The case for Cone Beam Computer Tomography (CBCT)
New Emerging Techniques..beware
Historically excitement vs skepticism of a new emerging technique should make any consumer/patient wary. When I was born in 1958 the Jubileumskliniken in Göteborg, Sweden, was just in a very giddy enthusiastic mood about radiation therapy. As an infant I had a small hemangioma** on my sternum. The pediatrician warned that this would/could develop into cancer and at 9 months old, a piece of cesium was put on the hemangioma my chest for an hour. It would cause a bit of a indentation in my sternum. Other children had the cesium put in locations where it would do more harm, as over the thyroid, on a breast, or near the eye. I've heard that in the States radiation was a novelty gimmick used in shoe stores for measuring feet.
Point being that any new technique, especially if it is connected to risk, should be used for the right reason in the first place, evaluated, and only used by someone who is sufficiently competent.
On the other hand...if there is a technique that will elucidate a problem, lead to a better result, in a shorter time, then you want it available as soon as possible.
So enter CBCT - computer cone beam tomography, digital so the radiation is lower than traditional scans, expensive, and it's usefulness very dependent on the competence of who is supposed to interpret and use the information.
Twenty years later. CBCT technology keeps improving, radiation doses going down, some orthodontists get their own machines, and no doubt using it very liberally to cover their costs; while some don't bother learning how to use it, probably calculating that they are retiring before CBCT is a standard.
Historically excitement vs skepticism of a new emerging technique should make any consumer/patient wary. When I was born in 1958 the Jubileumskliniken in Göteborg, Sweden, was just in a very giddy enthusiastic mood about radiation therapy. As an infant I had a small hemangioma** on my sternum. The pediatrician warned that this would/could develop into cancer and at 9 months old, a piece of cesium was put on the hemangioma my chest for an hour. It would cause a bit of a indentation in my sternum. Other children had the cesium put in locations where it would do more harm, as over the thyroid, on a breast, or near the eye. I've heard that in the States radiation was a novelty gimmick used in shoe stores for measuring feet.
Point being that any new technique, especially if it is connected to risk, should be used for the right reason in the first place, evaluated, and only used by someone who is sufficiently competent.
On the other hand...if there is a technique that will elucidate a problem, lead to a better result, in a shorter time, then you want it available as soon as possible.
So enter CBCT - computer cone beam tomography, digital so the radiation is lower than traditional scans, expensive, and it's usefulness very dependent on the competence of who is supposed to interpret and use the information.
Twenty years later. CBCT technology keeps improving, radiation doses going down, some orthodontists get their own machines, and no doubt using it very liberally to cover their costs; while some don't bother learning how to use it, probably calculating that they are retiring before CBCT is a standard.
|
|
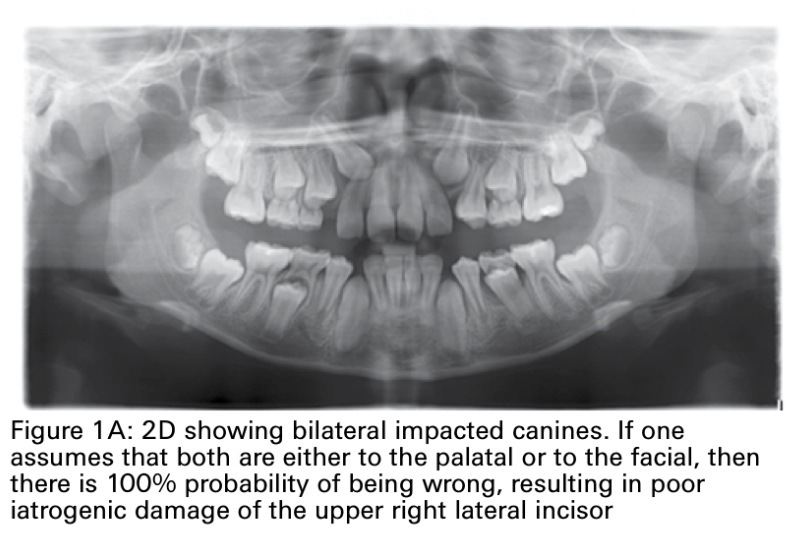
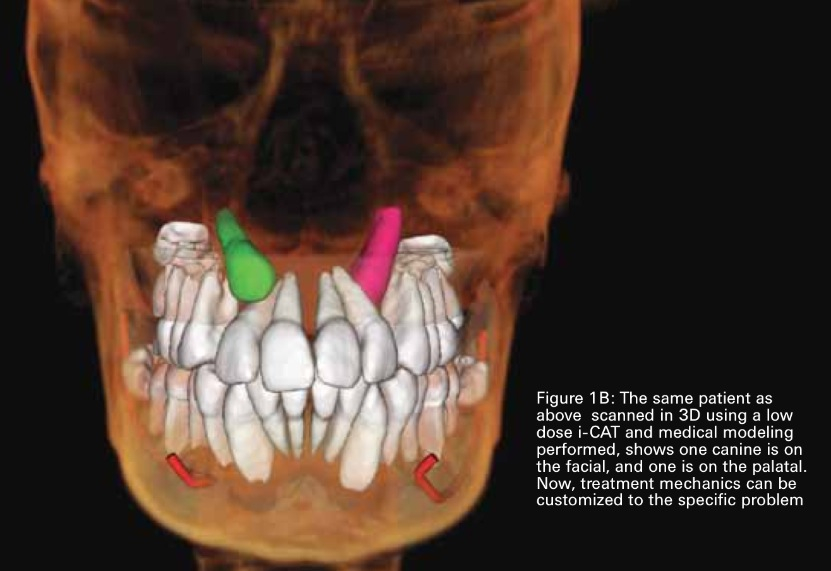
Images above are from quinteroorthodontics.com and Drs Quintero and Sean Carlson's article 'CBCT changing the face of orthodontics', images are actually from a case of Dr Quintaro's in (8).
I think the images make a convincing case, but it is interesting to see how a new technique enters the scene, is
rejected or embraced, and how long it will take for it to benefit patients. With low dose CBCTs, I don't see how you defend doing surgery on impacted canines without CBCT. A part from the surgery, the CBCT can then be used to analyse how proper traction should be applied by the orthodontist.
I think the images make a convincing case, but it is interesting to see how a new technique enters the scene, is
rejected or embraced, and how long it will take for it to benefit patients. With low dose CBCTs, I don't see how you defend doing surgery on impacted canines without CBCT. A part from the surgery, the CBCT can then be used to analyse how proper traction should be applied by the orthodontist.
To do, or not to do CBCT, is not going to even be a question in 5 years time (my qualified-non-professional-parent opinion). Orthodontists, and dentists, are getting their own machines, and once they have them, they are going to use them, and the orthodontist who doesn't, will look obsolete. I think it is going the same way as digital imagery vs. traditional x-rays 10 years ago. To continue predicting what is ahead I can only hope that 'impacted canines' becomes its own speciality, that it is identified as the 'bête noir' it is, and that not just anybody should 'have a go' at it. Radiation dosage isn't the issue anymore if technology is handled right, it's competence and access.( Also predicting, I think you will be using 3D printers making models and that direction and force of traction will be scientifically administered, actually I think we are already there.).
For a CBCT, a scanner rotates round the patient's head while obtaining hundreds of images, 'slices',
dcm files (part of DICOM), of the area of interest. The xrays are concentrated to the specific area in a 'cone'. These images can then be manipulated through software programs in 3D. Certainly to manipulate and interpret the images is then going to take time and require experience and skill.
It is very easy to share the images for consultations and between treating professionals through
DICOM (Digital Imaging and Communication i Medicine), so this is how you can come by expert advice from anywhere in the world by the clic of a computer.
For a CBCT, a scanner rotates round the patient's head while obtaining hundreds of images, 'slices',
dcm files (part of DICOM), of the area of interest. The xrays are concentrated to the specific area in a 'cone'. These images can then be manipulated through software programs in 3D. Certainly to manipulate and interpret the images is then going to take time and require experience and skill.
It is very easy to share the images for consultations and between treating professionals through
DICOM (Digital Imaging and Communication i Medicine), so this is how you can come by expert advice from anywhere in the world by the clic of a computer.

|
|
Here is Dr. Sean Carlson's youtube video on CBCT
from February, 2014 He has a practice in Mill Valley, CA and puts informative podcasts on his website: www.carlsonorthodontics.com Dr. Carlson shows cases where not doing an initial CBCT will result in harm. Dr Carlson refers to a paper by Dr. John Ludlow, North Carolina, from December 2013, where he makes the case for CBCT as a way to lower the radiation patients as compared to 2D imaging. |
Dr. Carlson gives a 1959 quote originally by Dr. Steiner addressing the Angle Society. In 1959 it applied to cephalometrics, Dr. Carlson points out that it might as well apply to CBCT today.
To those of you who are not fully employing cephalometric principals in your orthodontic practices, I ask these questions:
Do you really want to know what you are doing to your patients, or are you afraid to find out?
Do you suspect that, if you did know, you might sometimes be unhappy?
If you did not like what you found, would you do something about it?
If the answer to these questions is no, then you do not need a cephalometer.
Do you really want to know what you are doing to your patients, or are you afraid to find out?
Do you suspect that, if you did know, you might sometimes be unhappy?
If you did not like what you found, would you do something about it?
If the answer to these questions is no, then you do not need a cephalometer.
The evolving orthodontic attitude to CBCT as illustrated by articles in the 'Bulletin' for the Pacific Coast Society of Orthodontists (pscortho.org):
2008 Spring Bulletin:"Three-Dimensional Cephalometrics in Clinical Practise: CBCT for You and Me" by Dr. John C. Huang:
For orthodontics, one single CBCT scan can effectively generate, at a relatively quivalent radiation,
all the conventional radiographic images needed for orthodontic diagnosis such as lateral
cephalogram, panoramic radiogaph, antero-posterior cephalogram, tempero-mandibular joint
tomograms, as well as many other oblique/ cross-sectional slices previously unavailable in flat
planar films.
2008 Winter Bulletin: depicts how the CBCT got established and developed at UCLA in 2003:
...we began taking CBCT scans on most of our patients in August 2006. From a single CBCT scan we are able
to generate a panoramic, lateral and front headfilms, tomographs, and submentovertex views, thus
eliminating the need for additional radiographs in the majority of patients (p 37)
2009 Spring Bulletin:
Dr. Hatcher notes that cone beam devices are now being offered by over 30 companies. He also
rightly points out that medico-legally, not using a CBCT in more complicated cases, such as
complicated impactions, would be defenseless.(p 9)
2010 Winter Bulletin: "3-D imaging - Do we Really Need It", talks of the first CBCT machine in the US installed at the Loma Linda University in June 2001 and being very enthusiastic about the possibilites that 3D imaging opens up.
2010 Summer Bulletin: Dr. Gerald Nelson writes in the editorial:
We are in a murky sea right now, and I look forward to the day when fresh currents sweep it all
away. So many questions are on the table about the use of CBCT in orthodontic practice.
Do we owe it to patients to use CBCT for all patients, since the information is more accurate, and significantly
more information is available?
I am part of an orthodontic program where each patient receives several CBCT scans during his or
her comprehensive orthodontic treatment. We are conducting some relevant research, and I know
that these records improve our diagnoses. However, how much are we benefitting our body of
If we order a CBCT, do we also need to order an Oral and Maxillofacial Radiologist's report? Should we offer the patient an option to not order this report?
2011 Spring editorial by Dr. Gerald Nelson:
A study done at UCSF by Dr. Erik Haney (Fairfax, CA) in 2009 involved orthodontists and oral surgeons
reviewing stations with 2D and 3D images of canine impactions. Twenty-five impacted teeth had had both
types of x-rays, which were distributed around randomly. Of the treatment plans for extraction of the
impacted tooth using the 2D images, 53% were changed to recovery when viewed in 3D. The recommended
vector of force application also differed between the two image techniques. Since then, other studies have
confirmed the value of 3D scans for impacted teeth.
Liability. Risk is an issue. A primary risk is that you will miss something important in you diagnosis with 2D.
When a disgrunteled patient goes to an attorney to take action against an orthodontist, the typical first action
is to order a CBCT scan to see if any pathology was missed. The second risk is less than ideal treatment plan,
since we know that treatment plans change with the benefit of 3D images. The third liability is the
responsibility to detect pathology in the entire 3D volume (not to diagnose every aberration, but to notice
and refer when appropriate). We handle this at UCSF by ordering radiologist reports. These reports are very
instructive, and after reviewing a few dozen of them, one becomes quite comfortable evaluating the image
on one's own.(p 12)
Orthodontists must recognize that this technology offers important benefits to the patient, and we need to
move toward utilizing CBCT on all our patients - and developing our diagnostic skills appropriately. The
technology offers an excellent tool to improve our treatment plans and avoid missing important pathology in
our patients.
The above editorial also refers to a 2010 article in American Journal of Orthodontics, 'Four curious cases of CBCT'. Abstract:
2008 Spring Bulletin:"Three-Dimensional Cephalometrics in Clinical Practise: CBCT for You and Me" by Dr. John C. Huang:
For orthodontics, one single CBCT scan can effectively generate, at a relatively quivalent radiation,
all the conventional radiographic images needed for orthodontic diagnosis such as lateral
cephalogram, panoramic radiogaph, antero-posterior cephalogram, tempero-mandibular joint
tomograms, as well as many other oblique/ cross-sectional slices previously unavailable in flat
planar films.
2008 Winter Bulletin: depicts how the CBCT got established and developed at UCLA in 2003:
...we began taking CBCT scans on most of our patients in August 2006. From a single CBCT scan we are able
to generate a panoramic, lateral and front headfilms, tomographs, and submentovertex views, thus
eliminating the need for additional radiographs in the majority of patients (p 37)
2009 Spring Bulletin:
Dr. Hatcher notes that cone beam devices are now being offered by over 30 companies. He also
rightly points out that medico-legally, not using a CBCT in more complicated cases, such as
complicated impactions, would be defenseless.(p 9)
2010 Winter Bulletin: "3-D imaging - Do we Really Need It", talks of the first CBCT machine in the US installed at the Loma Linda University in June 2001 and being very enthusiastic about the possibilites that 3D imaging opens up.
2010 Summer Bulletin: Dr. Gerald Nelson writes in the editorial:
We are in a murky sea right now, and I look forward to the day when fresh currents sweep it all
away. So many questions are on the table about the use of CBCT in orthodontic practice.
Do we owe it to patients to use CBCT for all patients, since the information is more accurate, and significantly
more information is available?
I am part of an orthodontic program where each patient receives several CBCT scans during his or
her comprehensive orthodontic treatment. We are conducting some relevant research, and I know
that these records improve our diagnoses. However, how much are we benefitting our body of
If we order a CBCT, do we also need to order an Oral and Maxillofacial Radiologist's report? Should we offer the patient an option to not order this report?
2011 Spring editorial by Dr. Gerald Nelson:
A study done at UCSF by Dr. Erik Haney (Fairfax, CA) in 2009 involved orthodontists and oral surgeons
reviewing stations with 2D and 3D images of canine impactions. Twenty-five impacted teeth had had both
types of x-rays, which were distributed around randomly. Of the treatment plans for extraction of the
impacted tooth using the 2D images, 53% were changed to recovery when viewed in 3D. The recommended
vector of force application also differed between the two image techniques. Since then, other studies have
confirmed the value of 3D scans for impacted teeth.
Liability. Risk is an issue. A primary risk is that you will miss something important in you diagnosis with 2D.
When a disgrunteled patient goes to an attorney to take action against an orthodontist, the typical first action
is to order a CBCT scan to see if any pathology was missed. The second risk is less than ideal treatment plan,
since we know that treatment plans change with the benefit of 3D images. The third liability is the
responsibility to detect pathology in the entire 3D volume (not to diagnose every aberration, but to notice
and refer when appropriate). We handle this at UCSF by ordering radiologist reports. These reports are very
instructive, and after reviewing a few dozen of them, one becomes quite comfortable evaluating the image
on one's own.(p 12)
Orthodontists must recognize that this technology offers important benefits to the patient, and we need to
move toward utilizing CBCT on all our patients - and developing our diagnostic skills appropriately. The
technology offers an excellent tool to improve our treatment plans and avoid missing important pathology in
our patients.
The above editorial also refers to a 2010 article in American Journal of Orthodontics, 'Four curious cases of CBCT'. Abstract:
Cone-beam computed tomography (CBCT) has become popular, and its many inherent advantages are indisputable. Nevertheless, CBCT is prescribed cautiously because the radiation dosage is higher than that of conventional radiography. When and to what extent should CBCT be prescribed for orthodontic patients? The purpose of this article is to present 4 curious cases in which a considerable discrepancy was found between the conventional panoramic radiograph and the CBCT view. Is it time to spare patients an unnecessary conventional panoramic radiograph and shift to CBCT for all patients?
The four curious cases at the Cairo University Egypt, was a 14-year-old girl where the CBCT revealed a foreign body, a pen eraser, in the nose; a 32-year-old woman where a left root was impeding the straightening of a molar; a patient with a dislodged TAD (temporary anchorage device); and a patient with a fracture in the mandible. All cases where the CBCT was superior to the panoramic radiograph.
2011 Summer Bulletin: has an interview with Dr. James Mah who is researching virtual 3D craniofacial patients upon which diagnosis, treatment planning and simulation can be performed. (p 19)
2013 Spring Bulletin: has the article 3-D-Aided Treatment of Impacted and Transposed teeth' with a summary of a talk by Dr. Kapila:
CBCT is not currently accepted by most clinicians for routine orthodontic records usage. The
prevailing emphasis on evidence-based therapy in orthodontics leads one to question what is the
best evidence-based use for CBCT today. In what situations will the information gathered from a
CBCT scan likely alter the diagnosis and/or treatment plan in a significant number of cases?
According to Dr. Kapila, the only situation that currently qualifies under this strict definition is the
impacted maxillary canine. However, a continuous flow of research is clarifying the protocols. Dr.
Kapila expects that unerupted teeth, missing teeth, assymetries, and anterior open bite will also
be identified as cases that will benefit from CBCT. (p29)
Dr. Kapila is the author of 'The current status of CBCT imaging in orthodontics' from 2011 (13), where he talks of CBCT in relation to impacted canines:
Of the topics discussed, impacted canines is the one in which CBCT has been shown to improve diagnosis and
possibly contribute to modifications in treatment planning. CBCT has been shown to enhance the ability to
accurately localize the canine, evaluate its proximity to other teeth, examine the follicle size and assess
resorption of the adjacent teeth.(34) A recent study compared variations in the diagnostic information
derived from routine 2D radiographs that included panoramic, occlusal and two periapical views with 3D CBCT
images and subsequent effects of this information on the treatment decisions by orthodontists.(35) The
orthodontists had substantially different perception of localization and root damage, and a significantly higher
confidence in diagnosis and treatment planning with CBCT images than with routine radiographs. More
importantly, the original treatment plans derived from the 2D radiographs were modified for more than a
quarter of the teeth when the orthodontists viewed the CBCT images. This study clearly demonstrates the
use of CBCT in both refining diagnosis and modifications in treatment plans of a significant number of
impacted teeth, thus validating the use of this imaging modality for impacted teeth.
You have a new technology that is proving itself vastly superior to the conventional. You have the
spearhead of enthusiastic practitioners, then you have a lagging, unwieldy mass resisting, because of the need for investing in equipment and training, and maybe also the basic fear that everyone doesn't have the fundamental spatial skill to be able to put all the new technology to its fullest use. It's a paradigm shift, "murky waters'" indeed.
However, there is a tipping point in the evolution and advancement of medicine, where not treating according to the best current knowledge is unethical, where not raising the bar is immoral, where you have to reevaluate 'standard of care'. As stated above, it was 'defenseless' in 2009 to not use CBCT for complicated cases of impacted canines, in 2010 the article ventures to ask if it's time to leave the Panorex for the CBCT, and 2013 it is stated that CBCT should be used for impacted canines.
Today, when the µSv dosage of radiation for a Panorex is equivalent to an ALARA CBCT, I can't find
any defense for not to make a change in 'standard of care'. It is very regretful that the AAO resisted putting out new guidelines 2012.
2013 Spring Bulletin: has the article 3-D-Aided Treatment of Impacted and Transposed teeth' with a summary of a talk by Dr. Kapila:
CBCT is not currently accepted by most clinicians for routine orthodontic records usage. The
prevailing emphasis on evidence-based therapy in orthodontics leads one to question what is the
best evidence-based use for CBCT today. In what situations will the information gathered from a
CBCT scan likely alter the diagnosis and/or treatment plan in a significant number of cases?
According to Dr. Kapila, the only situation that currently qualifies under this strict definition is the
impacted maxillary canine. However, a continuous flow of research is clarifying the protocols. Dr.
Kapila expects that unerupted teeth, missing teeth, assymetries, and anterior open bite will also
be identified as cases that will benefit from CBCT. (p29)
Dr. Kapila is the author of 'The current status of CBCT imaging in orthodontics' from 2011 (13), where he talks of CBCT in relation to impacted canines:
Of the topics discussed, impacted canines is the one in which CBCT has been shown to improve diagnosis and
possibly contribute to modifications in treatment planning. CBCT has been shown to enhance the ability to
accurately localize the canine, evaluate its proximity to other teeth, examine the follicle size and assess
resorption of the adjacent teeth.(34) A recent study compared variations in the diagnostic information
derived from routine 2D radiographs that included panoramic, occlusal and two periapical views with 3D CBCT
images and subsequent effects of this information on the treatment decisions by orthodontists.(35) The
orthodontists had substantially different perception of localization and root damage, and a significantly higher
confidence in diagnosis and treatment planning with CBCT images than with routine radiographs. More
importantly, the original treatment plans derived from the 2D radiographs were modified for more than a
quarter of the teeth when the orthodontists viewed the CBCT images. This study clearly demonstrates the
use of CBCT in both refining diagnosis and modifications in treatment plans of a significant number of
impacted teeth, thus validating the use of this imaging modality for impacted teeth.
You have a new technology that is proving itself vastly superior to the conventional. You have the
spearhead of enthusiastic practitioners, then you have a lagging, unwieldy mass resisting, because of the need for investing in equipment and training, and maybe also the basic fear that everyone doesn't have the fundamental spatial skill to be able to put all the new technology to its fullest use. It's a paradigm shift, "murky waters'" indeed.
However, there is a tipping point in the evolution and advancement of medicine, where not treating according to the best current knowledge is unethical, where not raising the bar is immoral, where you have to reevaluate 'standard of care'. As stated above, it was 'defenseless' in 2009 to not use CBCT for complicated cases of impacted canines, in 2010 the article ventures to ask if it's time to leave the Panorex for the CBCT, and 2013 it is stated that CBCT should be used for impacted canines.
Today, when the µSv dosage of radiation for a Panorex is equivalent to an ALARA CBCT, I can't find
any defense for not to make a change in 'standard of care'. It is very regretful that the AAO resisted putting out new guidelines 2012.
Act blindly or know what you are doing? Duh...
According to Chaushu et al. (1), for an orthodontist to be in a position to recommend the best line of treatment for an impacted tooth, the following information is required:
1) the exact positions of the crown and root apex of the impacted tooth and the three-dimensional orientation
of its long axis,
2) the proximity of the impacted tooth to the roots of adjacent teeth,
3) the presence of any pathological entities in association with the impacted tooth and their spatial relationship
with the impacted tooth,
4) the presence of adverse conditions affecting the adjacent teeth, including root resorption
5) the three-dimensional anatomy of the crown and root of the impacted tooth
Quotes from Dr. Becker et al.'s 'Cone-beam computed tomography and the orthosurgical management of impacted teeth'(10)suppl):
CBCT diagnosis can provide information that lets the practioner view the tooth in the three planes of space
and the tooth's adjacent structures with accuracy, including one-tone measurements of distance. Axial,
transaxial and coronal slices can show the existence and location of supernumerary teeth, odontomes and
soft-tissue pathological entities; the extent and depth of the resorption process of the neighboring roots; the
relationship of the roots of an impacted tooth to important anatomical structurees, such as the inferior
dental canal or maxilliary sinus; the proximity of the tooth to neighboring roots; and the root apex location
and the orientation of the long axis of the canine.
A series of plain film radiographs obtained at diverse angles will show the impacted tooth variously
superimposed on the roots of the adjacent teeth and, if the exact angle of of each image can be defined, it
is possible to arrive at a fair assessement of their 3D relationship. However, radiographs taken at diverse
angles are open to possible misinterpretations, miscalculations and mistakes, take much more time than does
cone beam computed tomography (CBCT) and do not provide the same level of resolution and accuracy as
does CBCT. Nevertheless, some authorities consider plain film radiographs to be adequate in many cases of
impacted canines. (p. 155)(1)
The article goes on to describe, in technical terms, the advantages of the CBCT:
The indications for CBCT in relation to the treatment of impacted teeth are compelling, particularly in
terms of anatomical detail, root resorption and the labiolingual relationship of the impacted tooth with the
roots of neighboring teeth, in addition to determining the pathway for biomechanical resolution. As CBCT is
in the relatively early stages of clinical use, there are no published and evidence-based guidelines regarding
its recommended use in the context of treating impacted teeth. We recommend its use, albeit empirically,
in all but the superficially located impacted canines. (pp.165-166).
Another article (5) in support of CBCT concludes:
The use of CBCT in orthodontics greatly enhances our understanding of impacted canines and offers
unique, comprehensive information for individual situations. Compared with conventional imaging
approaches, the
fidelity of this information is unsurpassed. In addition, this information is invaluable
for prognostication and development of biomechanical approaches for management of the impacted
teeth.
One more quote from Dr. Becker's 'Analysis of Failure in the treatment of impacted teeth' (3):
There are many aspects and minutiae involved in the treatment of impacted maxillary canines, that, singly
or together, can lead to failure of the overall aim of the exercise. This study has shown that failure in this
type of treatment is all to frequent for the following reasons.
1. Diagnosis of the location of the tooth and its immediate relationship with the roots of the adjacent teeth
is generally treated with cavalier and often negligent simplicity, even though modern technology has
provided the tools to achieve this with great accuracy in all 3 dimensions.
2. With inappropriate positional diagnosis, it follows traction will be applied in the wrong direction.
3. A lack of appreciation of the considerable anchorage requirements of the case and the need to exploit all
available means of enhancing them will inevitably lead to inefficient mechanotherapy and unnecessarily
longer treatment.
4. Ankylosis might have afflicted the impacted tooth either a priori or as a result of the earlier surgical
or orthodontic maneuvers.(p 753)(3)
From Dr. Becker's Bulletins:
When dealing with impacted teeth, it is crucial to accurately locate the tooth in the 3 planes of space
and in relation to the adjacent teeth, before any treatment to resolve it should be initiated. The
purpose is to evaluate the topography of the locale, in order to be in a position to offer an operative
strategy that will decide the direction or directions that traction needs to be applied. Ignoring this
basic diagnostic step risks the possibility of failure to resolve the problem, as has been shown in a
number of the earlier bulletins on this website (see Bulletins #5 November 2011, #15 Octoer 2012, #16
November 2012). (Bulletin from March 2013, see 8)
Describing a complicated case in the May 2014 Bulletin:
This case is a prime example of the enormous advantage that CBCT has to offer in relation to plane film
radiography in the diagnosis and treatment planning of impacted teeth. As little as 15 years ago, this case
would have been a momentous failure because reliance of its positional diagnostic would have been placed
on plane film radiography only. It could still fail but, given the diagnostic imaging available today, an
accurate and planned strategy may be evolved and the chances for failure reduced very significantly.
Below is a Feb 2014 article from AJO-DO (25), with South Korean authors, relates a case of a 10-year-old with with two horizontally displaced impacted canines, used CBCT to strategies how to erupt the canines by finding the 'centers of resistance':
we located the centers of resistance in the 3-dimensionally rendered images. Using these images, we
concluded that the maxillary right was incompletely transposed, and the left canine was not transposed,
unlike the view from the 2-dimensional panoramic radiograph.
Here's a local study from UCSF and the department of orofacial sciences from 2012: 'Three-dimensional assessement of impacted canines and root resorption using CBCT' where the conclusion was:
We reliably assessed the position of impacted canines in 3 dimensions using CBCT, thereby improving
accuracy of location and facilitating precise surgical and orthodontic management.
Looking specifically at whether roots were touching each other (27) comparing panoramic images to CBCT, showed that 89% of the panoramas showed 89 false positive root contact.
'Enamel drillign for canine traction: advantages, disadvantages, description of surgical technique and biomechanics' from 2011(29) writes:
CBCT made the diagnosis of anomalies in the position of maxillary canine, also called dysgenesis, much more
effective. CBCT's various slice planes and the resulting 3D reconstructions, viewable from virtually every
angle, allows today's professionals to plan orthodontic traction of maxillary canines with greater accuracy
and refinement. This allows surgeons to deal with, their dental follicle, cervical region and adjacent teeth
with the aid of detailed planning, which ultimately reduces the risks of unintended outcomes. In other
words, technological advances in imaging have increased the chances of orthodontic traction being
accomplished more safely and accurately. It also eliminates the possibility of preexisting processes such as
external cervical resorption, alveolodental ankylosis and replacement resorption in the teeth to be
submitted to traction. When the imaging diagnosis reproduces more faithfully the actual position, the
prognosis tends to be more precise and the treatment plan can be tailored to the individual.
Lastly, from 'The Journal of Contemporary Dental Practice', Jan-Feb 2013:
The most recognized need for CBCT imaging in othodontics is that of impacted canine evaluation. CBCT
imaging is precise in determining not only the labial/lingual relationship but also a more exact angulation of
the impacted canine. Theses 3D images are beneficial in determining the proximity of adjacent incisor and
premolar roots, which can be invaluable in determining the ease of uncovering and bonding. It also helps in
deciding the vector of force that should be used to move the tooth into the arch with a lesser chance of
adjacent root resorption. (15)
Unfortunately I've seen in the radiological services' information that they not only want to do the CBCT, but also want the orthodontists/surgeons to rely on their reading of the CBCT for time saving purposes, so they can see more patients, time is money. As a patient/parent I do not want treatment from an orthodontist/oral surgeon who can't spend that time! If you can't understand a CBCT image, you are not going to be able to put that information to optimal use when you are making incisions at surgery or applying traction to a tooth while avoiding the roots of the adjacent teeth.
BE WARNED!
To give the other side it's two-cents-worth, I give you a curiously titled article 'Evidence supporting the use of CBCT in orthodontics' from JADA, March 2012, where the Dutch authors looked at 50 studies and then concluded
that 'they found no high quality evidence regarding the benefits of CBCT use in orthodontics' (23). Go figure!
BE WARNED!
To give the other side it's two-cents-worth, I give you a curiously titled article 'Evidence supporting the use of CBCT in orthodontics' from JADA, March 2012, where the Dutch authors looked at 50 studies and then concluded
that 'they found no high quality evidence regarding the benefits of CBCT use in orthodontics' (23). Go figure!
The case for an initial CBCT and as a guide before surgery
On my intro page I refer to a study called: 'the Light in the Attic' describes a case where Dr Quintero describes 'how a potentially disastrous outcome was averted'(8). It's the case with the photos on top of my page. During treatment, Dr Quintero did a smaller 'progress scan'
to evaluate root and tooth position and determine if we had cleared the root of the lateral incisor, making it
safe to force-erupt the tooth. As we had predicted, the tooth had moved perfectly, and it was now safe to
change vector of force and redirect the retraction of the canine.
This author, Dr Quintero in Florida, has also written in 'New study may change the face of orthodontics': which concludes:
One thing is for sure: With extremely low radiation doses, CBCT scanners, such as the i-CAT FLX and its
QuickScan+ setting now on the market, mark not only the end of the CBCT-in-orthodontics controversy, but
likely the future death of panos, cephs, and plaster.(7)
Dr Eraso, a radiologist/orthodontist, gave me the image of parallell parking a car, to come in wrong and then do the back and forth trying to get in the proper spo. That is not biodynamics. With unplanned traction, you can be pulling the canine into an impossible position that cannot be rectified. You want it right at the first go. Dr Eraso is promoting the use of software such as Anatomage to make dynamic study models (see 'CBCT and beyond...')
A Swedish study (4) showed that treatment plans of 43.7% (35 out of 80) children were modified after the CT investigation a year after the start of treatment. This study was looking for the effect of impacted canines on the neighboring incisiors and root resorption of these teeth.
It also states that:
When one or two maxillary canines are impacted, the occlusion is normal, and space for all teeth available,
two questions must be considered by the clinician. What is the quality of the incisor teeth? Is it possible to
use these teeth in a fixed orthodontic appliance system to correct the position of the canines in the dental
arch?
(In this case, as I understand it, a "A Siemens Somatome Plus CT scanner" is the traditional CT, while the CBCT does the same thing with less radiation).
Without the CT investigation, 11 children would not have been treated for resorption that had exposed the
pulp of an incisor root and 13 who had no root resorption on their incisors would have had one or both
lateral incisors extracted.(p 43)(4)
'Comparative analysis of traditional radiographs and CBCT volumetric images in the diagnosis and treatment planning of maxillary impacted canines'(14) a paper produced at UCSF in 2010 also showed how the treatment decision of 27 % of the cases changed between whether the tooth should be left, recovered or extracted.
The PCSO (Pacific Coast Society of Orthodontics Bulletin) winter 2008, 'The information Superhighway for Orthodontists' reviews a presentation by Dr. James Mah at an orthodontist meeting:
James discussed some of the questionable assumptions we make with our typical orthodontic X-ray series:
If the tooth refuses to move it is ankylosed. He showed a case where the CBCT revealed a previously
undetected impaction that was blocking the stubborn tooth.
If the tooth is not on the x-ray it is missing. His CBCT images revealed a cuspid up near the orbit. The tooth
was well off any panogram, and not very noticeable in the cephalogram.
Below is a conclusion from a UCSF study: "CBCT evaluation of Impacted Canines and Root Resorption" from the Department of Orofacial Sciences:
For the surgeon, knowing the precise location of the tooth provides better information as to the best
possible direction of access, and may reduce the invasiveness of surgery. Obtaining an accurate 3-D spatial
location of the impacted canine can help direct the surgeon/ortho- dontist as to what orthodontic force vector
should be applied to move the canine without causing damage to adjacent teeth.(http://www.pcsortho.org
/LinkClick.aspx?fileticket=79sM03vc6JI%3D&tabid=152)
The American Journal of Orthodontics and Dentofacial Orthopedics' had an article in May 2013 entitled: 'Impact of CBCT on orthodontic diagnosis and treatment' (14). Experienced orthodontists from PCSO, UCLA and Loma Linda participated and looked at 6 case studies.
These findings support obtaining a CBCT scan before orthodontic diagnosis and treatment planning when a
patient has an unerupted tooth with delayed eruption or a questionable location, severe root resorption as
diagnosed with a periapical or panoramic x-ray, or a severe skeletal discrepancy, the study authors noted.
Even more than these cases where teeth were saved, consider the teeth lost because there was no CBCT and no referral. It would be interesting if it could be appreciated how many impacted canines that are lost.
Dr Becker relates in his October 2012 Bulletin: 'What price negligent reading of radiograph' how badly things can go without a CBCT.
The AJO-DO (American Journal of Orthodontics & Dentofacial Orthopedics) had POINT / COUNTERPOINT
articles in April 2012. The pro writer was Dr Brent E. Larson wrote CBCT is the imaging technique of choice for
comprehensive orthodontic assessement'. He remarked in his article that:
On my intro page I refer to a study called: 'the Light in the Attic' describes a case where Dr Quintero describes 'how a potentially disastrous outcome was averted'(8). It's the case with the photos on top of my page. During treatment, Dr Quintero did a smaller 'progress scan'
to evaluate root and tooth position and determine if we had cleared the root of the lateral incisor, making it
safe to force-erupt the tooth. As we had predicted, the tooth had moved perfectly, and it was now safe to
change vector of force and redirect the retraction of the canine.
This author, Dr Quintero in Florida, has also written in 'New study may change the face of orthodontics': which concludes:
One thing is for sure: With extremely low radiation doses, CBCT scanners, such as the i-CAT FLX and its
QuickScan+ setting now on the market, mark not only the end of the CBCT-in-orthodontics controversy, but
likely the future death of panos, cephs, and plaster.(7)
Dr Eraso, a radiologist/orthodontist, gave me the image of parallell parking a car, to come in wrong and then do the back and forth trying to get in the proper spo. That is not biodynamics. With unplanned traction, you can be pulling the canine into an impossible position that cannot be rectified. You want it right at the first go. Dr Eraso is promoting the use of software such as Anatomage to make dynamic study models (see 'CBCT and beyond...')
A Swedish study (4) showed that treatment plans of 43.7% (35 out of 80) children were modified after the CT investigation a year after the start of treatment. This study was looking for the effect of impacted canines on the neighboring incisiors and root resorption of these teeth.
It also states that:
When one or two maxillary canines are impacted, the occlusion is normal, and space for all teeth available,
two questions must be considered by the clinician. What is the quality of the incisor teeth? Is it possible to
use these teeth in a fixed orthodontic appliance system to correct the position of the canines in the dental
arch?
(In this case, as I understand it, a "A Siemens Somatome Plus CT scanner" is the traditional CT, while the CBCT does the same thing with less radiation).
Without the CT investigation, 11 children would not have been treated for resorption that had exposed the
pulp of an incisor root and 13 who had no root resorption on their incisors would have had one or both
lateral incisors extracted.(p 43)(4)
'Comparative analysis of traditional radiographs and CBCT volumetric images in the diagnosis and treatment planning of maxillary impacted canines'(14) a paper produced at UCSF in 2010 also showed how the treatment decision of 27 % of the cases changed between whether the tooth should be left, recovered or extracted.
The PCSO (Pacific Coast Society of Orthodontics Bulletin) winter 2008, 'The information Superhighway for Orthodontists' reviews a presentation by Dr. James Mah at an orthodontist meeting:
James discussed some of the questionable assumptions we make with our typical orthodontic X-ray series:
If the tooth refuses to move it is ankylosed. He showed a case where the CBCT revealed a previously
undetected impaction that was blocking the stubborn tooth.
If the tooth is not on the x-ray it is missing. His CBCT images revealed a cuspid up near the orbit. The tooth
was well off any panogram, and not very noticeable in the cephalogram.
Below is a conclusion from a UCSF study: "CBCT evaluation of Impacted Canines and Root Resorption" from the Department of Orofacial Sciences:
For the surgeon, knowing the precise location of the tooth provides better information as to the best
possible direction of access, and may reduce the invasiveness of surgery. Obtaining an accurate 3-D spatial
location of the impacted canine can help direct the surgeon/ortho- dontist as to what orthodontic force vector
should be applied to move the canine without causing damage to adjacent teeth.(http://www.pcsortho.org
/LinkClick.aspx?fileticket=79sM03vc6JI%3D&tabid=152)
The American Journal of Orthodontics and Dentofacial Orthopedics' had an article in May 2013 entitled: 'Impact of CBCT on orthodontic diagnosis and treatment' (14). Experienced orthodontists from PCSO, UCLA and Loma Linda participated and looked at 6 case studies.
- A total of 64 CBCT scans were ordered. Two participants never ordered a CBCT scan for any of the cases, 16 participants ordered two to four scans, and two participants requested a CBCT scan for all six cases.
- An unerupted tooth was the most frequently cited reason for ordering a scan (64% of orders), followed by root resorption (33%).
- Of the 72 observations on patients with unerupted teeth, a CBCT scan was ordered 39 times when the characteristic was present and only twice when it was not.
- Root resorption was cited as the rationale for ordering a CBCT scan 13 times when the characteristic was present and eight times when it was not.
- Orthodontists in practice for a decade or less ordered significantly fewer CBCT exams than the more experienced orthodontists.
These findings support obtaining a CBCT scan before orthodontic diagnosis and treatment planning when a
patient has an unerupted tooth with delayed eruption or a questionable location, severe root resorption as
diagnosed with a periapical or panoramic x-ray, or a severe skeletal discrepancy, the study authors noted.
Even more than these cases where teeth were saved, consider the teeth lost because there was no CBCT and no referral. It would be interesting if it could be appreciated how many impacted canines that are lost.
Dr Becker relates in his October 2012 Bulletin: 'What price negligent reading of radiograph' how badly things can go without a CBCT.
The AJO-DO (American Journal of Orthodontics & Dentofacial Orthopedics) had POINT / COUNTERPOINT
articles in April 2012. The pro writer was Dr Brent E. Larson wrote CBCT is the imaging technique of choice for
comprehensive orthodontic assessement'. He remarked in his article that:
A truly unexpected result from our study of CBCT incidental findings in orthodontic patients was the 10% frequency of significant endodontic findings: apical periodontitis, apical radiolucency, internal or external root resorption, or retained root tips.(18) These are important items to assess before final orthodontic planning--items that could dramatically alter the treatment plan. I was convinced that this high degree of endodontic involvement was most likely a statistical anomaly since it did not correspond with my clinical experience; however, Price et al (19) recently reported a similar prevalence of endodontic findings in a different population, lending additional support to the result.
(The counterpoint opinion was held by Dr. Demetrios J. Halazonetis of the University of Athens, Greece:
CBCT is not the imaging technique of choice for comprehensive orthodontic assessment.)
CBCT is not the imaging technique of choice for comprehensive orthodontic assessment.)
Dr. Larsen's study, 'Incidence of significant Findings on CBCT Scans of an Orthodontic Patient Population' (20)
concluded that:
Of the 194 patients in this study scanned for the purpose of orthodontic diagnosis and treatment planning, 73,
or 37% demonstrated findings deemed significant enough to require a follow-up evaluation or appropriate
referral. When characterized by location, the majority of findings could be classified as being outside the orthodontic
treatment domain. The study adds support to the notion that regardless of the purpose of the CBCT scan, the entire volume
should be reviewed by a clinician competent to do so.
concluded that:
Of the 194 patients in this study scanned for the purpose of orthodontic diagnosis and treatment planning, 73,
or 37% demonstrated findings deemed significant enough to require a follow-up evaluation or appropriate
referral. When characterized by location, the majority of findings could be classified as being outside the orthodontic
treatment domain. The study adds support to the notion that regardless of the purpose of the CBCT scan, the entire volume
should be reviewed by a clinician competent to do so.
Radiation
Actually, CBCT, in the form of the i-CAT FLX QuickScann+, seems to have the blessing now in the form of an article by Dr John Ludlow (28 ) in December 2013 where he concludes that:
QuickScan+effective doses are comparable with conventional panoramic examinations. Significant dose
reductions areaccompanied by significantreductions in image quality. However, theis trade-off might be
acceptablefor certain diagnostic tasks, such as assessement of treatment results.(28)
As always when exposing a patient for a potential risk, in this case the cumulative risk of radiation exposure, it should be thought through carefully in terms of risks and benefits.
The goal for the radiation dose is ALARA= as low as reasonably achievable. And it involves a trained technician, a well written referral based on a valid need.
There is information on the FDA (US food and drug administration) website http://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX-Rays/ucm315011.htm)
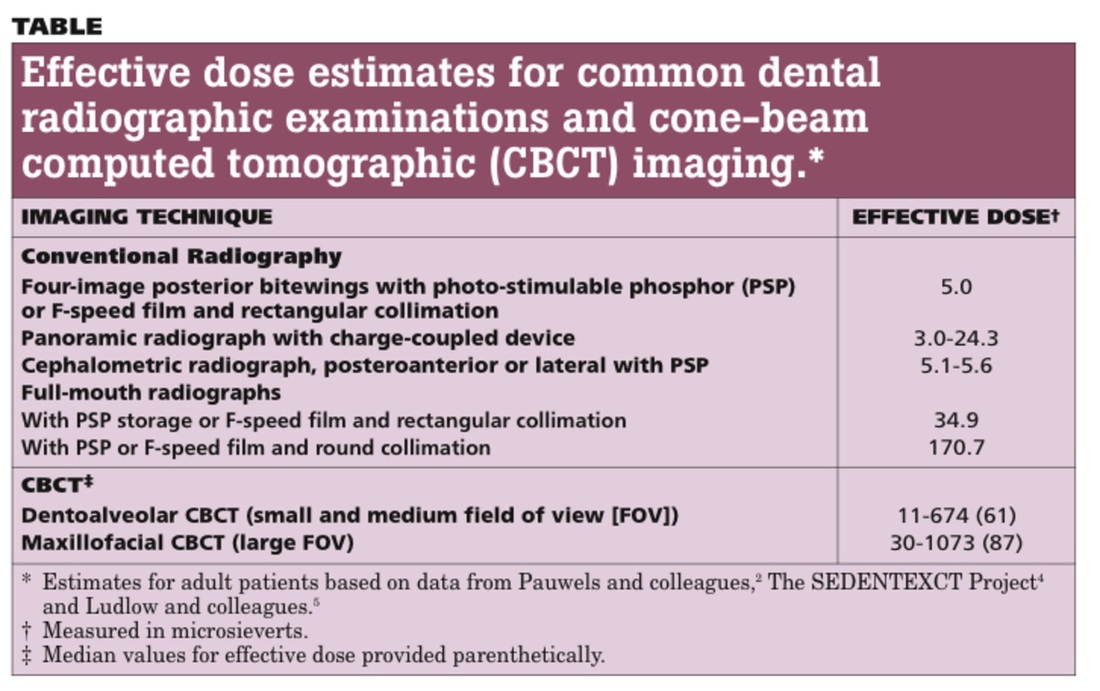
Below is a table from JADA, August 1, 2012 ( http://jada.ada.org/content/143/8/899.full). It seems like the radiation dose varies greatly depending on how it is done. So after deciding on using a CBCT, you want the dose to be "ALARA" = 'as low as reasonably achievable'. I am guessing that the amount is depends on how the referral is written and then how it is executed
Actually, CBCT, in the form of the i-CAT FLX QuickScann+, seems to have the blessing now in the form of an article by Dr John Ludlow (28 ) in December 2013 where he concludes that:
QuickScan+effective doses are comparable with conventional panoramic examinations. Significant dose
reductions areaccompanied by significantreductions in image quality. However, theis trade-off might be
acceptablefor certain diagnostic tasks, such as assessement of treatment results.(28)
As always when exposing a patient for a potential risk, in this case the cumulative risk of radiation exposure, it should be thought through carefully in terms of risks and benefits.
The goal for the radiation dose is ALARA= as low as reasonably achievable. And it involves a trained technician, a well written referral based on a valid need.
There is information on the FDA (US food and drug administration) website http://www.fda.gov/Radiation-EmittingProducts/RadiationEmittingProductsandProcedures/MedicalImaging/MedicalX-Rays/ucm315011.htm)
Below is a table from JADA, August 1, 2012 ( http://jada.ada.org/content/143/8/899.full). It seems like the radiation dose varies greatly depending on how it is done. So after deciding on using a CBCT, you want the dose to be "ALARA" = 'as low as reasonably achievable'. I am guessing that the amount is depends on how the referral is written and then how it is executed
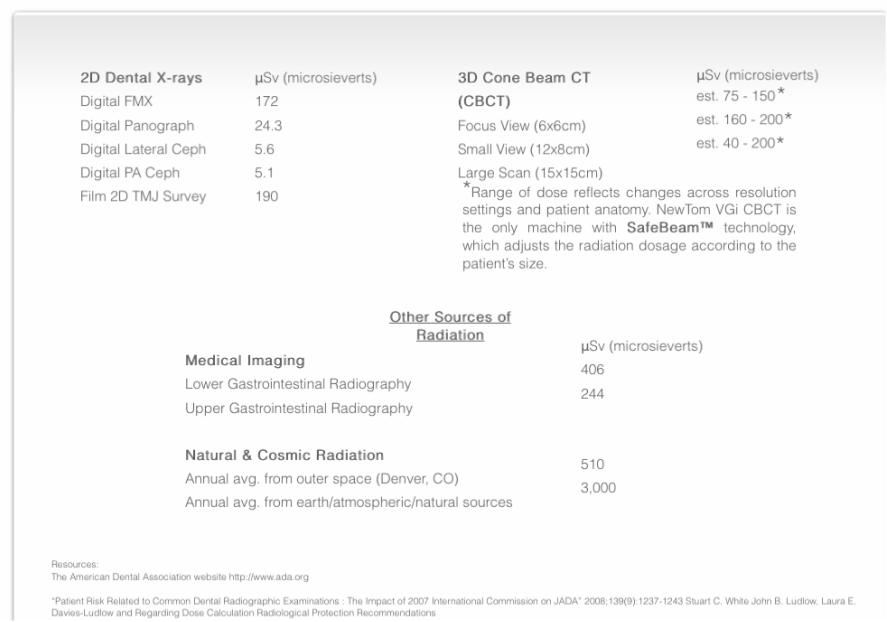
This is radiation information to patients from the website of cdental.com
C-dentals info on radiation: http://www.cdental.com/#!radiation-information/c24l0
Although the radiation doses from dental CBCT exams are generally lower than other CT exams, dental CBCT exams
typically deliver more radiation than conventional dental X-ray exams. Concerns about radiation exposure are greater for
younger patients because they are more sensitive to radiation (i.e., estimates of their lifetime risk for cancer incidence and
mortality per unit dose of ionizing radiation are higher) and they have a longer lifetime for ill effects to develop.
The FDA has launched a pediatric X-ray imaging website that provides specific recommendations for parents and health
care providers to help reduce unnecessary radiation exposure to children. The FDA’s Center for Devices and Radiological
Health defines the ages of the pediatric population as birth through 21 years.
The FDA suggests keeping a record of your child's exposure to radiation and they refer to 'The Alliance for Radiation Safety in Pedicatric imaging". Their advice for dental professionals is:
Discuss the rationale for the examination with the patient and/or parent to ensure a clear understanding of benefits and risks
Reduce the number of inappropriate referrals (i.e., justify X-ray imaging exams) by:
determining if the examination is needed to answer a clinical question,
considering alternate exams that use less or no radiation exposure, and reviewing the patient's medical imaging history to
avoid duplicate exams.
Use exposure settings for dental CBCT exams that are optimized to provide the lowest radiation dose that yields an image
quality adequate for diagnosis (i.e., radiation doses should be "As Low as Reasonably Achievable"). The technique factors
used should be chosen based on the clinical indication, patient size, and anatomical area scanned, and the equipment
should be properly maintained and tested.
A statement from the American Dental Association Council on Scientific Affairs, August 1, 2012, can be found in JADA (The Journal of the American Dental Association)
CBCT technologies offer an advanced point-of-care imaging modality that clinicians should use selectively as an adjunct to conventional dental radiography. The selection of CBCT for dental and maxillofacial imaging should be based on professional judgment in accordance with the best available scientific evidence, weighing potential patient benefits against the risks associated with the level of radiation dose. Clinicians must apply the ALARA principle in protecting patients and staff during the acquisition of CBCT images. This includes appropriate justification of CBCT use, optimizing technical factors, using the smallest FOV necessary for diagnostic purposes and using appropriate personal protective shielding
The Swedish article (4) has a section on 'dosage and relative safety'. The dosage depends on the the
kind of CBCT unit used and if it is a standard resolution or a high resolution image.
By comparison, the E20007 for digital panoramic radiographs ranges from 14 to 24 microsievert.
....
Although the risk-to-benefit ratio must be kept as low as possible, we should look to the time when CBCT
units are able to provide imaging with even lower levels of radiation. (pp. 175-176)(1)
kind of CBCT unit used and if it is a standard resolution or a high resolution image.
By comparison, the E20007 for digital panoramic radiographs ranges from 14 to 24 microsievert.
....
Although the risk-to-benefit ratio must be kept as low as possible, we should look to the time when CBCT
units are able to provide imaging with even lower levels of radiation. (pp. 175-176)(1)
Right now you can look at orthodontists's websites and check their CBCT status. I found this website drhungvu.com, that belongs to an orthodontist in Orange County, which talks extensively of the virtues of CBCT, he has a CS 9300C "one of the best CBCT machines" (yes, I can even see how orthodontists are going to compete with the latest models in a near future) and how it is used in the clinic:
The benefit for the patient is the braces can come off sooner and the side effects (such as root resorption)
are minimized...
As CBCT is adopted by more practioners, it will continue to provide numerous benefits for practioners and
patients, including improved outcomes: reduced need for exploratorory procedures; improved treatment
predictability; reduced morbidity; and potentially lowered cost and time savings.
Even when extracting an impacted tooth, is it essential to plan surgery with CBCT in order to cause as little damage as possible.
The importance of CBCT in planning the surgical extraction of impacted teeth is undeniable. The reported
case shows that a more detailed examination may assist surgical strategies, and provide valuable biological
benefits. One of the main challenges in dentistry, especially in implant dentistry, is the reconstruction of
bone defects. The unnecessary loss of the alveolar ridge has been widely condemned, because the reversion
of this condition can be very expensive. Therefore, every effort must be made to ensure the use of
surgical approaches that are as conservative as possible, in order to preserve the bone tissue.(12)
The benefit for the patient is the braces can come off sooner and the side effects (such as root resorption)
are minimized...
As CBCT is adopted by more practioners, it will continue to provide numerous benefits for practioners and
patients, including improved outcomes: reduced need for exploratorory procedures; improved treatment
predictability; reduced morbidity; and potentially lowered cost and time savings.
Even when extracting an impacted tooth, is it essential to plan surgery with CBCT in order to cause as little damage as possible.
The importance of CBCT in planning the surgical extraction of impacted teeth is undeniable. The reported
case shows that a more detailed examination may assist surgical strategies, and provide valuable biological
benefits. One of the main challenges in dentistry, especially in implant dentistry, is the reconstruction of
bone defects. The unnecessary loss of the alveolar ridge has been widely condemned, because the reversion
of this condition can be very expensive. Therefore, every effort must be made to ensure the use of
surgical approaches that are as conservative as possible, in order to preserve the bone tissue.(12)
Concern about radiation? Give patients and consumers facts
We can read about 'nutrition facts' on our food, so we can chose if we want to eat 'trans fats' or not (even if the information sometimes is obfuscated in hydrogenated fats).
Why are we not given the actual number of µSiv that x-rays and scans subject us to? This information could be collected in charts and added up, the same way that vaccinations are documented.
If things are measureable, then we don't have to rely on someone telling us it is 'low and safe' or it is
'high and risky'.
I asked and was told that the two CBCTs that Sam had were 25 µSiv and 15 µSiv. If I know that a
panoramic, with much less information, is 26 µSiv, then I, and the dentist or orthodontist, can make an intelligent decision.
(It would be useful if the yearly dosage of µSiv included air travel and airport scanners. I have been forcing my children to do the pat-down option, instead of the body scanner, but it seems that is being overly cautious and counter intuitive. You get more radiation standing in line and next to the machine,than actually going through the scanner. Pertinent information of dosage should be given out at the airports, as well as hospitals, and for dental xrays.)
We can read about 'nutrition facts' on our food, so we can chose if we want to eat 'trans fats' or not (even if the information sometimes is obfuscated in hydrogenated fats).
Why are we not given the actual number of µSiv that x-rays and scans subject us to? This information could be collected in charts and added up, the same way that vaccinations are documented.
If things are measureable, then we don't have to rely on someone telling us it is 'low and safe' or it is
'high and risky'.
I asked and was told that the two CBCTs that Sam had were 25 µSiv and 15 µSiv. If I know that a
panoramic, with much less information, is 26 µSiv, then I, and the dentist or orthodontist, can make an intelligent decision.
(It would be useful if the yearly dosage of µSiv included air travel and airport scanners. I have been forcing my children to do the pat-down option, instead of the body scanner, but it seems that is being overly cautious and counter intuitive. You get more radiation standing in line and next to the machine,than actually going through the scanner. Pertinent information of dosage should be given out at the airports, as well as hospitals, and for dental xrays.)
AAO AND AAOMR's evolving attitude: Statement in 2012 and 2013, and onward...
From "Practical Applications of CBCT in Orthodontics" (24):
In 2010, the House of Delegates of the AAO adopted a resolution that state: "RESOLVED, that the
AAO recognizes that while there may be clinical situations where CBCT may be of value, the use
of such technology is not routinely required for orthodontic radiography".
The authors continue:
The criteria for classifying a patient as routine are not defined, and the necessary diagnostic
protocols to determine if a patient is routine also are undefined. In practice, it would be
impossible to determine if a patient is routine without conducting a comprehensive evaluation.
Rather, a more practical guidelinewould be that CBCT is indicated for comprehensive
orthodontic treatment for which precise knowledge of the dentition: dentoalveolar volume; root
morphology;imp possible supernumerary, impimpacted or ankylosed teeth and other dental
abnormalities...
In 2012 it seemed the AAO was not as interested in setting up a gold standard for the benefit of patients, as they were interested in protecting the orthodontists who are not using CBCT and to make it sound as if 'to do or not to do CBCT' is a justified individual option up to the individual orthodontist. To not use CBCT when dealing with an impacted tooth is, in my opinion, is a choice made from lack of education, lack of access to a machine, lack of ability to read the images and general unwillingness to advance the science of orthodontics, everything to the the detriment of the patient, and as such, very discrediting to the profession.
In 2010, the House of Delegates of the AAO adopted a resolution that state: "RESOLVED, that the
AAO recognizes that while there may be clinical situations where CBCT may be of value, the use
of such technology is not routinely required for orthodontic radiography".
The authors continue:
The criteria for classifying a patient as routine are not defined, and the necessary diagnostic
protocols to determine if a patient is routine also are undefined. In practice, it would be
impossible to determine if a patient is routine without conducting a comprehensive evaluation.
Rather, a more practical guidelinewould be that CBCT is indicated for comprehensive
orthodontic treatment for which precise knowledge of the dentition: dentoalveolar volume; root
morphology;imp possible supernumerary, impimpacted or ankylosed teeth and other dental
abnormalities...
In 2012 it seemed the AAO was not as interested in setting up a gold standard for the benefit of patients, as they were interested in protecting the orthodontists who are not using CBCT and to make it sound as if 'to do or not to do CBCT' is a justified individual option up to the individual orthodontist. To not use CBCT when dealing with an impacted tooth is, in my opinion, is a choice made from lack of education, lack of access to a machine, lack of ability to read the images and general unwillingness to advance the science of orthodontics, everything to the the detriment of the patient, and as such, very discrediting to the profession.
I contacted the American Association of Orthodontist society to hear what the result was from the AAO and the AAOMR (American Association of Oral and Maxillofacial Radiology)'s review last year. The answer I got was that:
The essence of the joint position statement was that CBCT images might either be taken in the orthodontic office or at some other facility, and that the resulting images should be reviewed by a radiologist.
September, 2012
That the AAO thank the joint committee for their time and efforts for developing the AAO/AAOMR draft joint position statement “Clinical Recommendations for the Appropriate Use of Cone Beam Computed Tomography (CBCT) in Orthodontics”, communicate to them that the draft document will not be included in the AAO’s Clinical Practice Guidelines,
that the AAO believes it is the responsibility of each individual orthodontist to make an informed decision along with the patient or family, as to what he or she believes to be in the patient’s long-term best interest,
and further, that notice of the AAO’s position regarding the draft position paper be communicated to the membership.
On vote, motion carried.
In 2012 The European Commission set up "Cone Beam CT for Dental and Maxillofacial Radiology - evidenced based Guidelines". A hefty work of 150 pages with hundreds of references to studies. AAO should take a look at it.
Thanks to links on a southern California orthodontist's website (drhungvu.com) I found an article by Dr. James Mah, from August 2012: http://www.orthodonticproductsonline.com/orp-orthodontic-news/15003-mah-responds-to-aao-cbct-standards where he lambasts, the results of AAO and AAOMR Joint Task Force:
Summary
The AAO/AAOMR Joint Task Force has been preparing their position paper for 2.5 years and has allowed less than 3 weeks for a response from the AAO membership (Scarfe, 2012). This short response time seems inadequate and should be extended if the Joint Task Force is serious about soliciting and considering feedback from the AAO membership and other interested parties.
A significant and favorable recommendation by the Task Force is to base imaging decisions on a clinical examination, patient history, and the presence of an appropriate clinical condition that would likely have a positive benefit-to-risk ratio if imaged. The discussion about selected imaging methods would significantly improve in the position paper by including traditional imaging along with CBCT. The position paper seemed to have a bias toward the use of conventional imaging methods, including panoramic, cephalometric, and intraoral imaging projections, as the default method without employing the same use criteria being proposed for CBCT. In the clinical orthodontic practice, there is a spectrum of imaging protocols in use. At one end of the spectrum the clinician will request a full-mouth survey of periapical images, vertex occlusal, panoramic and cephalometric projections for a baseline assessment. The use of non-CBCT imaging methods can result in a relatively high effective dose without the requisite benefits. The Task Force Position Paper employed evidence-based assessment methods for CBCT and ignored a similar calibration of conventional imaging. Conventional CCD cephalometric systems do not have standardized projection geometry, and if unaccounted for, could result in clinically significant consequences (Chadwick et al, 2009).
The AAO/AAOMR draft document is lacking in many respects related to objectivity, balance, failure to apply the available evidence, and flawed recommendations. As is, it may be impossible for AAO members to follow the guidelines and may put them, their practices, and the AAO in difficult, if not impossible, situations.
The AAO/AAOMR put out a new statement in 2013: Clinical recommendations regarding use of CBCT in orthodontics. Position statement by the AAOMR
and it looks like they are now working on getting evidence based assessements to make more precise recommendations. They do note that CBCT:
has demonstrated clinical efficacy in altering treatment planning for impacted maxillary canines, unerupted
teeth, severe root resorption, and severe skeletal discrepancies
(Based on 3 studies: (4), (13) and (17))
'Appendix A:Diagnostic uses of CBCT in Orthodontics' notes 'Dental structural abnormalities, as in internal and external resorption and 'Anomalies in dental position', such as dental impactions'
and it looks like they are now working on getting evidence based assessements to make more precise recommendations. They do note that CBCT:
has demonstrated clinical efficacy in altering treatment planning for impacted maxillary canines, unerupted
teeth, severe root resorption, and severe skeletal discrepancies
(Based on 3 studies: (4), (13) and (17))
'Appendix A:Diagnostic uses of CBCT in Orthodontics' notes 'Dental structural abnormalities, as in internal and external resorption and 'Anomalies in dental position', such as dental impactions'
Latest news from Dec 2013 is that 'the Joint Commission' http://www.jointcommission.org/joint_commission_announces_new_and_revised_diagnostic_imaging_standards/
is that 'Phase two', 'to be implemented in 2015', of revising standards will contain 'minimum qualifications for clinicians who perform imaging exams, and cone beam CT used in dental offices and oral-maxillary surgery practices'
hurrah!?
is that 'Phase two', 'to be implemented in 2015', of revising standards will contain 'minimum qualifications for clinicians who perform imaging exams, and cone beam CT used in dental offices and oral-maxillary surgery practices'
hurrah!?
CBCT in the US and Canada
A study in 2010, "An Evaluation of CBCT Use in Postgraduate Orthodontic Programs in the US and Canada"(16), with 52.2 % of programs responding, showed that 83.3% of programs had access to a CBCT, 73.3 % reported regular usage, 81.8% used it for diagnostics, 18.2 % used it on every patient. Residents received didactic training in 59.1 % of programs, and hands-on in 31.8 %. Interpretation of CBCT results was the responsibility of a radiologist in 59.1 %, and 'residents were responsible for reading and referring abnormal findings in 31.8%
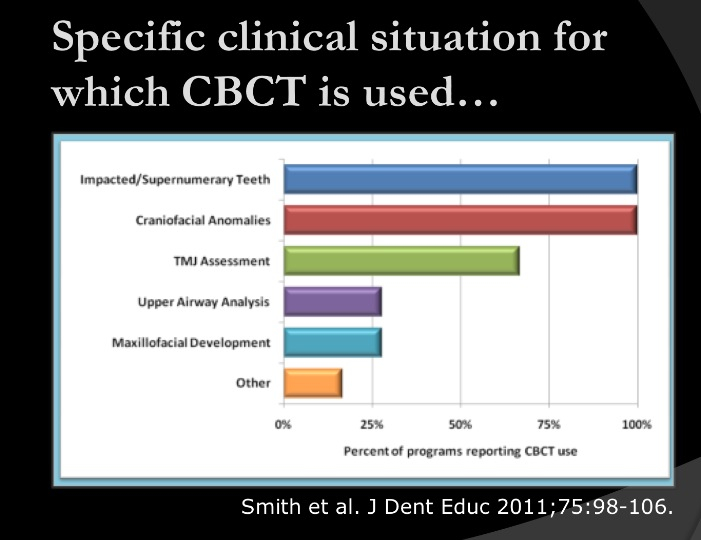
In those programs in which CBCT was only used for specific diagnoses, 100% of the programs
use it for localization of supernumerary and impacted teeth. Liu et al. (21) demonstrated the
efficacy of impacted canine localization using CBCT. Haney et al. (22) reported significant
differences in the 3D localization of the cusp tip of impacted maxillary cuspids using CBCT when
compared to using a set of conventional 2D rediographs (including a panoramic image, an
occlusal film, and two periapical radiographs together)
A study in 2010, "An Evaluation of CBCT Use in Postgraduate Orthodontic Programs in the US and Canada"(16), with 52.2 % of programs responding, showed that 83.3% of programs had access to a CBCT, 73.3 % reported regular usage, 81.8% used it for diagnostics, 18.2 % used it on every patient. Residents received didactic training in 59.1 % of programs, and hands-on in 31.8 %. Interpretation of CBCT results was the responsibility of a radiologist in 59.1 %, and 'residents were responsible for reading and referring abnormal findings in 31.8%
In those programs in which CBCT was only used for specific diagnoses, 100% of the programs
use it for localization of supernumerary and impacted teeth. Liu et al. (21) demonstrated the
efficacy of impacted canine localization using CBCT. Haney et al. (22) reported significant
differences in the 3D localization of the cusp tip of impacted maxillary cuspids using CBCT when
compared to using a set of conventional 2D rediographs (including a panoramic image, an
occlusal film, and two periapical radiographs together)
From Dr Park's Power point presentation at AAO meeting April 2014 (26)
CBCT at UCSF
A CBCT at a university clinic is $ 388 (at least at UCSF), and appears like a good investment if you are dealing with impacted canines and a tolerable expense in the grand scheme of things. The University of California at San Francisco has had a CBCT since 2004, and in May 2012, they installed a newer model which gives images with less radiation.
Dr Art Miller in the Orofacial Science Department writes on UCSF website:
We were the first institution in the US to use a CBCT system and have developed a variety of joint projects
that incorporate our orthodontic residents. The CBCT system at UCSF has now become the standard for our
Division of Orthodontics, which purchase the Hitachi MercuRay unit in 2004, and is rapidly becoming a
standard for other advanced postgraduate programs at UCSF. This work has developed a long-term
collaboration with Dr. Janice Lee and Dr. John Huang. We are at the forefront
at developing how CBCT can be used, and how craniofacial development can be followed with highly
accurate and 3D volumes that render the skeleton, the airway, and facial profile.
Dr Hung writes:
Impacted teeth may be associated with pathology. In some cases, a tooth is impacted because of adjacent
pathology, such as supernumerary tooth or neoplasm (figure2) that is not visible on standard 2-D imaging.
In other cases, pathology can occur adjacent to or secondary to an impacted tooth, such as cysts, tumors,
or inflammatory processes. Pathological findings need to be identified, diagnosed, and managed along with
the impacted tooth.
Defining 'Standard-of-care' and standards of practice
At UCSF the Department of Orthodontics and Oral Surgery hold it that CBCT is not necessary/ standard for the treatment of impacted canines. It is not even needed when it is a matter of a complicated impacted maxillary canine on a 14-year-old to do a second surgery...with resorption. Even when there is a CBCT scan made, ordered by an oral surgeon, it is not necessary that anyone look at it, the Panorex 'appear to be adequate for the purpose of carrying out the recommended surgery".. The argument put forward, defending not looking at the CBCT, by Dr. Anthony Pogrel, the head surgeon, was that articles in the New York Times in 2010 warned of the radiation:
I am sure you are aware that the New York Times has actually had this issue on their front page on a
couple of occasions with particular reference to cone-beam CTs for pediatric dentistry and orthodontics.
Like all new technologies, it must be used judiciously and appropriately and not misused.
Sam's orthodontist, Dr. Gerald Nelson, confirmed, saying there are 'regional differences', but yes, at UCSF it would not be standard and necessary to have a CBCT made to do a second round of surgery on impacted canines with resorption on a 14-year-old like Sam. It is not standard for oral surgeons. Not standard for orthodontists.
It might not be standard-of-care, but it is common sense, at least if you master the execution and reading of
CBCTs . Dr. Nelson always does it, and as cited in the PCSO Bulletin, he also does 'repeat CBCT' on patients for a study.
Something is seriously wrong if there are perfunctory CBCTs done. It is wrong if CBCTs are done for reasons other than for the best of the patient. It is wrong if the surgical and orthodontic departments don't have consensus for which patients need a CBCT. It is fundamentally wrong if CBCTs are done and not discussed by the orthodontist/oral surgeon team in order to treat a patient optimally..
And if you have 100% adherence to something, I think that is what defines 'standard'.
New York Times 2010
Here is a link to "Radiation Worries for Children in Dentists' Chairs'" from 2010/11/23, by Walt Bogdanich and Jo Craven McGinity. It states that
'there is little independent research to validate these claims. Instead the cone beam's popularity
has been fueled in part by misinformation about its saety and efficacy, some of it coming from
dentists paid or sponsored by manufactureres to give speeches, seminars and continuing
education classes...".
It cited Dr. Stuart White, former chairman of radiology at the UCLA School of Dentistry saying:
Would you like me to use a tool that is entirely safe - a camera- to record the position of your
child's teeth, or another method that may rarely cause cancer so that we can save time.
The CBCT manufactures are cited for having infomercials where orthodontists claim that 'Kids love to see the 3-D image and they can color skulls in 'green and purple'.
The positive voices in the article, "had all received speaking fees from Imaging Sciences".
According to the article there is a non radiation alternative to CBCT but it takes half-an-hour rather than the minutes that a CBCT scanner takes. However, according to a specialist, the radiation images are better on roots and 'detects hidden problems that might complicate treatment.', the argument was then translated into a $/minute and $/year perspective, making it more monetary that health issue.
CBCT discussion continued
The Pacific Coast Orthodontic Society (pcso.org) Bulletin of Summer of 2015 has several articles concerning
CBCT and references a policy statement by the American Academy of Oral and Maxillofacial Radiology from August 2013. The guidelines for CBCT in Orthodontics there states:
1. Image appropriately according to clinical condition
2. Assess the radiation dose risk
3. Minimize patient radiation exposure
4. Maintain professional competency in performing and interpreting CBCT studies.
All sounds common sensical. For a patient to get any clue of whether the referral writing clinician has done any kind of assessment of risk and benefit, ask what dose of µSiv your child is about to get exposed to.
In the Bay Area, C-dental with several
My Conclusion:
Impacted canines = CBCT + specialist orthodontist literate in CBCT. If there is a non radiation alternative to CBCT that gives enough information I would go for that too.
If this is not apparent to the dental community, it is a very logical conclusion if you are a parent who is
going to pay the $ 6000 for an orthodontist + $ 1500-2000/surgery occasion (sometimes renewed surgery is needed) for oral surgery (another $ 1000 if the surgeon wants an anesthesiologist), haul a kid in for treatments once or twice a month over a two-years-or-more period; and most importantly, if you want an end result that will work for your child. It is astounding and painful if this process of dealing with impacted canines is not taken seriously. Impacted canines need a 'state of the art' course of action that ensures parents and patients that failures are not caused by lack of training and/or lack of technology.
Several expert sources underline the importance of CBCT and from a patient/parent perspective it seems totally unjustifiable to start treating impacted canines without it.Of course, this also necessitates that there is someone competent to read it, and someone competent to treat based on the results! It should be (and I think legally it is) malpractise to extract canines without a CBCT, and to some degree trying to find the cause for failure. I'm sure this is just a matter of time, but, I want to speed it up by telling you, fellow parents, orthodontists and dental boards, that you should make it happen now, without delay.
How do you get change fast? In California I guess you sue. If you read 'Sam's case', my son's dental drama includes several villains: all dental professionals ignoring the importance of resorption, an orthodontist who wants to extract without CBCT, another orthodontist who doesn't know how to read a CBCT, an oral surgeon who doesn't need to see the CBCT to operate, and the head of oral surgery who thinks CBCT is unnecessary and dangerous,
an absurd argument, since it wasn't about doing or not doing a CBCT, it was about looking at the CBCT that had been done, ordered by the operating surgeon. Kafka!
(1) Becker A, Chaushu S. Casap-Caspi N. Cone-beam computed tomography and the orthosurgical management
of impacted teeth. JADA 141(10 suppl), October 2010.
(2) Chaushu S, Chaushu G, Becker A. The role of digital volume tomography in the imaging of impacted
teeth. World journal of orthodontics, 2004 -ncbi.nlm.nih.gov
(3) Becker A, Chaushu G, Chaushu S. Analysis of failure in the treatment of impacted canines, Am J Orthod
Dentofacial Orthop. 2010 Jun; 137(6): 743-54.
(4) Bjerklin K, Ericson S. How a computerized Tomography Examination changed the Treatment Plans of 80
Children with Retained and Ectopically Positioned Maxillary Canines.Angle Orthodonttist, Vol 76, No 1,
January, 2006, pp 43-51)
(5) Mah J, Alexandroni S. Cone-Beam Computed Tomography in the Management of Impacted Canines.
Seminars in Orthodontics, Vol 16, No 3 (September), 2010: pp199-204.
(6) Dr Becker's March 2013 bulletin: http://www.dr-adrianbecker.com/page.php?pageId=281&nlid=54
(7) http://www.i-cat.com/assets/documents/Articles--Reviews/41-43TechnologyQuintero-2.pdf
(8) Quintero J-C.'3-D imaging; the light in the attic', Ortho Tribune',
http://www.i-cat.com/assets/documents/Ortho-Case-Reports/CasereportQuintero.pdf
i-cat.com is a commercial website selling CBCT machines.
(9) Oberoi S, Knueppe S. 'Three-dimensional assessement of impacted canines and root resorption using CBCT',
Oral surgery, Oral Medicine, Oral Patology, Oral Radiology, Volume 113, Issue 2, Pages 260-267, February
2012.
(10) Becker et al. 'CBCT and the Orthosurgical Management of Impacted Teeth', JADA, Oct 2010, 141, 14S-18S.
(11) Moustafa et al.Four curious cases of CBCT'. Am J Orthod Dentoofacial Orthop. 2010 Apr; 137(4 Suppl):
S136-40./http://www.ncbi.nlm.nih.gov/pubmed/20381754
(12) Allex Morelli Heiderich de Mattos, Christiano Sampaio Queiroz, Pablo Leal Teixeira Santos, Adriana Borges
de Oliviera, Camila Oliveira, Paulo Sérgio Flores Campos. Antrum Approach planning for removal of
Impacted tooth using CBCT. Open Dent J. 2012; 6: 90–93. Published online
2012 June 1. doi: 10.2174/1874210601206010090 PMCID: PMC3379539
(13) Dentomaxillofac Radiol. 2011 Jan;40(1):24-34. doi: 10.1259/dmfr/12615645.(14) Haney E, Gansky
SA, Lee JS*, Johnson E, Maki K, Miller AJ, Huang JC. SourceDepartment of Orofacial
Sciences, School of Dentistry, University of California at San Francisco, San Francisco, Calif, USA.
Am J Orthod Dentofacial Orthop. 2010 May;137(5):590-7. doi: 10.1016/j.ajodo.2008.06.035.(15)
(14) Volume 143, Issue 5 , Pages 665-674, May 2013.
As related by http://www.drbicuspid.com/index.aspx?sec=sup_n&sub=img&pag=dis&itemId=313316
(15) Jiwanasha Manish Agrawal et al. CBCT in Orthodontics: The Wave of the Future. The Journal of
Contemporary Dental Practice, January-February 2013;14(1):153-157.
(16) Smith BR, Park JH, Cederberg. RA. Journal of Dental Education. January 1, 2011 vol. 75 no 1, pp 98-106.
(17) Hodges RJ, Atchinson KA, White SC. Impact of CBCT on orthodontic diagnosis and treatment planning. Am J
Orthod Dentofacial Orthop. 2013;143:665-674.
(18) Pliska B., DeRochr M, Larson BE. Incidence of significant findings on CBCT scans of an orthodontic patient
population. Northwest Dent. 2011,90:12-16
(19) Price JB, Thaw KL, Tyndall DA, Ludlow JB, Padilla RJ. Incidental findings from CBCT of the maxillofacial
region: a descriptive retrospective study. Clin Oral Implants Res. 2011 Sep 30
(20) Pliska et al. Incidence of Significant Findings on CBCT Scan of an Orthodontic Patient Population. Journal of
the Minnesota Dental Association. 2011.
(21) Liu et al. Localization of impacted maxillary canines and observation of adjacent incisor resorption with
CBCT. Oral Surg Oral Med Pathol Oral Radiol Endod 2008; 105(1):91-8.
(22) Haney et al. Comparative analysis of traditional radiographs and CBCT volumetric images in the diagnosis
and treatment planning of maxillary impacted canines. Am J Orthod Dentofacial Orthop 2010;
137(5):590-7.
(23) van Vlijmen et al.The Journal of American Dental Association, March 1, 2012. 143, 242-252.
(24) James Mah, John Huang, HyeRan Choo. Practical Applications of CBCT in Orthodontics. JADA, Oct 2010.
141, 7S-13S.
(25) Kyung-Keun Shi, Ji-Young Kim, Tae-Hyun Choi, Kee-Joon Lee. Timely relocation of subapically impacted
maxillary canines and replacement of an ankylosed mandibular molar are the keys to eruption disturbances
in a prepubertal patient.AJO-DO, Volume 145, Issue 2, Pages 228-237, February 2014.
(27)
(26) 'Diagnosis and Treatment of Impacted Maxillary Canines' using CBCT'
(28) Ludlow JB, Walker C. Assessement of phantom dosimetry and image quality of i-CAT FLX CBCT. Am J
Orthod Dentofacial Orthop. 2013. DEc.
(29) Filho L, Consolaro A, Almeida Cardoso, Siqueira D. Enamel drilling for canine traction: advantages,
disadvantages, description of surgical technique and biomechanics.Dental Press Journalk of Orthodontics.
vol 16 no 5 Maringá Sept./Oct. 2011.
* Ironically, Dr. Janice S. Lee, formerly of UCSF, is the surgeon who operated on Sam without looking at the
CBCT she had ordered.
** hemangiomas are small clumps of blood vessels that usually go away by themselves.They are not in any way
related to cancer.
CBCT she had ordered.
** hemangiomas are small clumps of blood vessels that usually go away by themselves.They are not in any way
related to cancer.