Part 1 of
An Orthodontic Odyssey (or 'why I wake up at 3 am')
A series of unfortunate events.....
Really, I can't believe how we could have such bad luck in every aspect all the way along...and I can't wait for this to be over and done with, and Sam out of braces.
It feels like 'Boyhood' with braces.
Trauma to front teeth 2006, age 8 and 1/2 years
I am relating the case of my son Sam to illustrate some of the points I've made on this website.
Also I recommend any parent to keep complete records of their own, because I've found I've had to rely on my iPAD many times when the dental offices can't find pictures or have technical problems.
Sam has not had any cavities in his life, and at 8 it looked as if he had good space for his developing teeth, but he had a very regrettable trauma to his permanent front teeth at age 8 1/2 (August 11, 2006). Sam was doing jumps in the bathroom while laughing, and landed with his permanent upper front teeth on the formica. They were both chipped.
We arrived frantic at the office of Sam's pediatric dentist, the chipped pieces in milk. The dentist said that the teeth had to rest after the trauma and there was nothing to be done, they looked a bit puzzled by the chips and the chips went in the refrigerator. When asked about bonding, the dentist said 'he'd ask around', he had no experience of bonding and thought we could ask our own 'adult' dentist about what to do.
We spent the day researching on the web and ended up at UCSF the following morning. The chips were bonded back on and they have held up since. (Sam will need more dental work on these teeth when his teeth are fully developed.)
Really, I can't believe how we could have such bad luck in every aspect all the way along...and I can't wait for this to be over and done with, and Sam out of braces.
It feels like 'Boyhood' with braces.
Trauma to front teeth 2006, age 8 and 1/2 years
I am relating the case of my son Sam to illustrate some of the points I've made on this website.
Also I recommend any parent to keep complete records of their own, because I've found I've had to rely on my iPAD many times when the dental offices can't find pictures or have technical problems.
Sam has not had any cavities in his life, and at 8 it looked as if he had good space for his developing teeth, but he had a very regrettable trauma to his permanent front teeth at age 8 1/2 (August 11, 2006). Sam was doing jumps in the bathroom while laughing, and landed with his permanent upper front teeth on the formica. They were both chipped.
We arrived frantic at the office of Sam's pediatric dentist, the chipped pieces in milk. The dentist said that the teeth had to rest after the trauma and there was nothing to be done, they looked a bit puzzled by the chips and the chips went in the refrigerator. When asked about bonding, the dentist said 'he'd ask around', he had no experience of bonding and thought we could ask our own 'adult' dentist about what to do.
We spent the day researching on the web and ended up at UCSF the following morning. The chips were bonded back on and they have held up since. (Sam will need more dental work on these teeth when his teeth are fully developed.)
Pulling all baby canines 2009, age 11 and 3 months
Sam, at age 11 and 3 months, in May and June of 2009, had his 4 baby canines extracted to make space for his permanent teeth.
(Money aspect: extraction $ 192 x 4= $ 768, nitrous oxide $ 75 x 2 = $ 150, total: $ 918)
(Image documentation: $300)
Then we waited. When we checked in with an orthodontist, we were reassured that the teeth were on their way, and waited some more. In December of 2010, age 12, the right side canines, both upper and lower, still had not erupted spontaneously, (It is more unusual to have a lower, mandibular, canine that is impacted) and we were told Sam would need surgery.
Sam, at age 11 and 3 months, in May and June of 2009, had his 4 baby canines extracted to make space for his permanent teeth.
(Money aspect: extraction $ 192 x 4= $ 768, nitrous oxide $ 75 x 2 = $ 150, total: $ 918)
(Image documentation: $300)
Then we waited. When we checked in with an orthodontist, we were reassured that the teeth were on their way, and waited some more. In December of 2010, age 12, the right side canines, both upper and lower, still had not erupted spontaneously, (It is more unusual to have a lower, mandibular, canine that is impacted) and we were told Sam would need surgery.
Begin braces February 2011
(Money aspect: $5 900, with $300 deduction for records already made)
We started braces with orthodontist #1. Now we heard that we were late and the root tips were almost all formed, which supposedly reduced the chances of a successful treatment. Sam got braces in February of 2011 (13 years old), and space was created for the canines over the next 9 months.
Sam was then referred to a periodontist for the exposing and bonding to get a chain on the canines. (Orthodontist # 1 said that he referred to a periodontist instead of an oral surgeon since it was less traumatic for the teeth and the patient, and no need for general anesthesia.)
The periodontist said Sam's canines were out of her reach and Sam needed an oral surgeon.
(Money aspect: $5 900, with $300 deduction for records already made)
We started braces with orthodontist #1. Now we heard that we were late and the root tips were almost all formed, which supposedly reduced the chances of a successful treatment. Sam got braces in February of 2011 (13 years old), and space was created for the canines over the next 9 months.
Sam was then referred to a periodontist for the exposing and bonding to get a chain on the canines. (Orthodontist # 1 said that he referred to a periodontist instead of an oral surgeon since it was less traumatic for the teeth and the patient, and no need for general anesthesia.)
The periodontist said Sam's canines were out of her reach and Sam needed an oral surgeon.
Resorption of impacted canine crowns
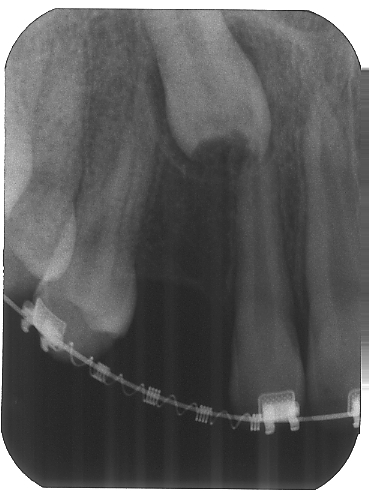
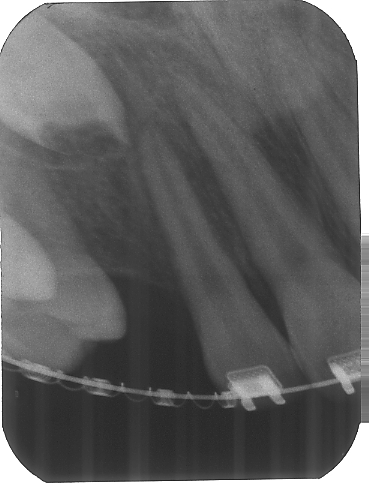
Nobody has been able to explain, while out of the blue, the crown of #6 is damaged on x-rays from 2010. And pre surgery periapicals from September 15, 2011 show the damaged crowns.
Speculations have been trauma to front teeth, baby teeth roots left in situ...
Unfortunately, nobody considered the possible effects resorption, or even more importantly, a progressive resorption and its effect on the attempts to pull the canines into place, until I email Dr. Becker in August of 2012 after reading his article on PEIR.
Nobody has been able to explain, while out of the blue, the crown of #6 is damaged on x-rays from 2010. And pre surgery periapicals from September 15, 2011 show the damaged crowns.
Speculations have been trauma to front teeth, baby teeth roots left in situ...
Unfortunately, nobody considered the possible effects resorption, or even more importantly, a progressive resorption and its effect on the attempts to pull the canines into place, until I email Dr. Becker in August of 2012 after reading his article on PEIR.

|
|
|
|
Expose & bond # 1, 10/7/2011
(Money aspect: $ 2 043)
Sam was referred to a periodontist for the exposing and bonding to get a chain on the canines.
(Orthodontist # 1 said that he referred to a periodontist instead of an oral surgeon since it was less traumatic for the teeth and the patient, and no need for general anesthesia.) The periodontist said Sam's canines were out of her reach and Sam needed an oral surgeon.
The oral surgeon # 1 pointed out that Sam's right maxillary canine, #6, has an irregular outline of the crown, something Sam's dentist had also seen on x rays. No definite explanation for it. One theory was that the trauma to Sam's front teeth could have interfered with his unerupted permanent canines somehow.
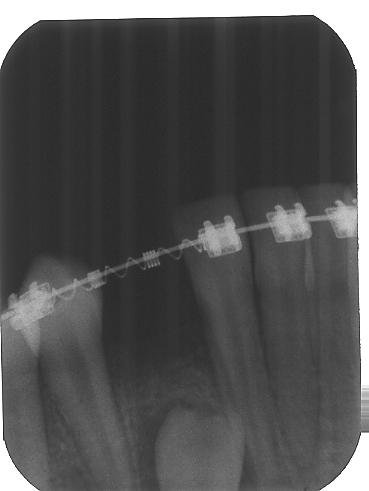
Sam had the surgery, "expose & bond", (10/07/11), see below::
A 'button' was put on the canines, a gold chain attached. His lower molar on the left side was helped by opening up the bone cover on top of it.
The surgeon did not comment on the 'wiggle test', i.e. whether you are able to gently luxate the impacted tooth; an indication that it is not ankylosed and thus gives you a chance to pull it in place. Unfortunately, at the time, I did not know enough to ask about 'the wiggle test' either. The surgeon did no comment on the resorption or that this should be cause for concern and if there was a need to check on the progression.
(Money aspect: $ 2 043)
Sam was referred to a periodontist for the exposing and bonding to get a chain on the canines.
(Orthodontist # 1 said that he referred to a periodontist instead of an oral surgeon since it was less traumatic for the teeth and the patient, and no need for general anesthesia.) The periodontist said Sam's canines were out of her reach and Sam needed an oral surgeon.
The oral surgeon # 1 pointed out that Sam's right maxillary canine, #6, has an irregular outline of the crown, something Sam's dentist had also seen on x rays. No definite explanation for it. One theory was that the trauma to Sam's front teeth could have interfered with his unerupted permanent canines somehow.
Sam had the surgery, "expose & bond", (10/07/11), see below::
A 'button' was put on the canines, a gold chain attached. His lower molar on the left side was helped by opening up the bone cover on top of it.
The surgeon did not comment on the 'wiggle test', i.e. whether you are able to gently luxate the impacted tooth; an indication that it is not ankylosed and thus gives you a chance to pull it in place. Unfortunately, at the time, I did not know enough to ask about 'the wiggle test' either. The surgeon did no comment on the resorption or that this should be cause for concern and if there was a need to check on the progression.
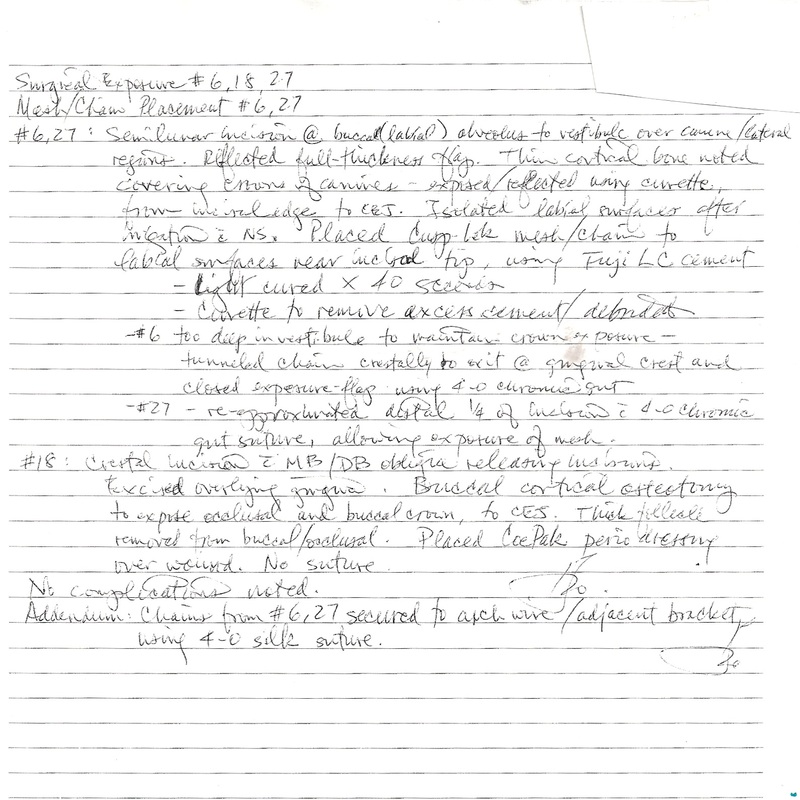
Information I asked for from surgeon #1 a year after his expose&bond #1:
The teeth were exposed by bone removal using curettes and a mesh/chain appliance was cemented with glass ionomer cement; no
etchant was involved as I prefer not to use caustic materials in exposures. By that token, calcium hydroxide is extremely caustic
and without suspecting the rare occurrence of pre-eruptive intracoronal resorption, its use was not considered.
curettes were used to uncover the teeth. At no time were burs or other rotary instruments used since, yes, mechanical or heat damage to
the teeth could occur. (This does not mean that I don’t use burs when necessary; but not in Sam’s case. I also use a piezo surgical
instrument when appropriate; its ultrasonic resonance under constant irrigation has been shown to be much less traumatic.) As a matter of
routine, once I expose the crown, I do give it a slight “nudge” with the curette to check mobility. Because there was no apparent sign of
ankylosis, this was not written down. I must admit that this should have been noted, as much as a positive lack of mobility is always noted.
Orthodontist # 1 gives up: March 2012
After 6 months of traction, and visits every two weeks, orthodontist #2 takes the panorama below.
He concludes the canines had not moved, but the rest of the teeth were getting misaligned according to the orthodontist from the effort.
Sam's orthodontist gave up and pulled the plug, or rather, cut the gold chains...The orthodontist sent us off with a referral for "extraction" to oral surgeon #1; no other option possible according to the orthodontist. He also told the oral surgeon to 'educate us about dental implants'. He didn't bother mentioning you don't put implants in 14-year-olds.
After 6 months of traction, and visits every two weeks, orthodontist #2 takes the panorama below.
He concludes the canines had not moved, but the rest of the teeth were getting misaligned according to the orthodontist from the effort.
Sam's orthodontist gave up and pulled the plug, or rather, cut the gold chains...The orthodontist sent us off with a referral for "extraction" to oral surgeon #1; no other option possible according to the orthodontist. He also told the oral surgeon to 'educate us about dental implants'. He didn't bother mentioning you don't put implants in 14-year-olds.
Research and finding Dr. Becker
We got cold feet (imminent extraction of permanent teeth does that to you) and started our web investigation of impacted canines. I found Dr. Becker, a leading expert, and in a nothing-to-loose impulse sent him an email. Dr Becker responded, from Jerusalem, within hours and his response helped convince me that we were not yet ready to give up Sam's canines for extraction.
(The letter below is me in blue, orthodontist #1 in black and Dr. Becker red.)
Our orthodontist accounts the failure of my son's traction to:
The factors that must be considered when determining probability of successful treatment of impacted canines are:
1. location of the canine, i.e., how far away the canine is from its ideal position and angulation of the canine
While distance is certainly a factor in the success of the treatment, distance is not, by itself, a reason for total non-movement. Evidence of movement should still be seen...... and presumably the treatment was attempted ab initio because the location was not deemed to be extraordinary at the outset. (Becker A. Extreme tooth impaction and its resolution. Seminars in Orthodontics, 2010, 16:222-233.)
2. age of the patient, i.e., the older the patient, the longer the canine has been in its present location, and the older the patient, the more mature the canine development is.
14 years of age is not "old" in the present context and active traction of a completely developed canine root should not be a contraindication for attempting the treatment. (Becker A, Chaushu S. Success rate and duration of orthodontic treatment for adult patients with palatally impacted maxillary canines. American Journal of Orthodontics and Dentofacial Orthopedics. 2003; 124:509-514)
3. root formation, i.e., the percentage of root development. The closer to 100% root formation, the more challenging the eruption.
This is true to a degree when considering normal unaided eruption of the tooth, but not when it comes to active appliance-generated encouraged eruption. If this were true, then we would not undertake to treat any impacted canine over the age of 14 years.
In your study the patients were 17.4 years +/- 4.3, but you do not mention anything about degree of root formation and if a 100 % root formation would make any attempt to move the tooth, and have it viable, impossible. Is it? Absolutely no.
My son, who is 14, with one impacted maxillary and one mandibular canine (and root resorption of the incisor) (Becker A, Chaushu S. Long-term follow-up of severely resorbed maxillary incisors following resolution of etiologically-associated canine impaction. American Journal of Orthodontics and Dentofacial Orthopedics. 2005, 127:650-654), is recommended extraction of these teeth.
He has been seen by dentists, orthodontists and an oral surgeon throughout his life here in the Bay Area and as parents we have tried finding the best advice, so it is very sad to us, that our current orthodontist says we basically came too late, and since the teeth haven't moved after 6 months of traction they have to be removed.
There are other reasons for failure, as we pointed out in that article and there is new evidence since the article was written, which I shall be presenting at the Hawaii meeting of the American Association of Orthodontists in a couple of weeks time. An account of this is available in both the second (2007) and now third (2012) editions of my textbook entitled "The Orthodontic Treatment of Impacted Teeth", published by Wiley Blackwell.
We have an appointment with the oral surgeon who attached the chains to his canines, but if there is someone of your caliber around here we would like to see him/her for a second opinion. With the benefits of internet, you can now seek advice from half way around the world!