RESORPTION
Just the prolonged treatment with braces and manipulation can cause the roots of teeth to shorten.
|
ROOT RESORPTION from the impacted tooth
Most commonly, looking up 'resorption' in relation to impacted teeth', the 'resorption' you find is the resorption that the impacted tooth inflicts on neighboring teeth by invading their space = root resorption. This is the kind of resorption any orthodontist, endodontist, oral surgeon cannot escape knowing of. The kinds of resorptions I describe below, are the ones that you will only know of if you have read a book on impacted canines, bothered to look for it if you have a patient with the condition, go to dental school in Jordan where it is on the curriculum, or generally bother in furthering your knowledge as a dental professional. |
|

Even a successfully erupted, previously impacted caine, may come at the expense of damage to other teeth if the traction is not performed in an expert manner. If the impacted tooth is pulled too close to the adjacent teeth, they cause root resorption of these teeth, and these may be damaged and ultimately lost.
Resorption is not a new phenomenon of course, the same problems have always been there for teeth. (In 1945
JADA (32: 1003-1009) had an article on 'Resorption of embedded teeth' by Stafne and Austin.)
Today though, there should be better ways to gather the facts and make information more readily available. Resorption, like other complications should not be ignored. They have to be detected early, diagnosed and dealt with, in order to give patients the best outcome. Data on prevalence, treatment and outcomes have to be collected and analyzed if problems are to be solved.
Here is an abstract from "Management of tooth resorption" by Professor GS Heithersay, in the Department of Endodontics, at the University of Adelaide (9):
A correct diagnosis and an understanding of the aetiology and dynamics of the processes involved in tooth resorption is critical to effective management. Tooth resorptions can be classified as: (1) trauma induced; (2) infection induced; or (3) hyperplastic invasive. Some transient trauma induced resorptions require no treatment but must be carefully monitored to check that there are no complicating issues such as infection. In cases of trauma induced replacement resorption, a multidisciplinary approach is usually necessary to ensure an optimal long-term solution. Infection induced tooth resorptions require the removal of the invading micro-organisms by endodontic therapy including intra-canal medication which can also facilitate repair of the resorbed tooth structure. The hyperplastic invasive tooth resorptions pose considerable challenges in management due to the complexity and aggressive nature of the resorptive process. With careful case selection and complete inactivation of resorptive tissue successful management can be achieved.
When a patient presents with tooth resorption, the following basic questions must be addressed in arriving at a diagnosis and treatment plan:
(1) What type of resorption is present?
(2) Is the resorption external (periodontally derived), internal (pulpally derived) or communicating?
(3) Will the resorptive process be self-limiting or transient and not require management other than careful monitoring of healing processes?
(4) If the resorptive process is progressive will there be a favourable response to treatment and, if so, what is the appropriate therapy?
(5) If treated what are the short and long-term prognoses?
(6) When is extraction and prosthetic therapy indicated?
Dr Heithersay has a very clear Table in his article (9) outlining what the management each type of resorption
demands. Problem is you first have to diagnose it, and to do that as a clinician, you have to examine, take a
history of the patient, research...you need a dental professional who will bother with that.
demands. Problem is you first have to diagnose it, and to do that as a clinician, you have to examine, take a
history of the patient, research...you need a dental professional who will bother with that.
CROWN RESORPTION
Impacted third molars seems to be a quite well known to be prone to crown resorption. As it goes,
viewing the wisdom teeth as dispensable/ unwanted, resorption is just one more reason to extract, I don't know if this has been a big concern. It sounds like it is just the mere fact of being impacted that would lead to crown resorption in third molars. How does this relate to crown resorption in impacted canines?
When related to wisdom teeth it sound like common knowledge that resorption will start a counter activity of bone rebuilding.
It sounds like if you would see crown resorption on an impacted canine, this should immediately alert the treating dentist to the risk of bone formation that could potentially ankylose the tooth, and that immediate action should be taken to stop resorption/rebuilding and take action to get the tooth to erupt immediately.
Impacted third molars seems to be a quite well known to be prone to crown resorption. As it goes,
viewing the wisdom teeth as dispensable/ unwanted, resorption is just one more reason to extract, I don't know if this has been a big concern. It sounds like it is just the mere fact of being impacted that would lead to crown resorption in third molars. How does this relate to crown resorption in impacted canines?
When related to wisdom teeth it sound like common knowledge that resorption will start a counter activity of bone rebuilding.
It sounds like if you would see crown resorption on an impacted canine, this should immediately alert the treating dentist to the risk of bone formation that could potentially ankylose the tooth, and that immediate action should be taken to stop resorption/rebuilding and take action to get the tooth to erupt immediately.
ROOT RESORPTION due to the orthodontic treatment
On the website grejorgensen.com, Dr Jorgensen answers the question 'Do Braces make the Roots of Your teeth Shorter?' writes that
'Research has shown that tooth movement causes at least small changes in the shape and length of the roots
in ALL patients. In 98% however, these changes are undectable by the naked eye. In 1-2% of patients,
however, obvious root shortening occurs during routine orthodontic treatment. These patients are just more
genetically susceptible to root resorption.
On the website grejorgensen.com, Dr Jorgensen answers the question 'Do Braces make the Roots of Your teeth Shorter?' writes that
'Research has shown that tooth movement causes at least small changes in the shape and length of the roots
in ALL patients. In 98% however, these changes are undectable by the naked eye. In 1-2% of patients,
however, obvious root shortening occurs during routine orthodontic treatment. These patients are just more
genetically susceptible to root resorption.
INVASIVE CERVICAL ROOT RESORPTION (ICRR)
Dr. Heithersay is an expert on resorption and 'discovered' ICRR (invasive cervical root resorption) in 1999.
This rare condition generally develops in erupting teeth where a localized coronal enamel defect allows the invasion of aggressive hyperplastic resorptive tissue, as illustrated in Fig 21a. In this case a pink resorptive defect can be observed in an area of hypomineralization on the labial surface of the crown of the erupting central incisor tooth. Invasive coronal resorption has also been observed in teeth which have been injured by the intrusion of a primary tooth.
Radiographically the image of the resorptive defect is generally irregular in outline and, depending on its extent, the radiolucency may extend both coronally and into the radicular tooth structure as illustrated in Fig 21b.
Management: Treatment is directed towards the total removal or inactivation of all resorptive tissue and the restoration of the coronal defect. This may be achieved by physical curettage of the defect with round burs and hand instruments, but is more conveniently and effectively treated by the topical application of 90% aqueous trichloracetic acid, curettage, endodontic therapy if there is pulp involvement, and restoration of the defect with a glass ionomer cement. Orthodontic extrusion to render the defect into a supragingival position may supplement treatment if the resorption extends deeply as illustrated in Fig 21b. While the pulp can be completely or partially retained in some cases, pulpectomy and root canal filling will be required in the more extensive resorptions. (9)
Dr. Becker in his March and July bulletins 2013 (8) writes of ICCR
From a questionnaire study that we carried out among the participants of the courses that we have
recently conducted in a number of countries, we found that very few of the orthodontists present had
heard of ICRR. For those who were aware of it, few knew that it is a potent factor in failure to move the
tooth...
On the other hand, the phenomenon is well known to endodontists, pediatric dentists and dental
traumatologists, because the prevalence of ICRR following trauma or bleaching of non-vital teeth is
relatively common.
a potent cause of failure to bring about resolution of the impaction and it is rarely diagnosed
ICRR is almost completely unrecognized by orthodontists and, until this year, totally absent from the
orthodontic literature. As a distinct entity, it was brought to the notice of the dental profession by
Heithersay only in 1999 and, while endodontists and dental traumatologists will find numerous articles on
the subject in their specialist journals, orthodontists are completely ignorant of it and its clinical
implications.
Probably a good number of impacted teeth that fail to respond to orthodontic forces are likely to be
affected by ICRR to a fairly severe degree. Histologically, we have found in ICRR that, in addition to
resorption, there are also areas of deposition of bone in the resorbed areas and that this is most likely
what will have contributed to the failure. Alternatively, it may be argued that failure is due to the break in
the integrity of the PDL caused by the lesion, since eruption depends on a healthy and complete PDL.
(PDL = Periodental ligament)
ICRR can be treated with the 'Heithersay method', see this Indian case report from 2012 (www.jaypeejournals.com/eJournals/ShowText.aspxID=4464&Type=FREE&TYP=TOP&IN=~/eJournals/images/JPLOGO.gif&IID=347&isPDF=YES) = mechanical debridement, treatment with TCA (trichloroacetic acid), and restoration.
Prognosis of the treatment depends on location, size and accessability of the lesion and the structural
integrity of the tooth and periodontium after treatment is completed.'
This is Dr. Becker on ICRR in AJO-DO, April 2013 (11):
ICRR is a lesion, which in its early stages, is difficult to diagnose on a radiograph, but, by the time the lesion
has grown, bone is usually deposited in the depth of the resorption lacunae, and the tooth will no longer
respond to extrusive traction. It is our view that this is the cause of many failed impacted teeth, rather than
the knee-jerk and usually unproved application of the label 'ankylosis.' Avoidance of extensive surgery down
to the cementoenamel junction would appear to be called for, to reduce the likelihood of this possible
sequel.
Dr. Becker had an article on ICRR in the September 2013 edition of the Angle Orthodontist entitled 'Failure of Treatment of impacted canines associated with invasive cervical root resorption' where 15 referred impacted teeth with grade 3 and 4 of ICRR are discussed. Diagnosis came too late for all these teeth and they had to be extracted.
ICRR does not eliminate the physiologic mobilbity of a normal tooth and, in the earlier stages, it lacks the
metallic sound on percussion that is typical of an ankylosed tooth. The exception is in relation to the more
advanced cases, wherer hard tissue may penetrate the area, showing extensive replacement of tooth
structure by bonelike calcified tissue.
Surgical luxation and immediate reapplication of the traction force may be prescribed for an ankylosed tooth
but is inappropriate in the case of ICRR, unless the resorptive tissue is removed.
Awareness of the condition by orthodontists is of paramount importance as ICRR begins and progresses
asymptomatically, rapidly destroying the root of the tooth and extending into the crown, where it
undermines the enamel.
Treatment of early incipient ICRR lesions in erupted teeth is possible and includes exposure of the
dentionoclastic material and granulation soft tissue. ..For unerupted teeth, effective treatment depends on
ease of access.
The only imaging tool that may provide an absolute diagnosis of the existence, location and extent of the
ICRR in its early stages is CBCT.
This study does not discount the possibility that some ICRR-affected impacted teeth may bee successfully
treated by routine orthodontic traction....Whether this is because the defect that is produced in the
periodontal ligament is below a certain critical size or whether bone has not yet secondarily been deposited
in lesion remains to be determined.
CONCLUSIONS
ICRR is an overlooked cause of failure of orthodontic resolution of impacted canines.
If no movement of the impacted canine is observed, a CBCT should be considered to check for ICRR and
assess damage of adjacent teeth.
Early diagnosis is critical if the implications of ICRR are to be overcome.
Dr Becker writes again on the subject of ICRR in his December 2014 Bulletin:
The ICRR-affected tooth is prevented from responding to the extrusive orthodontic force by the resorptive
process itself and, probably, by the bony tissue that is usually laid down in the lesion, in and around the
resorption lacunae.8-10
On the other hand, if the specific area of the portal of entry of the lesion can be identified and accessed
surgically with a periodontal flap, then the affected root surface may be minimally excavated and sealed
with a glass ionomer or other cement. This needs to be done without any attempt made to remove all the
mush. On the contrary, relating to the mush as if it were dental caries will inevitably result in iatrogenic pulp
exposure and this would necessitate immediate root treatment. The reason the tooth is entirely
asymptomatic is that the resorptive process is sterile, it stops short at the predentine line and continues on
to encircle but not to penetrate the pulp. It seems that the resorptive process is prevented from advancing
by the higher organic content of the predentine layer.10 There is therefore no pulpal inflammation, no pain,
no stimulus to form secondary dentine and no direct justification for the initiation of emergency endodontic
treatment.
With the integrity of the root surface restored by placement of the glass ionomer cement, the tooth is no
longer restrained from responding to orthodontic extrusive force and an appropriate appliance placed on
the teeth will then generate the needed movement and will be able to quickly bring the restored area of
root to the surface. Extrusion should continue until the affected area of root is entirely supragingival and the
tooth should then be prepared for crowning. It will therefore be obvious that this line of treatment can only
be considered viable if the lesion is not too extensive,
Without doubt in the more advanced instances of invasive cervical root resorption, an elective root canal
treatment will often need to be performed with the aim of providing adequate retention for the final crown
and always assuming that the ICRR has left sufficient healthy root length to support the restoration.
One is permitted to wonder whether the orthodontist was responsible for the initiation of the ICRR lesion;
whether ICRR is recognized by orthodontists for the progressive pathologic entity that it is and whether the
profession-at-large is aware of the implications of the diagnosis. The fact that orthodontic treatment had
been performed on the patient does not, of itself, mean that the treatment was the trigger that initiated
the lesion. It is far more likely that trauma was the cause, as noted above. It should be recognized that
trauma to the front teeth in a young child, whether during play, a fall, a fight at school, or other similar
events, is a common occurrence. By and large, it is mild and forgotten by the next day ………. and
consequently may be conspicuously absent from the patient’s history. The absence of any follow-up
radiographs during the period of treatment, in a patient with a history of trauma and whose treatment is
unnecessarily long, is a cause for concern.
ICRR is a condition that is seen routinely in endodontic practice and it must be assumed that an endodontist
is aware of its implications regarding the prognosis of the tooth2-7. There can be little doubt that this is why
this particular endodontist advised its extraction. He may or may not have been aware of the fact that an
ICRR-affected tooth will not respond to orthodontic forces. However, did he consider the treatment option
outlined above before prescribing extraction of the tooth? Perhaps he did but considered that the lesion too
advanced for any conservative remedy.
From a questionnaire study that we carried out among the participants of the courses that we have
recently conducted in a number of countries, we found that very few of the orthodontists present had
heard of ICRR. For those who were aware of it, few knew that it is a potent factor in failure to move the
tooth...
On the other hand, the phenomenon is well known to endodontists, pediatric dentists and dental
traumatologists, because the prevalence of ICRR following trauma or bleaching of non-vital teeth is
relatively common.
a potent cause of failure to bring about resolution of the impaction and it is rarely diagnosed
ICRR is almost completely unrecognized by orthodontists and, until this year, totally absent from the
orthodontic literature. As a distinct entity, it was brought to the notice of the dental profession by
Heithersay only in 1999 and, while endodontists and dental traumatologists will find numerous articles on
the subject in their specialist journals, orthodontists are completely ignorant of it and its clinical
implications.
Probably a good number of impacted teeth that fail to respond to orthodontic forces are likely to be
affected by ICRR to a fairly severe degree. Histologically, we have found in ICRR that, in addition to
resorption, there are also areas of deposition of bone in the resorbed areas and that this is most likely
what will have contributed to the failure. Alternatively, it may be argued that failure is due to the break in
the integrity of the PDL caused by the lesion, since eruption depends on a healthy and complete PDL.
(PDL = Periodental ligament)
ICRR can be treated with the 'Heithersay method', see this Indian case report from 2012 (www.jaypeejournals.com/eJournals/ShowText.aspxID=4464&Type=FREE&TYP=TOP&IN=~/eJournals/images/JPLOGO.gif&IID=347&isPDF=YES) = mechanical debridement, treatment with TCA (trichloroacetic acid), and restoration.
{kind=link}
Prognosis of the treatment depends on location, size and accessability of the lesion and the structural
integrity of the tooth and periodontium after treatment is completed.'
This is Dr. Becker on ICRR in AJO-DO, April 2013 (11):
ICRR is a lesion, which in its early stages, is difficult to diagnose on a radiograph, but, by the time the lesion
has grown, bone is usually deposited in the depth of the resorption lacunae, and the tooth will no longer
respond to extrusive traction. It is our view that this is the cause of many failed impacted teeth, rather than
the knee-jerk and usually unproved application of the label 'ankylosis.' Avoidance of extensive surgery down
to the cementoenamel junction would appear to be called for, to reduce the likelihood of this possible
sequel.
Dr. Becker had an article on ICRR in the September 2013 edition of the Angle Orthodontist entitled 'Failure of Treatment of impacted canines associated with invasive cervical root resorption' where 15 referred impacted teeth with grade 3 and 4 of ICRR are discussed. Diagnosis came too late for all these teeth and they had to be extracted.
ICRR does not eliminate the physiologic mobilbity of a normal tooth and, in the earlier stages, it lacks the
metallic sound on percussion that is typical of an ankylosed tooth. The exception is in relation to the more
advanced cases, wherer hard tissue may penetrate the area, showing extensive replacement of tooth
structure by bonelike calcified tissue.
Surgical luxation and immediate reapplication of the traction force may be prescribed for an ankylosed tooth
but is inappropriate in the case of ICRR, unless the resorptive tissue is removed.
Awareness of the condition by orthodontists is of paramount importance as ICRR begins and progresses
asymptomatically, rapidly destroying the root of the tooth and extending into the crown, where it
undermines the enamel.
Treatment of early incipient ICRR lesions in erupted teeth is possible and includes exposure of the
dentionoclastic material and granulation soft tissue. ..For unerupted teeth, effective treatment depends on
ease of access.
The only imaging tool that may provide an absolute diagnosis of the existence, location and extent of the
ICRR in its early stages is CBCT.
This study does not discount the possibility that some ICRR-affected impacted teeth may bee successfully
treated by routine orthodontic traction....Whether this is because the defect that is produced in the
periodontal ligament is below a certain critical size or whether bone has not yet secondarily been deposited
in lesion remains to be determined.
CONCLUSIONS
ICRR is an overlooked cause of failure of orthodontic resolution of impacted canines.
If no movement of the impacted canine is observed, a CBCT should be considered to check for ICRR and
assess damage of adjacent teeth.
Early diagnosis is critical if the implications of ICRR are to be overcome.
Dr Becker writes again on the subject of ICRR in his December 2014 Bulletin:
The ICRR-affected tooth is prevented from responding to the extrusive orthodontic force by the resorptive
process itself and, probably, by the bony tissue that is usually laid down in the lesion, in and around the
resorption lacunae.8-10
On the other hand, if the specific area of the portal of entry of the lesion can be identified and accessed
surgically with a periodontal flap, then the affected root surface may be minimally excavated and sealed
with a glass ionomer or other cement. This needs to be done without any attempt made to remove all the
mush. On the contrary, relating to the mush as if it were dental caries will inevitably result in iatrogenic pulp
exposure and this would necessitate immediate root treatment. The reason the tooth is entirely
asymptomatic is that the resorptive process is sterile, it stops short at the predentine line and continues on
to encircle but not to penetrate the pulp. It seems that the resorptive process is prevented from advancing
by the higher organic content of the predentine layer.10 There is therefore no pulpal inflammation, no pain,
no stimulus to form secondary dentine and no direct justification for the initiation of emergency endodontic
treatment.
With the integrity of the root surface restored by placement of the glass ionomer cement, the tooth is no
longer restrained from responding to orthodontic extrusive force and an appropriate appliance placed on
the teeth will then generate the needed movement and will be able to quickly bring the restored area of
root to the surface. Extrusion should continue until the affected area of root is entirely supragingival and the
tooth should then be prepared for crowning. It will therefore be obvious that this line of treatment can only
be considered viable if the lesion is not too extensive,
Without doubt in the more advanced instances of invasive cervical root resorption, an elective root canal
treatment will often need to be performed with the aim of providing adequate retention for the final crown
and always assuming that the ICRR has left sufficient healthy root length to support the restoration.
One is permitted to wonder whether the orthodontist was responsible for the initiation of the ICRR lesion;
whether ICRR is recognized by orthodontists for the progressive pathologic entity that it is and whether the
profession-at-large is aware of the implications of the diagnosis. The fact that orthodontic treatment had
been performed on the patient does not, of itself, mean that the treatment was the trigger that initiated
the lesion. It is far more likely that trauma was the cause, as noted above. It should be recognized that
trauma to the front teeth in a young child, whether during play, a fall, a fight at school, or other similar
events, is a common occurrence. By and large, it is mild and forgotten by the next day ………. and
consequently may be conspicuously absent from the patient’s history. The absence of any follow-up
radiographs during the period of treatment, in a patient with a history of trauma and whose treatment is
unnecessarily long, is a cause for concern.
ICRR is a condition that is seen routinely in endodontic practice and it must be assumed that an endodontist
is aware of its implications regarding the prognosis of the tooth2-7. There can be little doubt that this is why
this particular endodontist advised its extraction. He may or may not have been aware of the fact that an
ICRR-affected tooth will not respond to orthodontic forces. However, did he consider the treatment option
outlined above before prescribing extraction of the tooth? Perhaps he did but considered that the lesion too
advanced for any conservative remedy.
Dr Becker's Bulletin for December 2014 describes the case of a 17-year-old girl loosing central incisor where
ICRR was not diagnosed and treated in time. He talks more about the treatment of ICRR affected teeth.
The ICRR-affected tooth is prevented from responding to the extrusive orthodontic force by the resorptive process itself and, probably, by the bony tissue that is usually laid down in the lesion, in and around the resorption lacunae.8-10
On the other hand, if the specific area of the portal of entry of the lesion can be identified and accessed surgically with a periodontal flap, then the affected root surface may be minimally excavated and sealed with a glass ionomer or other cement. This needs to be done without any attempt made to remove all the mush. On the contrary, relating to the mush as if it were dental caries will inevitably result in iatrogenic pulp exposure and this would necessitate immediate root treatment. The reason the tooth is entirely asymptomatic is that the resorptive process is sterile, it stops short at the predentine line and continues on to encircle but not to penetrate the pulp. It seems that the resorptive process is prevented from advancing by the higher organic content of the predentine layer.10 There is therefore no pulpal inflammation, no pain, no stimulus to form secondary dentine and no direct justification for the initiation of emergency endodontic treatment.
With the integrity of the root surface restored by placement of the glass ionomer cement, the tooth is no longer restrained from responding to orthodontic extrusive force and an appropriate appliance placed on the teeth will then generate the needed movement and will be able to quickly bring the restored area of root to the surface. Extrusion should continue until the affected area of root is entirely supragingival and the tooth should then be prepared for crowning. It will therefore be obvious that this line of treatment can only be considered viable if the lesion is not too extensive,
Without doubt in the more advanced instances of invasive cervical root resorption, an elective root canal treatment will often need to be performed with the aim of providing adequate retention for the final crown and always assuming that the ICRR has left sufficient healthy root length to support the restoration.
One is permitted to wonder whether the orthodontist was responsible for the initiation of the ICRR lesion; whether ICRR is recognized by orthodontists for the progressive pathologic entity that it is and whether the profession-at-large is aware of the implications of the diagnosis. The fact that orthodontic treatment had been performed on the patient does not, of itself, mean that the treatment was the trigger that initiated the lesion. It is far more likely that trauma was the cause, as noted above. It should be recognized that trauma to the front teeth in a young child, whether during play, a fall, a fight at school, or other similar events, is a common occurrence. By and large, it is mild and forgotten by the next day ………. and consequently may be conspicuously absent from the patient’s history. The absence of any follow-up radiographs during the period of treatment, in a patient with a history of trauma and whose treatment is unnecessarily long, is a cause for concern.
ICRR is a condition that is seen routinely in endodontic practice and it must be assumed that an endodontist is aware of its implications regarding the prognosis of the tooth2-7. There can be little doubt that this is why this particular endodontist advised its extraction. He may or may not have been aware of the fact that an ICRR-affected tooth will not respond to orthodontic forces. However, did he consider the treatment option outlined above before prescribing extraction of the tooth? Perhaps he did but considered that the lesion too advanced for any conservative remedy.
ICRR, I am conjecturing, is what is called External Cervical Resorption (ECR) in a Brazilian article (18):
During surgical removal of the of the dental follicle the dentin gaps present in all human teeth, including
deciduous teeth, are inevitably exposed to connective tissue after the flap is folded back over the tooth. The
exposure of these dentin proteins, defined as sequestered antigens, can induce, over weeks or months, an
immunological process of elimination that is clinically known as ECR. This process may occur during
orthodontic traction or after the tooth has reached the occlusal plane. In many such cases a belated
detection tends to be the rule. ECR is defined as a slow, painless, insiduous process that does not
compromise pulp tissues. In more advanced cases, it can lead to gingival inflammation and pulpitis secondary
to bacterial contamination. One way to prevent this is to leave at least 2 mm of soft tissue from the dental
follicle attached to the cervical region.
During surgical removal of the of the dental follicle the dentin gaps present in all human teeth, including
deciduous teeth, are inevitably exposed to connective tissue after the flap is folded back over the tooth. The
exposure of these dentin proteins, defined as sequestered antigens, can induce, over weeks or months, an
immunological process of elimination that is clinically known as ECR. This process may occur during
orthodontic traction or after the tooth has reached the occlusal plane. In many such cases a belated
detection tends to be the rule. ECR is defined as a slow, painless, insiduous process that does not
compromise pulp tissues. In more advanced cases, it can lead to gingival inflammation and pulpitis secondary
to bacterial contamination. One way to prevent this is to leave at least 2 mm of soft tissue from the dental
follicle attached to the cervical region.
PRE-ERUPTIVE INTRA-CORONAL RADIOLUCENCY/RESORPTION (PEIR or PECR)

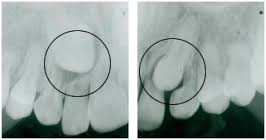
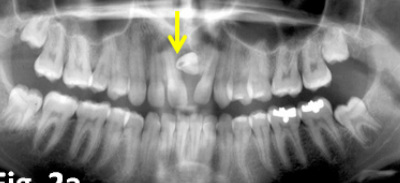
PEIR is the resorption of dentin starting in the dentin-enamel junction, usually at the crown of a molar, before the tooth has erupted. It sounds like there is some kind of fissure or defect in the surface that gets the process started. There is no pain, no bacteria, and no symptoms. You find it on x-rays as a 'radiolucency' and and at surgery. The resorption continues insidiously inside the tooth, the outside can appear normal, even as the tooth turns to mush inside, covered by an enamel shell.
It was first thought to be due to 'occult caries', but it has since been, supposedly?, established that bacteria are not present in unerupted teeth ("caries cannot occur in a fully embedded tooth"(1)).
As the lesion resembles caries, they are often referred to as 'pre-eruptive caries'. There is little scientific
basis for this nomenclature as a pre-eruptive, developing tooth which is completely encased in its crypt is
not likely to be infected with cariogenic microorganisms. (14)
The condition was first described and documented in 1941: 'Intra-follicular caries' (, but even today "its prevalence and etiology remain largely unknown'' (3).
Actually, some authors still describe the condition as 'hidden caries', here is an article from January 2012 by authors from the Columbia and New York Universities: 'Hidden carries a concern for pediatric dentists and orthodontists." The article states: 'An interesting finding in the Seow et al study was that close to 28% of unerupted ectopic teeth were associated with pre-eruptive dentin defects, either in itself, or on an adjacent tooth.' I can't find that number in the article they mention (14), it cites several studies and numbers all over the place, anything from 0.8 to 50%, 'in spite of its relatively high prevalence, the etiology and patogenesis of occult caries remain unclear' (14). The conclusion is:
Bitewing radiographs are useful for detecting early occlusal fissure caries while panorex radiographs of
unerupted developing teeth aid in the diagnosis of pre-eruptive intracoronal lesions. It is suggested that
that all unerupted, developing teeth on radiographs be examined for pre-eruptive resorptive lesions. (14)
Why is ICRR and PEIR unrecognized by orthodontists? It certainly is not a new phenomenon, but somehow it has been ignored, deemed non relevant. It is curious that ignorance is not more easily fixed in the internet age. Information, if you are looking for it, seems plentiful. (Unfortunately Sam is a point in case, nobody
was really interested in researching the resorption, at a university too no less, nobody cared to consider if and how resorption would influence treatment, and surgery took place without planning for the right course of action. Dr. Becker seems to think that endodontists and oral surgeons know better, but it is not the case at UCSF.)
A December 2013 article in the European Archives of Paediatric Dentistry, 'Pre-eruptive intracoronal radiolucencies in the permanent dentition of Jordanian children' (15) with 1,571 children found a prevalence of 8.1% by subject and 0.62% by teeth. The authors' conclusion was:
PEIR defects occur at a significant prevalence rate in unerupted teeth. Increased awareness and careful
radiographic examination of unerupted teeth may improve early detection and treatment of PEIR defects in
children.
Compare the frequency to 'impacted teeth' which afflicts around 1-2%, and you would think it worth knowing about for every dentist and orthodontist.
While over 60 teeth with pre-eruptive intracoronal lesions have been reported in over 25 case reports,
beginning as early as 1941 (Table 2), the prevalence of this entity was unknown until recently.
...
To date, clinical and histological evidence substantiate the hypothesis that these defects are acquired, as a
result of coronal resorption. In the pre-eruptive state, these lesions were reported to
contain soft tissue when examined during surgical exposure. Histological examination often reveals signs
of resorption such as scalloping of the lesion margins, as well as resorptive cells such as osteoclasts and
macrophages.The resorptive cells are thought to enter the dentin through poorly coalesced enamel
fissures or the cemento-enamel junction. Although trigger factors for the resorption are unknown,
a high association of ectopic positioning of affected teeth or in the adjacent abutting teeth was reported in
controlled studies, which suggests that abnormal local pressure may be an inciting factor for the
resorption.
...
Although trigger factors for the resorption are unknown, a high association of ectopic positioning of affected
teeth or in the adjacent abutting teeth was reported in controlled studies, which suggests that abnormal local
pressure may be an inciting factor for the resorption.
...
Early diagnosis of occult lesions is the best management. As radiographs are prob- ably the most effective
method of diagnosing all occult lesions, they should be recommended at appropriate ages to aid early
detection of these lesions. Also, examination of the crowns of unerupted teeth for intracoronal defects is
suggested on all rou- tine radiographs.
A study by the Faculty of Dentistry of Malaya, Kuala Lumpur, from 2003 found a 27.3% (sic!) incidence of pre-eruptive dentin defects.
The high prevalence of the condition indicates the need for increased awareness and recognition of this
during radiographic examination of the teeth in the pediatric group in early pre-eruptive stages so that
early detection and diagnosis can be made and treatment can be done at the most appropriate time.(7)
Treatment of PEIR
According to a 2012 article in the European Archives of Pediatric Dentistry (15) entitled Case Report: Idiopathic pre-eruptive coronal resorption of a maxillary permanent canine (15):
In the past the treatment for 'an unerupted tooth [with resorption] was surgical exposure by removing the
overlaying soft tissue and curettage of the defects followed by lining with calcium hydroxide and restoration
[Sullivan and Jolly, 1957; Wood and Crozier, 1985](12)
.....
More recently it has been suggested that for the more progressive lesion, it is important to conserve the tooth
by surgical exposure [Dowling et al., 1999]. Alternatively, if the lesion is thought to be slowly progressive, it
should be allowed to erupt and then treatment can be commenced immediately upon eruption.
...
Conclusion
Teeth affected by idiopathic pre-eruptive coronal resorption can be retained if the problem is intercepted at
an early stage and appropriate restorative procedures are performed. It is prudent to make an early
diagnosis of the condition and to formulate short and long-term treatment plans, which may involve keeping
the affected tooth to retain the alveolar bone height and width to allow for the option of planing an implant.
Looking at the Jordan University School of Dentistry website, which is excellent!, I found that they had PEIR on their schedule for 2008-9. At UCSF it is an unknown!
A Chinese study, Prevalence of preeruptive radiolucency in Chinese children from panoramic radiographs (16)
found a prevalence of 0.85% by subject with 707 panoramas. That would be 10 times less than with CBCT in
the Jordanian study.
See Dr Becker's July 2014 newsletter where he describes the treatment of an 18-year-old woman with a dilacerated, impacted central incisor with PEIR! It's orthodontics at it's best!
It was first thought to be due to 'occult caries', but it has since been, supposedly?, established that bacteria are not present in unerupted teeth ("caries cannot occur in a fully embedded tooth"(1)).
As the lesion resembles caries, they are often referred to as 'pre-eruptive caries'. There is little scientific
basis for this nomenclature as a pre-eruptive, developing tooth which is completely encased in its crypt is
not likely to be infected with cariogenic microorganisms. (14)
The condition was first described and documented in 1941: 'Intra-follicular caries' (, but even today "its prevalence and etiology remain largely unknown'' (3).
Actually, some authors still describe the condition as 'hidden caries', here is an article from January 2012 by authors from the Columbia and New York Universities: 'Hidden carries a concern for pediatric dentists and orthodontists." The article states: 'An interesting finding in the Seow et al study was that close to 28% of unerupted ectopic teeth were associated with pre-eruptive dentin defects, either in itself, or on an adjacent tooth.' I can't find that number in the article they mention (14), it cites several studies and numbers all over the place, anything from 0.8 to 50%, 'in spite of its relatively high prevalence, the etiology and patogenesis of occult caries remain unclear' (14). The conclusion is:
Bitewing radiographs are useful for detecting early occlusal fissure caries while panorex radiographs of
unerupted developing teeth aid in the diagnosis of pre-eruptive intracoronal lesions. It is suggested that
that all unerupted, developing teeth on radiographs be examined for pre-eruptive resorptive lesions. (14)
Why is ICRR and PEIR unrecognized by orthodontists? It certainly is not a new phenomenon, but somehow it has been ignored, deemed non relevant. It is curious that ignorance is not more easily fixed in the internet age. Information, if you are looking for it, seems plentiful. (Unfortunately Sam is a point in case, nobody
was really interested in researching the resorption, at a university too no less, nobody cared to consider if and how resorption would influence treatment, and surgery took place without planning for the right course of action. Dr. Becker seems to think that endodontists and oral surgeons know better, but it is not the case at UCSF.)
A December 2013 article in the European Archives of Paediatric Dentistry, 'Pre-eruptive intracoronal radiolucencies in the permanent dentition of Jordanian children' (15) with 1,571 children found a prevalence of 8.1% by subject and 0.62% by teeth. The authors' conclusion was:
PEIR defects occur at a significant prevalence rate in unerupted teeth. Increased awareness and careful
radiographic examination of unerupted teeth may improve early detection and treatment of PEIR defects in
children.
Compare the frequency to 'impacted teeth' which afflicts around 1-2%, and you would think it worth knowing about for every dentist and orthodontist.
While over 60 teeth with pre-eruptive intracoronal lesions have been reported in over 25 case reports,
beginning as early as 1941 (Table 2), the prevalence of this entity was unknown until recently.
...
To date, clinical and histological evidence substantiate the hypothesis that these defects are acquired, as a
result of coronal resorption. In the pre-eruptive state, these lesions were reported to
contain soft tissue when examined during surgical exposure. Histological examination often reveals signs
of resorption such as scalloping of the lesion margins, as well as resorptive cells such as osteoclasts and
macrophages.The resorptive cells are thought to enter the dentin through poorly coalesced enamel
fissures or the cemento-enamel junction. Although trigger factors for the resorption are unknown,
a high association of ectopic positioning of affected teeth or in the adjacent abutting teeth was reported in
controlled studies, which suggests that abnormal local pressure may be an inciting factor for the
resorption.
...
Although trigger factors for the resorption are unknown, a high association of ectopic positioning of affected
teeth or in the adjacent abutting teeth was reported in controlled studies, which suggests that abnormal local
pressure may be an inciting factor for the resorption.
...
Early diagnosis of occult lesions is the best management. As radiographs are prob- ably the most effective
method of diagnosing all occult lesions, they should be recommended at appropriate ages to aid early
detection of these lesions. Also, examination of the crowns of unerupted teeth for intracoronal defects is
suggested on all rou- tine radiographs.
A study by the Faculty of Dentistry of Malaya, Kuala Lumpur, from 2003 found a 27.3% (sic!) incidence of pre-eruptive dentin defects.
The high prevalence of the condition indicates the need for increased awareness and recognition of this
during radiographic examination of the teeth in the pediatric group in early pre-eruptive stages so that
early detection and diagnosis can be made and treatment can be done at the most appropriate time.(7)
Treatment of PEIR
According to a 2012 article in the European Archives of Pediatric Dentistry (15) entitled Case Report: Idiopathic pre-eruptive coronal resorption of a maxillary permanent canine (15):
In the past the treatment for 'an unerupted tooth [with resorption] was surgical exposure by removing the
overlaying soft tissue and curettage of the defects followed by lining with calcium hydroxide and restoration
[Sullivan and Jolly, 1957; Wood and Crozier, 1985](12)
.....
More recently it has been suggested that for the more progressive lesion, it is important to conserve the tooth
by surgical exposure [Dowling et al., 1999]. Alternatively, if the lesion is thought to be slowly progressive, it
should be allowed to erupt and then treatment can be commenced immediately upon eruption.
...
Conclusion
Teeth affected by idiopathic pre-eruptive coronal resorption can be retained if the problem is intercepted at
an early stage and appropriate restorative procedures are performed. It is prudent to make an early
diagnosis of the condition and to formulate short and long-term treatment plans, which may involve keeping
the affected tooth to retain the alveolar bone height and width to allow for the option of planing an implant.
Looking at the Jordan University School of Dentistry website, which is excellent!, I found that they had PEIR on their schedule for 2008-9. At UCSF it is an unknown!
A Chinese study, Prevalence of preeruptive radiolucency in Chinese children from panoramic radiographs (16)
found a prevalence of 0.85% by subject with 707 panoramas. That would be 10 times less than with CBCT in
the Jordanian study.
See Dr Becker's July 2014 newsletter where he describes the treatment of an 18-year-old woman with a dilacerated, impacted central incisor with PEIR! It's orthodontics at it's best!
Dr Becker's thoughts on PEIR (and talking of Sam's case specifically):
The crown resorption that has occurred is due to clastic cells whose origin is the PDL and not the pulp. I see it as analogous in
virtually every detail to invasive cervical root resorption (ICRR) that we published in the Angle Orthodontist earlier this year
(Becker A, Abramovitz I, Chaushu S. Failure of treatment of impacted canines associated with invasive cervical root resorption.
Angle Orthodontist, 2013,83:870-876) and was the subject of our presentation at the AAO meeting in Hawaii last year (it's on
the disk from the meeting). Additionally, pre-eruptive crown resorption was the subject of the July 2013 Bulletin on my
website athttp://www.dr-adrianbecker.com/page.php?pageId=273This is not caries, but resorption. According to the research
(see list of refs in that article), it attacks the body of the dentine but stops short at the predentine, which has a much higher
organic content and probably does not actually get through to expose the pulp. The diagnosis that there is an open connection
was presumably made radiographically, which must be viewed with some suspicion. If the resorption mush is cleared away
meticulously, as if it were caries, instrumentation will certainly push through the predentine layer. Cutting off the lesion by
minimal mush removal and sealing it off (with the deeper mush still inside) with glass ionomer or other filling material, will
effectively stop the resorption by starvation - since its nourishment comes from the PDL and not from the pulp. According to
the same research (and again relying on the high degree of similarity between this form of crown resorption and ICRR), in
advanced stages, bone is deposited in the lesion (see list of references in the article) and I would hazard an informed guess
that this is the factor that stops the tooth from responding to extrusive forces - as in a pure ankylosis.For these reasons, I
have recommended surgery to expose the teeth and to seal off the lesions and then to try again. If I am right, the teeth
should respond to well directed traction. Once the teeth erupt, then endo can be done under ideal conditions - if it is required
for reasons of retention of a crown. Leaving the mush in place and properly sealed, it should not cause a pulpal reaction
during this entire period, because it is sterile, uninfected, and now non-progressive. It is not caries and it should not be
treated as such, because it contains no bacteria and therefore it does not generate pulp inflammation.
It is entirely possible that my conclusions are not as well founded as I like to believe, but these points represent my line of
thinking and are the basis for the recommendations that I made in my correspondence
The crown resorption that has occurred is due to clastic cells whose origin is the PDL and not the pulp. I see it as analogous in
virtually every detail to invasive cervical root resorption (ICRR) that we published in the Angle Orthodontist earlier this year
(Becker A, Abramovitz I, Chaushu S. Failure of treatment of impacted canines associated with invasive cervical root resorption.
Angle Orthodontist, 2013,83:870-876) and was the subject of our presentation at the AAO meeting in Hawaii last year (it's on
the disk from the meeting). Additionally, pre-eruptive crown resorption was the subject of the July 2013 Bulletin on my
website athttp://www.dr-adrianbecker.com/page.php?pageId=273This is not caries, but resorption. According to the research
(see list of refs in that article), it attacks the body of the dentine but stops short at the predentine, which has a much higher
organic content and probably does not actually get through to expose the pulp. The diagnosis that there is an open connection
was presumably made radiographically, which must be viewed with some suspicion. If the resorption mush is cleared away
meticulously, as if it were caries, instrumentation will certainly push through the predentine layer. Cutting off the lesion by
minimal mush removal and sealing it off (with the deeper mush still inside) with glass ionomer or other filling material, will
effectively stop the resorption by starvation - since its nourishment comes from the PDL and not from the pulp. According to
the same research (and again relying on the high degree of similarity between this form of crown resorption and ICRR), in
advanced stages, bone is deposited in the lesion (see list of references in the article) and I would hazard an informed guess
that this is the factor that stops the tooth from responding to extrusive forces - as in a pure ankylosis.For these reasons, I
have recommended surgery to expose the teeth and to seal off the lesions and then to try again. If I am right, the teeth
should respond to well directed traction. Once the teeth erupt, then endo can be done under ideal conditions - if it is required
for reasons of retention of a crown. Leaving the mush in place and properly sealed, it should not cause a pulpal reaction
during this entire period, because it is sterile, uninfected, and now non-progressive. It is not caries and it should not be
treated as such, because it contains no bacteria and therefore it does not generate pulp inflammation.
It is entirely possible that my conclusions are not as well founded as I like to believe, but these points represent my line of
thinking and are the basis for the recommendations that I made in my correspondence
I wrote Dr. Heithersay at at the Department of Endodontics in Adelaide, Australia, an expert on resorption
and received this reply:
In our endodontic clinic we have treated two cases with similar histories of frustrated orthodontic treatment where no movement could be activated despite similar coronal exposure as that carried out for Sam . One of these cases also had pre-eruptive invasive coronal resorption. After a multidisciplinary consultation involving an orthodontist, and a peridontist and our endodontic group, it was decided in both cases to treat the unerupted teeth be intentional transplantation, with concurrent treatment of the resorptive defect and endodontic treatment in the case with pre-eruptive invasive coronal resorption. The teeth were very carefully removed surgically with special attention to avoid damage to the root surface. Before the teeth were transplanted into a newly created socket site, the root sufaces were treated with Emdogain and after transplantation, the bone defect was filled with a combination of Bio-oss and Collagen and the area was then covered with Bioguide which is a resorbable membrane. In the tooth without the pre-eruptive invasive coronal resorption, endodontic treatment was commenced prior to the transplantation, but an intra-canal dressing was placed incorporating a cortico-steroid antibiotic combination as this has been shown to control potential reesorption. The tooth will be root filled after some weeks.
The patient with the pre-eruptive resorption has been followed up for two years to date and there has been excellent progress.
Transplantation of unerupted canines is not a new technique- it has been used for many years- an orthodontist named Moss published an impressive series in the early 70's while an extensive study has been carried out by Dr Jens Andreasen of Copenhagen- he and his surgical team have very impressive results.
The patient with the pre-eruptive resorption has been followed up for two years to date and there has been excellent progress.
Transplantation of unerupted canines is not a new technique- it has been used for many years- an orthodontist named Moss published an impressive series in the early 70's while an extensive study has been carried out by Dr Jens Andreasen of Copenhagen- he and his surgical team have very impressive results.
'Other' resorptions
'Resorption of the crown in impacted maxillary canine: A clinical, radiographic and histologic study. B. Azaz, A. Shteyer. Department of oral surgery, The Hebrew University Hadassah School of Dentistry, Jerusalem, Israel,International Journal of Oral Surgery, Vol 7, Issue 3, June 1978, p 167-171. Abstract:
Thirty-six maxillary impacted canines which showed coronary resorption were selected out of 252 impacted canines. Clinical,
radiographic and histologic observations were performed. In the majority of the cases (31) a local inflammatory factor was
present and only in five cases was the resorption idiopathic. The incidence of resorption was highest in the later decades of
life. In all cases bone replacement was found.
The study above is cited in the Nigerian Journal of Clinical Practice, December 2002, Vol. 5 (2) p91-98, in an article by O.O.da Costa entitled "The unerupted Maxillary Canine":
Coronal resorption of the maxillary canine is another possible complication of long standing impaction. Azaz and Shteyer
reported a 14% occurence of resorption among the impacted canines seen in their study. Complete impaction over a long
period of time was an important aetiological factor. Most cases were seen in patients over 40 years and above.It has been
suggested that local inflammatory factors such as non-vital teeth, periodontal pockets or chronic irritation from dentures may
act as predisposing factors leading to the destruction of enamel epithelium and initiation of enamel resorption...External
resorption of the crown occurs more frequently than root resorption and occasionally the whole tooth may be destroyed
without symptoms. However, due to the difficulty in removing the tooth in this condition Seddon and Smith concluded that
only in cases where it is necessary should this be done e.g. cystic change, fitting of prostheses or presence of symptoms.
"Early arrested development and coronal resorption of an impacted maxillary canine: report of cases" (13)
Coronal resorption of maxillary canines is a possible complication of long standing impaction. Degeneration of the enamel
epithelium allows the connective tissues to come into direct contact with enamel. Irregular replacement of the pericoronal
tissues and resorbed enamel by bone characterizes the histological picture. Inflammatory changes are rare. Resorption of
enamel is slow and usually symptomless so that reported cases have usually been incidental radiographic findings in older
patients. This report presents the early arrested development, ankylosis and resorption of the crown of a maxillary canine in a
child 7.7-years-old. Arrest of crown development occurred between three and four-years-of-age. Radiographically the crown of
the canine was incompletely formed and showed irregular resorption. Serial radiographs taken over a five-year period showed
movement of the canine superiorly in relation to the hard palate which was taken as radiographic evidence for ankylosis of the
resorbing maxillary canine in a growing child.
The importance of early diagnosis, the need for an endodontist and a treatment plan
Specialists in orthodontics are often the first to see the radiographs of unerupted permanent teeth; therefore, they
have the responsibility to be aware of the condition, diagnose it, and consult with an endodontist for a treatment
plan for the teeth with intracoronal resorption. Decisive for the orthodontic treatment plan is, first, the
endodontist's evaluation of whether the tooth can be preserved and the prognosis for the tooth. Only after this
evaluation can the orthodontist determine a treatment plan. Since orthodontic treatment planning depends on
diagnostics of the dentition, type of malocclusion, and cooperation, each patient with with preeruptive intracoronal
resorption requires an individual treatment plan. The only guidance recommended from this study would be to
consult an endodontist in the initial phase.(1)
The management of pre-eruptive dentin radiolucencies depends largely on the extent of radiolucency at the time
of diagnosis. A rapidly progressive and large lesion in a tooth which is still unerupted should indicate immediate
surgical exposure, and curettage of the defects followed by lining with calcium hydroxide and restoration with
dental cements or amalgam.(3)
The consequence of neglecting diagnosis and adequate treatment
If the condition is not picked up on before eruption by way of x-rays, it can be missed, and it could be interpreted as bacterial decay. If a tooth erupts with this condition unmanaged it is highly susceptible to bacteria. One case tells how it wasn't discovered until the orthodontist took off the band around the tooth and the whole tooth just collapsed.
Somehow, orthodontists, dentists and oral surgeons have not been alerted to this condition even though it doesn't seem to be that rare of a thing and the phenomenon of radiolucency was reported 70 years ago. To advance science, awareness is number one as everyone who has looked at this are advocating. As it is I get a feeling that ICRR and PEIR has fallen by the wayside.
Without diagnosis, close observation and treatment, the tooth is eaten away from the inside, in some cases it sounds like it's a quick and progressiv decay, in some cases the PEIR is slower
(see: http://www.ncbi.nlm.nih.gov/pubmed/15587105?dopt=Abstract).
If a PEIR tooth is treated by someone without knowledge of the condition, they could cause damage that might be irreversible. If the pulp is exposed by poking at 'the mush', the tooth is doomed.
Note the progression of this lesion on the mandibular left second premolar. Operative efforts were
extensive and involved a pulp-capping procedure for a tooth that might have been restored far more
conservatively if the early and smaller lesion had been detected by the orthodontist while he/she was
scrutinizing the panoramic radiograph for other more routine orthodontic areas of interest and concern
(Figure 8).(6)
Collection of case studies
|
Dr Becker's 2014 July Bulletin presents a case of an 18-year-old with an impacted, dilacerated, central incisor with PEIR. You don't have to be an orthodontist to appreciate how Dr Becker could solve a problem like that and what it must have meant to that young woman! Dr Becker repaired the PEIR lesion, there was no apicoectomy or root canal therapy. The PEIR lesion was clearly seen and was sealed off with composite material, without any attempt to excavate the mush within. The rationale for this is that the lesion is not carious, but it is non-bacterial and completely sterile, receiving its nutrient supply through the dental follicle, from which it was isolated by the composite filling. ... Since the tooth has responded to vitality testing and is symptomless, it is hoped that this represents an area of immature bone that is the result of the extensive root movement of the tooth, which will disappear as further calcification proceeds. Careful radiographic monitoring has been introduced to oversee developments during the succeeding months. |
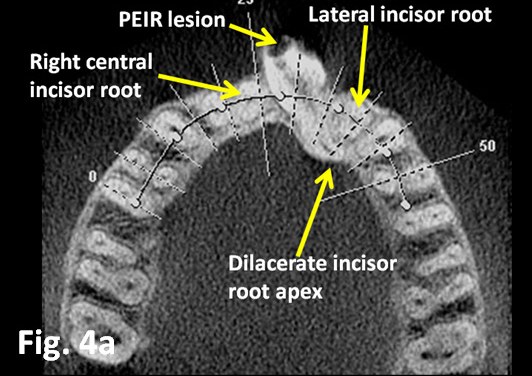
Dr Becker's July 2014 Bulletin is entitled
"Unraveling intertwined incisor roots"

|
'Treatment of Severe Pre-eruptive Intracoronal Resorption of a Permanent Second Molar',E. Davidovitch et al., Pediatric Dentistry, 27:1, 2005:www.aapd.org/assets/1/25/Peretz-27-1.pdf
11-year-old referred to the university clinic because of a transluscent area in unerupted permanent mandibular molar. It was exposed and "caries-like tissue was removed with low-speed round bur...the cavity floor was lined with glass ionomer. ...Three months later the tooth erupted" and a partial pulpectomy was performed. Six-month follow-up good, continued root development.
Discussion:...The dental literature generally recommends surgical exposure of the unerupted tooth - as
soon as the lesion has been diagnosed radiographically - to arrest the progression of the resorptive
progress and prevent its penetration into the dental pulp...
Conclusions: Early diagnosis and treatment of PEIR are essential to avoid pulp involvement after tooth
eruption
Pre-eruptive coronal resorption of a maxillary canine: A case report Omar Yaqoob etc.,
14-year-old with impacted canine. After 22 months of braces a panoramic (pre-surgery) showed extensive coronal damage of the tooth. After another 26 months the 'condition had progressed to such a degree that extensive restorative treatment was necessary'...The patient was anxious to have his orthodontic appliances removed; therefore, due to the extensive nature of the lesion, a definitive solution was likely to involve prosthodontic rehabilitation....
Conclusion: PECR is a rare condition that may arise during adolescence and undergo rapid progression
without any warning signs. If resorption remains undetected for extended period, it may culminate in loss
of affected teeth, necessitating prostethic or combined orthodontic-restorative treatment.(5)
14-year-old with impacted canine. After 22 months of braces a panoramic (pre-surgery) showed extensive coronal damage of the tooth. After another 26 months the 'condition had progressed to such a degree that extensive restorative treatment was necessary'...The patient was anxious to have his orthodontic appliances removed; therefore, due to the extensive nature of the lesion, a definitive solution was likely to involve prosthodontic rehabilitation....
Conclusion: PECR is a rare condition that may arise during adolescence and undergo rapid progression
without any warning signs. If resorption remains undetected for extended period, it may culminate in loss
of affected teeth, necessitating prostethic or combined orthodontic-restorative treatment.(5)
'Case Report: Pre-eruptive intra-coronal radiolucencies revisited. Study in European Archives of Pediatric Dentistry, 2012:
Two cases, a 6-year-old and a 12 year-old where the teeth affected erupted. The 6 year old could keep her tooth after it was restored with a metal crown. The twelve-year-old came with extensive damage, the tooth had to be extracted.
Conclusion: Early detection and classification of the PEIR lesion allows an array of individualised
treatments to be provided for successful outcome.(1)
Two cases, a 6-year-old and a 12 year-old where the teeth affected erupted. The 6 year old could keep her tooth after it was restored with a metal crown. The twelve-year-old came with extensive damage, the tooth had to be extracted.
Conclusion: Early detection and classification of the PEIR lesion allows an array of individualised
treatments to be provided for successful outcome.(1)
Case report: 'Idiopathic PEIR of a permanent maxillary canine' (12)
Describes case of 13-year-old with PEIR:
A periapical radiograph (Fig. 2) showed no evidence of a retained primary canine. While a panoramic
radiograph (Fig. 3), which had been taken about a year previously, revealed a coronal radiolucency
resembling a carious lesion on the permanent canine with evidence of a retained primary canine.
Describes case of 13-year-old with PEIR:
A periapical radiograph (Fig. 2) showed no evidence of a retained primary canine. While a panoramic
radiograph (Fig. 3), which had been taken about a year previously, revealed a coronal radiolucency
resembling a carious lesion on the permanent canine with evidence of a retained primary canine.
A comment to the (1) article relates a case where they did not take the endodontist's advice of root filling:
We referred the patient to an endodontist who suggested that the tooth be root filled and a temporary
crown placed, followed later by a post crown. Since the patient now is now only 15 years old and
undergoing full orthodontic treatment, we have opted to have the tooth extracted and the space closed
orthodontically, with the first premolar substituting for the canine. In our opinion, endodontic treatment of
a tooth that has just erupted commits the patient to a post crown, which might not last a lifetime. In a case
already undergoing full orthodontic treatment, serious consideration should be given to extracting the tooth
and substituting it with an adjacent healthy tooth.(4)
We referred the patient to an endodontist who suggested that the tooth be root filled and a temporary
crown placed, followed later by a post crown. Since the patient now is now only 15 years old and
undergoing full orthodontic treatment, we have opted to have the tooth extracted and the space closed
orthodontically, with the first premolar substituting for the canine. In our opinion, endodontic treatment of
a tooth that has just erupted commits the patient to a post crown, which might not last a lifetime. In a case
already undergoing full orthodontic treatment, serious consideration should be given to extracting the tooth
and substituting it with an adjacent healthy tooth.(4)
(Worth exploring further:
I found endodontist in Arizona, Dr. John J. Stropko (www.stropko.com), who practices micro surgery and is the
inventor of the 'Stropko Irrigator'.)
I found endodontist in Arizona, Dr. John J. Stropko (www.stropko.com), who practices micro surgery and is the
inventor of the 'Stropko Irrigator'.)
MY CONCLUSION:
As with the impaction in general, it appears that there is an alarming lack of standard of care and risk of teeth lost because patients are not getting optimal care. Also lost with the teeth, is the science that could be extracted (pardon pun) by collecting case studies and data.
All the studies that do exist on PEIR, point to the importance of awareness and also to a suspicion that PEIR might be relatively prevalent. There is need for evidence-based science here! Problem is that orthodontists have these teeth extracted without a second thought, and that at least UCSF, lacks the knowledge and interest to look at PEIR when it appears at their clinic! The professors haven't heard of it, and their students, the next generation of dental professionals, will not hear of it either.
With the internet it should not have to take another 70 years for PEIR to get properly explored and to get an evidence based consensus of what constitutes the best care! Can't the Dental Board issue information to all professions involved, that resorption and PEIR is a condition you, as a dental professional, are expected to be aware of, and that you need to keep at the cutting edge of, or at least to be aware enough to refer patients to someone with expertise? Any resorption in a tooth should give rise to some research into what it is!
As with the impaction in general, it appears that there is an alarming lack of standard of care and risk of teeth lost because patients are not getting optimal care. Also lost with the teeth, is the science that could be extracted (pardon pun) by collecting case studies and data.
All the studies that do exist on PEIR, point to the importance of awareness and also to a suspicion that PEIR might be relatively prevalent. There is need for evidence-based science here! Problem is that orthodontists have these teeth extracted without a second thought, and that at least UCSF, lacks the knowledge and interest to look at PEIR when it appears at their clinic! The professors haven't heard of it, and their students, the next generation of dental professionals, will not hear of it either.
With the internet it should not have to take another 70 years for PEIR to get properly explored and to get an evidence based consensus of what constitutes the best care! Can't the Dental Board issue information to all professions involved, that resorption and PEIR is a condition you, as a dental professional, are expected to be aware of, and that you need to keep at the cutting edge of, or at least to be aware enough to refer patients to someone with expertise? Any resorption in a tooth should give rise to some research into what it is!
For an expose on the different resorptions, see Dr Becker's February 2015 Newsletter, where he describes:
1. Root resorption as a by-product of routine orthodontic treatment
2. Resorption of the root of the adjacent tooth assocaited with the aberrant eruptive progress of an impacted
canine
3. Invasive cervical root resorption (ICRR) of the impacted tooth itself, causing failure of eruption and resistance
of eruption mechanism.
4. Apical root resorption causing root shortening of the anchor teeth.
5. Pre-eruptive intra-coronal resorption (PEIR)
6. Surface resorption of enamel
1. Root resorption as a by-product of routine orthodontic treatment
2. Resorption of the root of the adjacent tooth assocaited with the aberrant eruptive progress of an impacted
canine
3. Invasive cervical root resorption (ICRR) of the impacted tooth itself, causing failure of eruption and resistance
of eruption mechanism.
4. Apical root resorption causing root shortening of the anchor teeth.
5. Pre-eruptive intra-coronal resorption (PEIR)
6. Surface resorption of enamel
(1) Inger Kjaer etc., Preeruptive intracoronal resorption observed in 13 patients, Am J Dentofacial Orthop
2012;142:129-32.
www.ajodo.org/article/S0889-5406(12)00362-9/abstract
(2) Dr.K.P Counihan, A. C. O'Connell. Case Report: Pre-eruptive intra-coronal radiolucencies revisited.
European Archives of Pediatric Dentistry. August 2012, Volume
13, Issue 4, pp 221-226. http://www.ncbi.nlm.nih.gov/pubmed/22883363
(3) Kim Seow et al. The prevalence of pre-eruptive dentin radiolucencies in the permanent dentiotion.
Pediatric Dentistry, 21:1,1999.)
(4) http://ajodoblog.blogspot.com/2012/08/letter-pre-eruptive-intracoronal.html
(5) Yaqoob et al. Pre-eruptive coronal resorption of a maxillary canine: A case report. WJO. Vol 12,
Nummber2, 2011.(www.quintpub.com/userhome/wjo/ortho_12_2_Yaqoob_web_11.pdf)
(6) www.orthopracticeus.com/web/home/clinical/226-hidden-cariesa-concern-for-pediatric-dentists-
and-orthodontists.html
(7) (Nik et al. Pre-eruptive intracoronal dentin defects of permanent teeth. J Clin Dent 2003;27 (4):371-5.
http://www.ncbi.nlm.nih.gov /pubmed/12924738
(8) http://www.dr-adrianbecker.com/page.php?pageId=281&nlid=59
(9) Australian Dental Journal Supplement 2007;52:(1 Supp;):S 105-121
(10) Davidovich E, Kreiner B, Peretz B. Treatment of severe pre-eruptive intracoronal resorption. Pediatr Dent.
2005, Jan-Feb; 27(1):74-7.
(11) Becker A, Chu Stella. Palatally impacted canines: The case for closed surgical exposure and immediate
orthodontic traction. Ajo-Do, Volume 143, Issue 4, p 451, April 2013.
(12) http://www.thefreelibrary.com/Case+report%3A+Idiopathic+pre-eruptive+coronal+resorption+of+a...-a0290066492
Manan, N.M.; Mallineni, S.K.; King, N.M.April 1, 2012.
(13) Sedon RP, Orth D, Smith PB. Early arrested development and coronal resorption of an impacted maxillary
canine: a case report.ASDC J Dent Child, 1966 May-June; 63(3): 208-12
(14) Seow K. 'PEIR as an entity of occult caries', American Academy of Pediatric Dentistry - 22:5, 2000.
Dr Seow is a Professor in pediatric dentistry at the University of Queensland, Brisbane, Australia.
(15) Al-Batayneh OB et al. Pre-eruptive intracoronal dentine radiolucencies in the permanent dentition of
Jordanian children. European Archives of Paediatric Dentistry, December 2013.
Dr. Al-Batayneh is Assistant Professor in Pediatric Dentistry, Faculty of Dentistry, Jordan University of
Science & Technology.
(16) Wang Y, Chen J, Liu H. Prevalence of preeruptive intracoronal radiolucency in Chinese children from
panoramic radiographs. Chin J Dent REs. 2013; 16(2): 153-6.
(17) Skillen WG (1941) Intra-follicular caries. Ill Dent J 10:307-308.
(18) Capelozza Filho L, Consolaro A, Cardoso MA, Siqueira DF. Enamel drilling for canine traction: advantages,
disadvantages, description of surgical technique and biomechanics.Dental Press Journalk of Orthodontics.
vol 16 no 5 Maringá Sept./Oct. 2011.
2012;142:129-32.
www.ajodo.org/article/S0889-5406(12)00362-9/abstract
(2) Dr.K.P Counihan, A. C. O'Connell. Case Report: Pre-eruptive intra-coronal radiolucencies revisited.
European Archives of Pediatric Dentistry. August 2012, Volume
13, Issue 4, pp 221-226. http://www.ncbi.nlm.nih.gov/pubmed/22883363
(3) Kim Seow et al. The prevalence of pre-eruptive dentin radiolucencies in the permanent dentiotion.
Pediatric Dentistry, 21:1,1999.)
(4) http://ajodoblog.blogspot.com/2012/08/letter-pre-eruptive-intracoronal.html
(5) Yaqoob et al. Pre-eruptive coronal resorption of a maxillary canine: A case report. WJO. Vol 12,
Nummber2, 2011.(www.quintpub.com/userhome/wjo/ortho_12_2_Yaqoob_web_11.pdf)
(6) www.orthopracticeus.com/web/home/clinical/226-hidden-cariesa-concern-for-pediatric-dentists-
and-orthodontists.html
(7) (Nik et al. Pre-eruptive intracoronal dentin defects of permanent teeth. J Clin Dent 2003;27 (4):371-5.
http://www.ncbi.nlm.nih.gov /pubmed/12924738
(8) http://www.dr-adrianbecker.com/page.php?pageId=281&nlid=59
(9) Australian Dental Journal Supplement 2007;52:(1 Supp;):S 105-121
(10) Davidovich E, Kreiner B, Peretz B. Treatment of severe pre-eruptive intracoronal resorption. Pediatr Dent.
2005, Jan-Feb; 27(1):74-7.
(11) Becker A, Chu Stella. Palatally impacted canines: The case for closed surgical exposure and immediate
orthodontic traction. Ajo-Do, Volume 143, Issue 4, p 451, April 2013.
(12) http://www.thefreelibrary.com/Case+report%3A+Idiopathic+pre-eruptive+coronal+resorption+of+a...-a0290066492
Manan, N.M.; Mallineni, S.K.; King, N.M.April 1, 2012.
(13) Sedon RP, Orth D, Smith PB. Early arrested development and coronal resorption of an impacted maxillary
canine: a case report.ASDC J Dent Child, 1966 May-June; 63(3): 208-12
(14) Seow K. 'PEIR as an entity of occult caries', American Academy of Pediatric Dentistry - 22:5, 2000.
Dr Seow is a Professor in pediatric dentistry at the University of Queensland, Brisbane, Australia.
(15) Al-Batayneh OB et al. Pre-eruptive intracoronal dentine radiolucencies in the permanent dentition of
Jordanian children. European Archives of Paediatric Dentistry, December 2013.
Dr. Al-Batayneh is Assistant Professor in Pediatric Dentistry, Faculty of Dentistry, Jordan University of
Science & Technology.
(16) Wang Y, Chen J, Liu H. Prevalence of preeruptive intracoronal radiolucency in Chinese children from
panoramic radiographs. Chin J Dent REs. 2013; 16(2): 153-6.
(17) Skillen WG (1941) Intra-follicular caries. Ill Dent J 10:307-308.
(18) Capelozza Filho L, Consolaro A, Cardoso MA, Siqueira DF. Enamel drilling for canine traction: advantages,
disadvantages, description of surgical technique and biomechanics.Dental Press Journalk of Orthodontics.
vol 16 no 5 Maringá Sept./Oct. 2011.