IMPLANTS, EXTRACTIONS, BONE GRAFTS AND THE ALVEOLAR RIDGE
"What do you have against implants? "
If you are missing a tooth, certainly implants are a true blessing and important for quality of life and oral health*. You have no choice, and the ads with before and after pictures of people starting with truly awful tooth problems, displaying perfect smiles with implants, are very convincing. Looking around the private practice websites it looks like implants are the darling of dentists, orthodontist and oral surgeons alike; everybody's doing it.
An orthodontist asked me, when told we were off to Jerusalem,"What do you have against implants?" First most it's a gut feeling, but I found this scientific paper, with an author I now recognize well, Dr. Kokich, whom I will let speak for me:
Implants have become an important part of restorative dentistry for patients who are congenitally missing
teeth as well as those patients where teeth were extracted due to extensive caries, trauma, or periodontal
diseases. If all members of the team participate correctly, the result can be outstanding. However,
if the team of surgeon, orthodontists, and restorative dentists do not coordinate their efforts
properly, the result could be disastrous.(4)
As with the 'expose & bond' it is teamwork and diagnosis and planning that make it work...or not.
An orthodontist asked me, when told we were off to Jerusalem,"What do you have against implants?" First most it's a gut feeling, but I found this scientific paper, with an author I now recognize well, Dr. Kokich, whom I will let speak for me:
Implants have become an important part of restorative dentistry for patients who are congenitally missing
teeth as well as those patients where teeth were extracted due to extensive caries, trauma, or periodontal
diseases. If all members of the team participate correctly, the result can be outstanding. However,
if the team of surgeon, orthodontists, and restorative dentists do not coordinate their efforts
properly, the result could be disastrous.(4)
As with the 'expose & bond' it is teamwork and diagnosis and planning that make it work...or not.
Quote above is from the abstract, since I do not have full access, but a review of the study can be found in medscape:
(http://www.medscape.com/viewarticle/811905) and I think the two frustrated comments below by two practioners say more than most studies:
Having removed 3 implants and treated 4 others for progressive bone loss in the last week I whole heartedly
agree. The implant industry seduced the profession by quoting very high success rates while keeping hidden
that these rates were produced by the best surgeons and restorative dentists under ideal conditions. This is
not translatable to the real world where, by definition, the majority of us are C students busy running full
time multi-modality offices.
Make no mistake, i love implant dentistry. It has often gotten me out of a jam where no other options
existed. Yet it is no panacea. Today there appears to be a race as to who can get the most titanium in th
shortest amount of time. I recently consulted on a case regarding an 80-year-old female, who had a bridge
of 50 years fail due to a small enamel fracture. The first option given the patient was to place an implant.
It never entered the practitioners mind that contraindications existed such as; patient had been on injectable
Bis-phosphonate therapy for 10 years, was currently in active treatment for thyroid cancer, and the fact that
the bridge was easily replaceable with minimal additional treatment.
Proceeding with an implant was a disaster waiting to occur in this patient. As a profession, we have been
fortunate that the malpractice lawyers have not found it fertile to prosecute cases involving dental implants.
This will change in the future and we will only have ourselves to blame for it. (Scott Manhart Oct 1, 2013)
Dr. Manhart is right on point, particularly with his observations relative to C students running
multimodality offices. Having worked closely with a team involved in implant research in implant [science pre-
Branemark] some 35 years ago I reflect on their intentions that implant prosthodontics was intended to be a
independent surgical/prosthetic discpline, a specialty unto itself, with a postdoctoral training program not
unlike oral/maxillofacial surgery in scope. IMHO both the implant industry and the ADA joined forces to
assure that anyone and his mother who could execute a modified pen grasp would be a provider. Now
retired to Florida, I have been told that, in this state, implant cases rank first in the medical malpractice
folios of personal injury litigations. The wrong provider, treating the wrong patient, at the wrong time.
(Arnold Rosenstock Oct 9, 2013)
(http://www.medscape.com/viewarticle/811905) and I think the two frustrated comments below by two practioners say more than most studies:
Having removed 3 implants and treated 4 others for progressive bone loss in the last week I whole heartedly
agree. The implant industry seduced the profession by quoting very high success rates while keeping hidden
that these rates were produced by the best surgeons and restorative dentists under ideal conditions. This is
not translatable to the real world where, by definition, the majority of us are C students busy running full
time multi-modality offices.
Make no mistake, i love implant dentistry. It has often gotten me out of a jam where no other options
existed. Yet it is no panacea. Today there appears to be a race as to who can get the most titanium in th
shortest amount of time. I recently consulted on a case regarding an 80-year-old female, who had a bridge
of 50 years fail due to a small enamel fracture. The first option given the patient was to place an implant.
It never entered the practitioners mind that contraindications existed such as; patient had been on injectable
Bis-phosphonate therapy for 10 years, was currently in active treatment for thyroid cancer, and the fact that
the bridge was easily replaceable with minimal additional treatment.
Proceeding with an implant was a disaster waiting to occur in this patient. As a profession, we have been
fortunate that the malpractice lawyers have not found it fertile to prosecute cases involving dental implants.
This will change in the future and we will only have ourselves to blame for it. (Scott Manhart Oct 1, 2013)
Dr. Manhart is right on point, particularly with his observations relative to C students running
multimodality offices. Having worked closely with a team involved in implant research in implant [science pre-
Branemark] some 35 years ago I reflect on their intentions that implant prosthodontics was intended to be a
independent surgical/prosthetic discpline, a specialty unto itself, with a postdoctoral training program not
unlike oral/maxillofacial surgery in scope. IMHO both the implant industry and the ADA joined forces to
assure that anyone and his mother who could execute a modified pen grasp would be a provider. Now
retired to Florida, I have been told that, in this state, implant cases rank first in the medical malpractice
folios of personal injury litigations. The wrong provider, treating the wrong patient, at the wrong time.
(Arnold Rosenstock Oct 9, 2013)

April 9, 2015. it makes at least me worried when an implant advertisement looks like a used car ad.
|
SF chronicle April 5, 2015.
So what is a fair price for an implant?
What's a quality implant and who is a quality implant surgeon?
|
Implants in growing teens
I looked at an informal chat on osseonews.com discussing what to do with a 14-year-old boy who lost all 4 maxillary incisors in a car accident, Implants in Young Patient: Will this prevent full growth of the maxilla?'. Could he get implants at 14? Another concerning implants in a 16-year-old girl. The comments (from 2007) ranged from 'sure' to 'it would be a disaster', total lack of consensus and not very confidence inspiring. Here are some of the arguments:
The worst case (and very likely) scenario is that the implants will integrate beautifully, then submerge relative
to the rest of the alveolus and adjacent teeth. If the patient has a high smile line, he could be permanently
disfigured.
Wow, i don't see any problems with placing dental implants for a 14 y old. The smile line is well established
and facial muscles and pre maxilla is fully developed. The alveolus doesn't grow down if the opposing
dentiotion is stable. Two implants at lateral incisors and then cantilever brige (lat incisor and central) on each
side would solve the problem even if there is hypothetical growth disfiguring the patient. Nothing in literature
that supports contraindication of placing and restoring implants in 14 y old patients. Clue is Research done with
governance.
No implant should be placed before its time and even 18 years old male might well be too young. Placing it
now may turn out to be a disaster.
The use of wrist films is only a rough guide, and they do not necessarily coincidfe with the growth of the
maxilla. The wrist bones are endochondral, while the bones of the skull (maxilla) are intramembranous in
origin. Their growth periods do not necessarily coincide. Placing implants in too young a patient willo result in
them being too apical and palatal as the patient's skull matures and ages.
Well, apparently there is no research and data that has been collected to really answer what is the best course of action. I did learn that there is something called 'transitional implant' or 'mini implant' that would be a middle way. Another 'thread' on the same forum with a dentist planning extraction of an impacted canine and implants resulted in this answer:
Let's be honest here! If you were having surgery on a very COMPLICATED AREA and your doc had to ask in a
forum "what should I do?" Would you want to have that procedure done by that doc?
This is not reassuring reading!
The worst case (and very likely) scenario is that the implants will integrate beautifully, then submerge relative
to the rest of the alveolus and adjacent teeth. If the patient has a high smile line, he could be permanently
disfigured.
Wow, i don't see any problems with placing dental implants for a 14 y old. The smile line is well established
and facial muscles and pre maxilla is fully developed. The alveolus doesn't grow down if the opposing
dentiotion is stable. Two implants at lateral incisors and then cantilever brige (lat incisor and central) on each
side would solve the problem even if there is hypothetical growth disfiguring the patient. Nothing in literature
that supports contraindication of placing and restoring implants in 14 y old patients. Clue is Research done with
governance.
No implant should be placed before its time and even 18 years old male might well be too young. Placing it
now may turn out to be a disaster.
The use of wrist films is only a rough guide, and they do not necessarily coincidfe with the growth of the
maxilla. The wrist bones are endochondral, while the bones of the skull (maxilla) are intramembranous in
origin. Their growth periods do not necessarily coincide. Placing implants in too young a patient willo result in
them being too apical and palatal as the patient's skull matures and ages.
Well, apparently there is no research and data that has been collected to really answer what is the best course of action. I did learn that there is something called 'transitional implant' or 'mini implant' that would be a middle way. Another 'thread' on the same forum with a dentist planning extraction of an impacted canine and implants resulted in this answer:
Let's be honest here! If you were having surgery on a very COMPLICATED AREA and your doc had to ask in a
forum "what should I do?" Would you want to have that procedure done by that doc?
This is not reassuring reading!
Dr Kokich article (4) also writes about when to determine the right time for implants:
The age for implant placement in adolescent males and females is completely dependent on the completion
of facial growth. As the mandibular ramus contimues to grow, the posterior teeth erupt. If an implant is
placed to early, before growth is completed, it will mimic an ankylosed tooth and become submerged in the
alveolus. This could cause a periodontal defect between the implant and the adjacent teeth, if the defect is
severe enough. The most precise method for determining if facial or ramal growth is completed is to
superimpose seqential cephalometric radiographs.If growth is continuing, the distance between nasion and
menton will continue to increase indicating that it is to early to place the implant. The implant should not be
placed until there is no change in facial vertical dimension taken on two headfilms one year apart...In
general, implants should not be placed in boys until after 21 years of age, and in females after 17 years.
The age for implant placement in adolescent males and females is completely dependent on the completion
of facial growth. As the mandibular ramus contimues to grow, the posterior teeth erupt. If an implant is
placed to early, before growth is completed, it will mimic an ankylosed tooth and become submerged in the
alveolus. This could cause a periodontal defect between the implant and the adjacent teeth, if the defect is
severe enough. The most precise method for determining if facial or ramal growth is completed is to
superimpose seqential cephalometric radiographs.If growth is continuing, the distance between nasion and
menton will continue to increase indicating that it is to early to place the implant. The implant should not be
placed until there is no change in facial vertical dimension taken on two headfilms one year apart...In
general, implants should not be placed in boys until after 21 years of age, and in females after 17 years.
Determining the cessation of vertical growth of the craniofacial structures to facilitate placement of single-tooth implants by Fudalej P, Kokich VG, Leroux B.(http://www.ncbi.nlm.nih.gov/pubmed/17448387) concludes that the growth of the facial skeleton continues after puberty, but the amount of growth decreases steadily and after the second decade of life seems to be clinically insignificant.
|
You can determine if the skull, mandible, maxill, and everything is done growing by superimposing cefalograms made with 6 months intervall. Image and text borrowed from: http://www.dentistrytoday.com/orthodontics/1564 But there seems to be a caveat to this too. There can be a temporary stop in growth, that is then followed by a growth spurt... |

Figure 9. Patient in Figures 5 and 6. Superimposed cephalometric tracings demonstrating no change in vertical growth from 7/9/99 (black) to 6/6/00 (red). An implant can now be sucessfully placed.
|
An article entitled 'Age as compromising factor for implant insertion' (5) talks of how the maxilla and mandibel grows and the continuous bone remodeling that you have to be aware of when placing an implant. For example
1. Teeth have a natural 'mesial drift'. An implant doesn't move and could cause assymetries with the opposite side of the arch.
2. Between 9 and 25 years of age, the maxillary incisor will move 6 mm downward and 2.5 mm buccally.
3. Different facial types have different ways of growing.
4. Chronological age isn't a sufficient criteria.
More reliable standards are
a. superimposing tracings of serial cephalometric radiographs taken at least 6 months apart
b. follow-up of growth in length during at least 2 year (waiting for a growth below 0.5 cm/year
c. the change in dental position= eruption of the second molar
d. an evaluation of the skeletal age + radiograph of wrist of least used hand
It is advisable to determine growth cessation through a combination of methods.
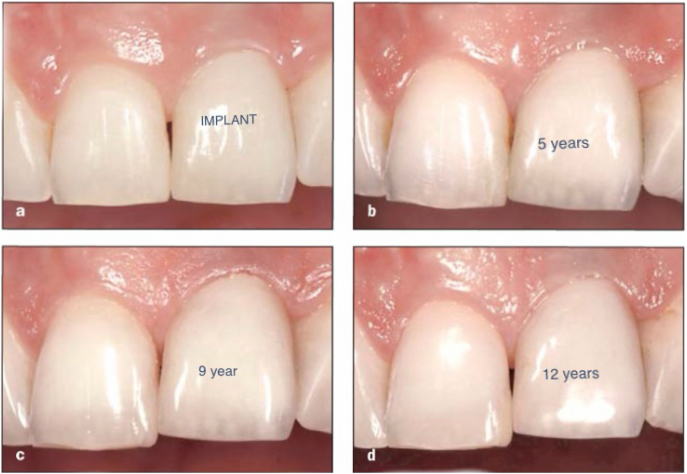
'Facial Development, Continuous Tooth Eruption, and Mesial DRift as Compromising Factors for Implant Placement' (6) has photos of what happens when the implant acts like an impacted (stuck tooth while the rest of the teeth are erupting and moving. It's very unfortunate for the front teeth, even millimeters of differences stand out when dealing with the 'social six'.
1. Teeth have a natural 'mesial drift'. An implant doesn't move and could cause assymetries with the opposite side of the arch.
2. Between 9 and 25 years of age, the maxillary incisor will move 6 mm downward and 2.5 mm buccally.
3. Different facial types have different ways of growing.
4. Chronological age isn't a sufficient criteria.
More reliable standards are
a. superimposing tracings of serial cephalometric radiographs taken at least 6 months apart
b. follow-up of growth in length during at least 2 year (waiting for a growth below 0.5 cm/year
c. the change in dental position= eruption of the second molar
d. an evaluation of the skeletal age + radiograph of wrist of least used hand
It is advisable to determine growth cessation through a combination of methods.
'Facial Development, Continuous Tooth Eruption, and Mesial DRift as Compromising Factors for Implant Placement' (6) has photos of what happens when the implant acts like an impacted (stuck tooth while the rest of the teeth are erupting and moving. It's very unfortunate for the front teeth, even millimeters of differences stand out when dealing with the 'social six'.
|
Photos from (6)
The implant gets osseointergrated/submerged as the neighboring teeth continues to develop and move. |
The jaw develops in 3 D= transversal, sagittal and coronal. 'The growth of the mandibel is closely associated with growth in stature, whereas growth of the maxilla is more associated with growth of the cranial structures' (p 870, (6)).
Maxillary growth
After the age of 7 years, the majority of change s that occur in the maxilla are the result of remodeling.
....
transverse growth implications:...The midpalatal suture usually closes after puberty, around the age of 15 (but
with large variation from 15 to 27 years). Thus the placement of a midpalatal implant as anchorage for
orthodontic appliances can be planned for patients who are at least 15 years old.
sagital growth implications: Resorption in hte anterior part of the maxilla could result in the gradual loss of
bone on the labial side of an implant. In a case report that described the treatment of a 13-year-old boy and
an 11.5-year-old girl, problems with labial fenestrations were noted as early as 1 months after placement in
the girl and 19 months in the boy. The problems increased in severity with growth.
Vertical Growth. Growth of the maxilla in a vertical direction occurs via displacement(sutural growth),
remodeling, and continued eruption. The maxilla is displaced downward, away from the cranium, by growth in
the orbits and in increases in the sizes of the nasal cavity ad maxillary sinuses...Usually adult levels of vertical
growth are reached at 17 or 18 for girls and somewhat later for boys.
vertical growth implications: To prevent complications in the vertical plane (especially related to remodeling),
it may be advisable to delay implant placement until the age of 18 years.
Mandibular Growth
The timing of mandibular growth is similar but not identical tto that of the maxilla. The mandible grows more
in a saggital plane than the maxilla during adolescence. This "differential jaw growth" converts the more
convex child profile to the straighter adult profile. In girls, mandibular growth is nearly completed 2 to 3 years
after menarche (usually at age 14 or 15), while for bos, growth can continue into the early 20s but
usually adult levels by age 18.
In females, the age at which growth of the facial skeleton ceases vertical development is shortly after 17
years of age on average. The vertical changes from nasion to menton ceases at slightly more than 20 years of
age on average in males. However, these are averages, and large deviations were observed. The clinican must
use superimposed cephalometric radiographs to accurately assess the cessation of vertical growth for each
specific patient.
Maxillary growth
After the age of 7 years, the majority of change s that occur in the maxilla are the result of remodeling.
....
transverse growth implications:...The midpalatal suture usually closes after puberty, around the age of 15 (but
with large variation from 15 to 27 years). Thus the placement of a midpalatal implant as anchorage for
orthodontic appliances can be planned for patients who are at least 15 years old.
sagital growth implications: Resorption in hte anterior part of the maxilla could result in the gradual loss of
bone on the labial side of an implant. In a case report that described the treatment of a 13-year-old boy and
an 11.5-year-old girl, problems with labial fenestrations were noted as early as 1 months after placement in
the girl and 19 months in the boy. The problems increased in severity with growth.
Vertical Growth. Growth of the maxilla in a vertical direction occurs via displacement(sutural growth),
remodeling, and continued eruption. The maxilla is displaced downward, away from the cranium, by growth in
the orbits and in increases in the sizes of the nasal cavity ad maxillary sinuses...Usually adult levels of vertical
growth are reached at 17 or 18 for girls and somewhat later for boys.
vertical growth implications: To prevent complications in the vertical plane (especially related to remodeling),
it may be advisable to delay implant placement until the age of 18 years.
Mandibular Growth
The timing of mandibular growth is similar but not identical tto that of the maxilla. The mandible grows more
in a saggital plane than the maxilla during adolescence. This "differential jaw growth" converts the more
convex child profile to the straighter adult profile. In girls, mandibular growth is nearly completed 2 to 3 years
after menarche (usually at age 14 or 15), while for bos, growth can continue into the early 20s but
usually adult levels by age 18.
In females, the age at which growth of the facial skeleton ceases vertical development is shortly after 17
years of age on average. The vertical changes from nasion to menton ceases at slightly more than 20 years of
age on average in males. However, these are averages, and large deviations were observed. The clinican must
use superimposed cephalometric radiographs to accurately assess the cessation of vertical growth for each
specific patient.
In the winter 2014 PSCO Bulletin it is mentioned how using CBCT images and '3D Superimposition Techniques' the digital imaging can be translated into 'polygon data' and used to assess growth (Tai K, Park JH. Superimposition of 3-dimensional CBCT for 2-dimensional image analysis. In: Computed Tomography: New Research. Hauppage, NY: Nova Science Publishers, Inc., 2013:457-475).
So the implant can end up not aligned with the rest of the teeth as the jaw continues to grow, I've also seen comments to the effect that the implant can stop the growth of the bone locally. This sound a bit like a chicken and egg dilemma and I've been looking for a source that can explain this more.
Thankfully research is ongoing. An Israeli company, Magdent, is trying to improve healing and anchorage of implant with 'a pulsed electromagnetic field', they published a study on rabbits in 2016
Thankfully research is ongoing. An Israeli company, Magdent, is trying to improve healing and anchorage of implant with 'a pulsed electromagnetic field', they published a study on rabbits in 2016
Mini implants
This turned out to be a red herring, when I looked into it further. Looking at realself.com with comments over five years, widely differing, it sounds like they are not viable as a replacement for teeth that are subject to heavy force, such as canines, and in the end doesn't hold any real advantage other than that they are cheaper.
This turned out to be a red herring, when I looked into it further. Looking at realself.com with comments over five years, widely differing, it sounds like they are not viable as a replacement for teeth that are subject to heavy force, such as canines, and in the end doesn't hold any real advantage other than that they are cheaper.
|
Immediate implants
Looking around for PEIR, I found this article in dentalaegis.com (not a scientific paper, more a dental product paper): "Extraction of impacted canine with immediate implant placement". I thought it interesting that the impacted canine had coronal radiolucency. However, the article had no mention of PEIR, nor age of the patient. It's an impacted canine and 'grade 3 mobility' of the lateral incisor next to it. They are both extracted The article merrily goes on to describe how the implant is done, with emphasis on the 'immediate' implant placement. One can only hope that they had some reason for not choosing the longer, but in the end more satisfactory solution of trying to extrude the canine, but the way it is written, it sounds like they couldn't wait to explore this new technique, which makes it very scary to me. Did they loose sight of the patient in their eagerness of writing a paper? Too bad that they did not make it a paper about PEIR instead, if indeed that was the diagnosis. (I did contact a coauthor, Dr Maurice Salama, who I understand is a renowned periodontist/orthodontist, but I did not hear back.)
In fact I think PEIR is out there, but, as in the article, ignored and undiagnosed, only the people aware of it can even see it. Implants for teens and the next 60, 70, 80 years
|
Looks like PEIR to me!
|
Implants have a 25 year history, which is not much when you think about putting them in a teen.
To solve an impacted canine with implants in children and youth, should only be the very last alternative, as far as I can judge at this point of my education in impacted canines. I can't say that it should be the first thing you do with an adult either.
In JADA Oct 1, 2013 there is a comparative study: 'Tooth preservation or implant placement - A systemic review of long-term tooth and implant survival rates' (3) concluding:
The results of this systematic review shows that implant survival rates do not exceed those of compromised
but adequately treated and maintained teeth, supporting the notion that the decision to extract a tooth and
place a dental implant should be made cautiously. Even when a tooth seems to be compromised and
requires treatment to be maintained, implant treatment also might require additional surgical procedures
that might pose some risks as well. Furthermore, a tooth can be extracted and replaced at any time;
however, extraction is a definitive and irreversible treatment.
'Long-term implant survival and success: a 10-16-year follow-up of non-submerged dental implants" (1) showed:
Results: The long-term implant cumulative survival rate up to 16 years was 82.94%. The prevalence of
biological complications was 16.94% and the prrevalence of technical complications was 31.09%. The
cumulative complication rate after an observation period of 10-16 years was 48.03%, which meant that
substantial amounts of chair time were necessary following implant placement. The majority of implant
losses and biological complications were concentrated in a relatively small number of patients
Conclusion: Despite a relatively high long-term survival rate, biological and technical complications were
frequent. Patients witth a history of periodontitis may have lower implant survival rates than patiens without
a history of periodontitis and were more prone to biological complications such as peri-implant mucositis and
peri-implantitis.
Endodontists, who are the ones doing root canals, are up in arms defending their turf, in this article: "New Research Shows Dental Implants Require Significantly More Follow-up that Root Canals"(2):
While the success of both procedures is similar, saving the natural tooth through a root canal rarely requires
follow-up treatment and generally lasts a lifetime; implants, on the other hand, have more postoperative
complications and higher long-term failure rates.
...
Because of the increasing popularity of dental implants, patients may not realize the long-term implications
of the procedure or that root canals may be healthier and less complicated in the long-run. Dental
professionals should ensure they explain to patients the difference between each procedure.
The option of extraction and implant may be presented as a solution, but hopefully patients are also informed that it isn't a matter of pulling out and putting in. When a tooth is stuck, the bone where all the teeth are
supposed to be anchored, is not developing normally. Extracting the tooth will stop the normal building up of bone, and instead cause a loss of bone. To make an implant stick there, usually needs to be preceeded by 'ridge augumentation' or bone grafts'. The problems associated with this are all the more prominent in children and youths where you don't yet have a fully developed jaw and teeth.
To extract an impacted canine will not only eliminate a tooth, it will also to cause resorption of the bone
of the alveolar ridge. When a tooth erupts it stimulates and preserves the alveolar ridge, without the tooth you
loose bone. If you are planning a future implant you need the bone to anchor screws into. In the absence of sufficient width and height of the bone, you are in for the added trouble of needing some sort of bone graft to
make it possible to fix the gap.
Bone grafts
The current materials for bone grafts are autografts (your own bone: the illiac crest, the tibia, or cranium as in chin or anterior mandibular ramus (coronoid process) or allografts (from another human),
xenograft (pig or cow bone) and different synthetic plastics. There are negative sides to all these alternatives,
and it is hard not to conclude that extraction & implant is not an easy alternative to trying to save a canine if
there is a way to do it.
It sounds like implants in teens can be summed up, changing the real estate axiom of 'location, location, location' to: 'timing, timing, timing'.
PRP = Platelet Rich Plasma, or PRGF = preparation rich in growth factors
Blood, 55 cc, is drawn from an IV, centrifuged to leave the platelets that is rich in growth factors to stimulate the stem cells at the location where they are put.
Not covered by insurance, you pay $400 (according to Dr Alberto's website).
Blood, 55 cc, is drawn from an IV, centrifuged to leave the platelets that is rich in growth factors to stimulate the stem cells at the location where they are put.
Not covered by insurance, you pay $400 (according to Dr Alberto's website).
Cost of implant
I found a useful 'yelp' on an oral surgeon in Mountain View that listed the costs involved:
- Consultation $ 127
- Panorex $ 154
- Extraction (#15) $ 391
- Grafting $ 1152
- PRGF $ 375
- implant $ 2539 (after 4 months)
- crown around $ 1000
So... $ 5,738 !!!
I found a useful 'yelp' on an oral surgeon in Mountain View that listed the costs involved:
- Consultation $ 127
- Panorex $ 154
- Extraction (#15) $ 391
- Grafting $ 1152
- PRGF $ 375
- implant $ 2539 (after 4 months)
- crown around $ 1000
So... $ 5,738 !!!
* I can take some national pride in this, since the first tooth implant in a patient was put in, 1965, by a Swedish orthopedic surgeon, Per-Ingvar Brånemark, at my alma mater, Göteborgs Universitet, Sweden.

|
Dr Brånemark, died at age 85, in 2014.The Brånemark Osseointegration Center was founded in 1989 in Gothenburg, Sweden.
|
(1) Simonis P, Dufour T, Tenenbaum H. Long-term implant survival and success: a 10-16-year follow-up of non-
submerged dental implants. Clin Oral Implants Res. 2010 Jul;21(7):772-7
(2) New Research Shows Dental Implants Require Significantly More Follow-Up Treatment Than Root Canals.
Website of the American Association of Endodontists: www.aae.org. 2008 article.
(3) Levin L, Halperin-Sternfeld M. Tooth preservation or implant placement - A systematic review of long-term
tooth and implant survival rates. JADA. Oct 1, 2013) 144, 1119-1133.
(4) Single-tooth implants and the adolescent orthodontic patient.
(5) Heij et al. Age as compromising factor for implant insertion. Periodontology, Vol.33, 2003, 172-184.
(6) Danny G. Op Heij et al. Facial Development, Continuous Tooth Eruption and Mesial Drift as Compromising
Factors for Implant Placement. Int J. Oral Maxillofacial Implants 2006;21:867-878
(7) Barak S. et al. A new device for improving dental implant anchorage: a histological and micro-computed
tomography study in the rabbit. Clin. Oral Impl. Res 27,2016,935-942. doi:10.1111/clr.12661.
submerged dental implants. Clin Oral Implants Res. 2010 Jul;21(7):772-7
(2) New Research Shows Dental Implants Require Significantly More Follow-Up Treatment Than Root Canals.
Website of the American Association of Endodontists: www.aae.org. 2008 article.
(3) Levin L, Halperin-Sternfeld M. Tooth preservation or implant placement - A systematic review of long-term
tooth and implant survival rates. JADA. Oct 1, 2013) 144, 1119-1133.
(4) Single-tooth implants and the adolescent orthodontic patient.
(5) Heij et al. Age as compromising factor for implant insertion. Periodontology, Vol.33, 2003, 172-184.
(6) Danny G. Op Heij et al. Facial Development, Continuous Tooth Eruption and Mesial Drift as Compromising
Factors for Implant Placement. Int J. Oral Maxillofacial Implants 2006;21:867-878
(7) Barak S. et al. A new device for improving dental implant anchorage: a histological and micro-computed
tomography study in the rabbit. Clin. Oral Impl. Res 27,2016,935-942. doi:10.1111/clr.12661.