(skeletal anchorage instead of dental) are invaluable in assessing the prognosis of canine movement
before appliance placement. They allow the orthodontist to plan treatment that may have been previously
unpredictable or even impossible with tradtional mechanics...
...less reactive forces are applied to the adjacent teeth, and the danger of negative deleterious side
effects, such as root resorption or uncontrolled movement of anchor teeth is significantly decreased.
Treatment of the impaction may be performed separately before or even simultaneously with treatment
of the remainder of the dentition, as 2 distinct force systems.(pp 239-40)(3)
http://www.tomasforum.com/files/CRG_Sept-2011.pdf
Website above is, I guess, basically an ad, but describes all kinds of diagnosis when a TAD is useful, including for
impacted canines.
also called mini-screws, mini-implants, micro-implants
Approved by the FDA in 2005. Before that used in Germany and Asia for a decade.
The TAD is commonly a titanium screw that is put into, what is ultimately more stable than the neighboring teeth, the skeleton, as in jaw bone.
There are biomechanical techniques that are useful in some cases, but have to be mastered, such as skeletal anchorage (3). Instead of using anchor teeth that are used as attachments for pulling on the canine, a fixed implant is put into bone. That way you don't risk negative consequences on the neighboring teeth and the arch
when pulling on the canines. The principle is Newton's third law: For every action there is an equal and opposite
re-action. Pulling on a canine, might instead pull on the anchor teeth.
(skeletal anchorage instead of dental) are invaluable in assessing the prognosis of canine movement
before appliance placement. They allow the orthodontist to plan treatment that may have been previously
unpredictable or even impossible with tradtional mechanics...
...less reactive forces are applied to the adjacent teeth, and the danger of negative deleterious side
effects, such as root resorption or uncontrolled movement of anchor teeth is significantly decreased.
Treatment of the impaction may be performed separately before or even simultaneously with treatment
of the remainder of the dentition, as 2 distinct force systems.(pp 239-40)(3)
http://www.tomasforum.com/files/CRG_Sept-2011.pdf
Website above is, I guess, basically an ad, but describes all kinds of diagnosis when a TAD is useful, including for
impacted canines.
Cantilevers
A cantilever is a 'beam anchored only at one end'(wikipedia), or a longer piece of wire sticking out,
in biomechanics.
A cantilever is a 'beam anchored only at one end'(wikipedia), or a longer piece of wire sticking out,
in biomechanics.
Keeping the tension constant
The 24/7 aspect of tension is that you don't want stop and go action (though, I haven't seen a study on that yet, it is more based on a 'that sounds right' kind of logic); this is unrelenting, constant force we are talking about. So it comes down to: how long does a rubber band last? You would hope that the people in the business has figuered it out, but why is it 2 weeks between visits with one orthodontist, and 5 or 6 weeks with another? Until proven otherwise, my presumption is that each orthodontist makes it up according to experience, or lack therof, what they have learnt somewhere, but it is pretty much up to whatever their own ideas are.
The 24/7 aspect of tension is that you don't want stop and go action (though, I haven't seen a study on that yet, it is more based on a 'that sounds right' kind of logic); this is unrelenting, constant force we are talking about. So it comes down to: how long does a rubber band last? You would hope that the people in the business has figuered it out, but why is it 2 weeks between visits with one orthodontist, and 5 or 6 weeks with another? Until proven otherwise, my presumption is that each orthodontist makes it up according to experience, or lack therof, what they have learnt somewhere, but it is pretty much up to whatever their own ideas are.
The case for immediate traction
The immediate traction described above isn't practiced generally as far as I can tell, a natural consequence of the orthodontist not being present at surgery. On individual orthodontist websites with 'stock' info on impacted canines. as well as in textbook version's, expose & bond surgery is followed by 1-2 weeks of 'rest' **, before the orthodontist applies traction:
Orthodontic manipulation is initiated after the initial healing of the soft tissue and when the patient is
comfortable, which can usually be expected 7-14 days after surgery.(6)
It would be interesting to know what studies this sequence of treatment emanates from, and if it is faulty, how long it will take to get rid of.
Here is the abstract of another interesting study: Ankylosis of impacted canines: a retrospective post-surgical study' by A. Garcia, 2013 (7):
Ankylosis is generally discovered following resistance to orthodontic displacement of an impacted canine.
This retrospective study, drawing on direct perioperative observation of impacted teeth and of their sites, is
intended, among other things, to analyze the causes of resistance to orthodontic movement and to report on
the therapeutic interest of the surgical tooth displacement technique in this type of clinical situation. We
demonstrate that primary coronal ankylosis can be detected by the orthodontic practioner using radiographic
records, that cervical ankylosis consequent to operative trauma during release is necessarily unpredictable
and that it should be suspected when the tooth resists traction for more that 3 months in the absence of any
other obvious case of resistance. Hence, the risk of ankylosis linked to the level of surgical difficulty increases
with the depth of coronal submergence within the bone. Moreover, the immediate placement of traction
following release reduces the risk of ankylosis. In addition, temporarily suspending traction is a risk for
secondary apical ankylosis. Finally surgical positioning should be borne in mind as the final effective option
when faced with any form of dental retention.
(1) Chaushu S, Chaushu G. Skeletal Implant Anchorage in the Treatment of Impacted Teeth - A Review of the
State of the Art. Seminars in Orthodontics, Vol 16, No 3 (September), 2010: pp 234-241.
(2) From the Wikipedia on 'Dental Implants'. Surprisingly there is nothing under 'Impacted Canines', by the way!
(3) PEREIRA, Cassiano Costa Silva et al. Surgical-Orthodontic Traction for Impacted Maxillary Canines: A Critical
view and Suggested Protocol. Stomatos [online]. 2012, vol.18, n.34 [cited 2014-06-15], pp. 78-83 .
Available from: <http://revodonto.bvsalud.org/scielo.php?script=sci_arttext&pid=S1519-
44422012000200009&lng=en&nrm=iso>. ISSN 1519-4442.
(4) Nilesh
(5) Filho L, Consolaro A, Almeida Cardoso, Siqueira D. Enamel drilling for canine traction: advantages,
disadvantages, description of surgical technique and biomechanics.Dental Press Journalk of Orthodontics. vol
16 no 5 Maringá Sept./Oct. 2011.
(6) Paduano et al. Use of Cantilever Mechanics for Impacted Teeth: Case Series. The Open Dentistry Journal,
2013, 7, 186-197.
(7) Ren Y, Maltha JC, Kuijpers-Jagtman AM. Optimum force magnitude for orthodontic tooth movement: a
systematic literature review. Angle Orthod 2003;73:86-92