THIRD MOLAR EXTRACTIONS and oral surgeons
A New York Times article in 2011 entitled 'The Wisdom of Having that Tooth Removed' described the US ritual of having third molars extracted before going to college. The article cites a 2010 press release by the AAOMF: 'Conventional Wisdom about Wisdom Teeth Confirmed -Evidence Shows Keeping Wisdom Teeth Might be More Harmful Than Previously Thought' where it states that "80% of young adult subjects who retained previously healthy wisdom teeth had developed problems within seven years", "retaining wisdom teeth can increase the risk
for broader conditions including preterm birth and cardiovascular disease".
The New York Times article author asked the contact person for the press release about the origin of the 80% figure and the answer was "We were not able to locate the reference for it, and subsequently deleted the statement from our website", quite a shocking statement if you are trying to put your confidence in doctors and science.
The OOMFS web page on wisdom teeth warns: "The worst thing you can do is to IGNORE your wisdom teeth". The webpage says if that a wisdom tooth can stay "if they grow in completely, are functional, painless, cavity-free, disease-free and in a hygenic environment with healthy gum tissue". It goes on to say that " When a tooth doesn't fully grow in, it's "impacted" -usually unable to break through the gums because there isn't enough room. 90 % of people have at least one impacted wisdom tooth."
It is reasonable to infer that the official OMFS information is saying that all the impacted wisdom teeth
need to go. And if you get to the surgeon at age 18 chances are that the wisdom tooth hasn't had the chance to erupt yet, ergo 'impacted', ergo it's got to go. And you can't just remove one.
Looking up the Swedish official recommendations on wisdom teeth (www.1177.se) the information you get is (my translation) :
Previously the tooth was always removed. During a period the dentist thought that a wisdom tooth that had not erupted was diseased and needed treatment. Since the 1980s it is viewed differently, and now the the wisdom tooth is left alone if it is not expected to cause problems.
The Swedish website includes information on complications at extraction such as nerve damage and breaking the maxillary bone around the tooth in the upper jaw where the bone is thin. The OMFS website has no information on risks with surgery.
The most scathing criticism of the third molar extraction is Dr Jay Friedman* who in 2006 (accepted in 2007) wrote a piece in the American Journal of Public Health: The Prophylactic Extraction of Third Molars: A Public Health Hazard (5). If Dr Brånemark** is the God of oral surgeons, Dr Friedman is the AntiChrist. Dr Friedman refutes the usual arguments put forwad by oral surgeons to go ahead with the third molar extractions:
Myth Number 1 - Third Molars have a High Incidence of pathology
Not more than 12% of impacted teeth have associated pathology. This incidence is the same as for
appendicities (10%) and cholecystitis (12%), yet prophylactic appendictomies and cholecystectomies are not
the standard of care. Why then prophylactic third-molar extractions?
What about pericoronitis, the pain and infection of the gum tissue surrounding a partially erupted or erupted
third molar? Excluding the normal discomfort of teething as the tooth erupts, the incidence of inflammation
and infection of the gum tissue ranges from 6% to 10%. Adding an average 8% incidence of pericoronitis to
the 12% pathology brings the maximum pathology associated with the third molars to 20%. However, as ingle
episode of pericoronitis is not a reason to remove a third molar; this should be considered only if the problem
fails to respond to conservative treatment or recurs.
...
Myth Number 2 - Early Removal of Third Molars are Less Traumatic
...dry socket, secondary infection, and paresthesia are less likely to occur in persons aged 35 to 83 years than
in those aged 12 to 24
......
Myth Number 3 - Pressure of Erupting Third Molars Cause Crowding of Anterior Teeth
It is not possible for the third molara, which develop in the spongy interior cancellous tissue of bone with no
firm support, to push 14 other teeth with roots implanted vertically like the pegs of a picket fence so that the
incisors in the middle twist and overlap. Yet that is the reason often given for removal of the third molars,
even though studies have produced contrary evidence. Third molars do not possess sufficient force to move
other teeth. They cannot cause crowding and overlapping of the incisors, and any such association is not
causation.
......
Myth Number 4 - the Risk of Pathology in Impacted Third Molars Increase With Age
There is no evidence of a significant increase in third-molar pathology with age.
.....
Myth Number 5 - There is Little Risk of Harm in the Removal of Third Molars
...ignored is the risk of incidental injury such as broken jaws, fractured teeth, damage to the
temporomandibular joints, temporary and, especially, permanent paresthsia or dysthesia (numbness and
dysfunction of the lower lip and the tongue. Data on the number of fractured jaws and damaged teeth are
lacking
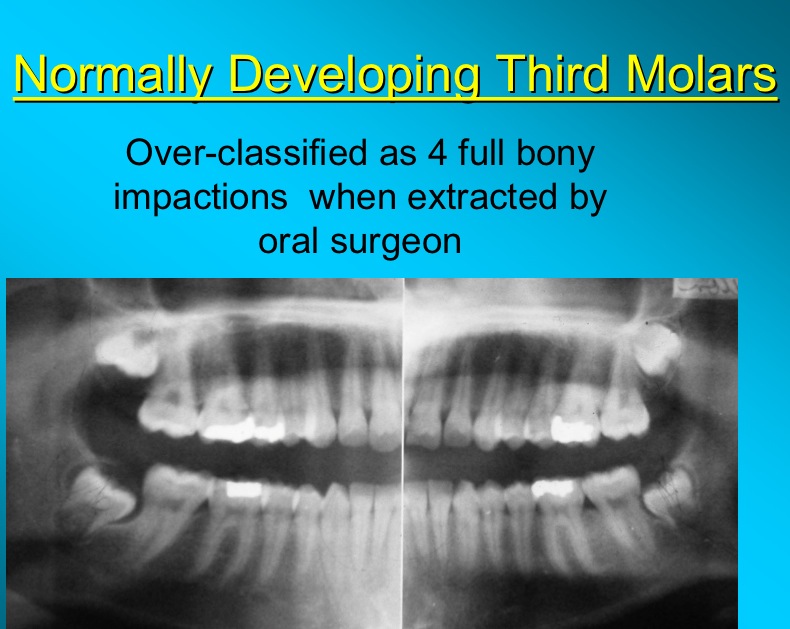
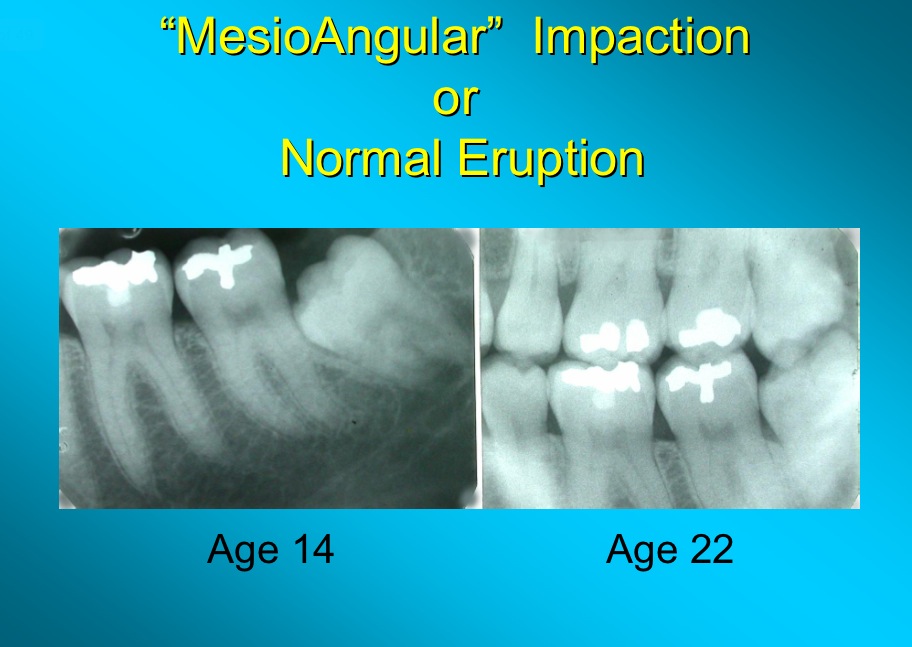
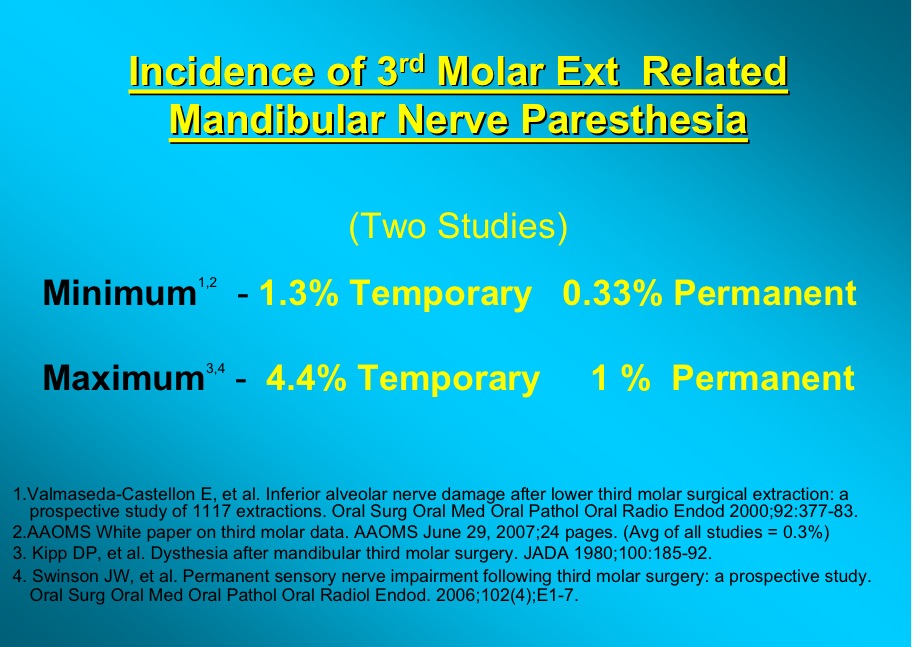
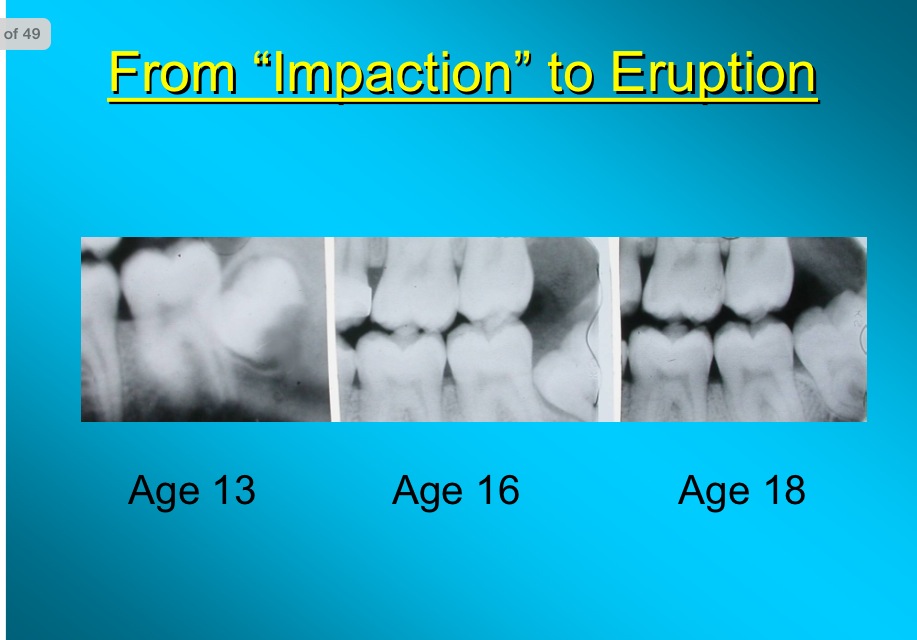
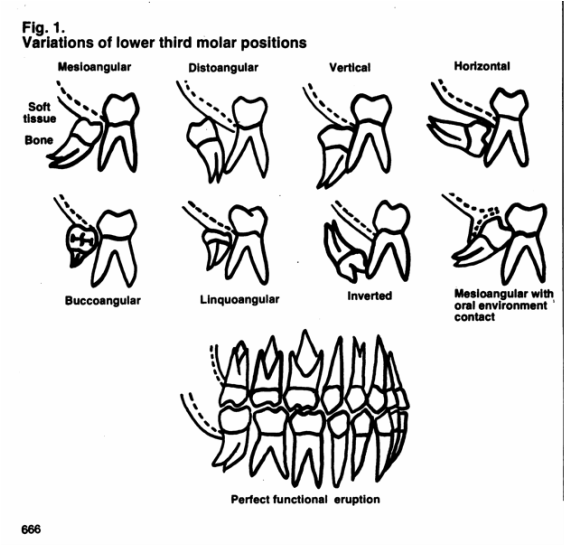
A powerpoint presentation by Dr Friedman from 2012 can be found on:
http://www.nationaloralhealthconference.com/docs/presentations/2012/05-02/Jay%20Friedman.pdf
It has images like this:
for broader conditions including preterm birth and cardiovascular disease".
The New York Times article author asked the contact person for the press release about the origin of the 80% figure and the answer was "We were not able to locate the reference for it, and subsequently deleted the statement from our website", quite a shocking statement if you are trying to put your confidence in doctors and science.
The OOMFS web page on wisdom teeth warns: "The worst thing you can do is to IGNORE your wisdom teeth". The webpage says if that a wisdom tooth can stay "if they grow in completely, are functional, painless, cavity-free, disease-free and in a hygenic environment with healthy gum tissue". It goes on to say that " When a tooth doesn't fully grow in, it's "impacted" -usually unable to break through the gums because there isn't enough room. 90 % of people have at least one impacted wisdom tooth."
It is reasonable to infer that the official OMFS information is saying that all the impacted wisdom teeth
need to go. And if you get to the surgeon at age 18 chances are that the wisdom tooth hasn't had the chance to erupt yet, ergo 'impacted', ergo it's got to go. And you can't just remove one.
Looking up the Swedish official recommendations on wisdom teeth (www.1177.se) the information you get is (my translation) :
Previously the tooth was always removed. During a period the dentist thought that a wisdom tooth that had not erupted was diseased and needed treatment. Since the 1980s it is viewed differently, and now the the wisdom tooth is left alone if it is not expected to cause problems.
The Swedish website includes information on complications at extraction such as nerve damage and breaking the maxillary bone around the tooth in the upper jaw where the bone is thin. The OMFS website has no information on risks with surgery.
The most scathing criticism of the third molar extraction is Dr Jay Friedman* who in 2006 (accepted in 2007) wrote a piece in the American Journal of Public Health: The Prophylactic Extraction of Third Molars: A Public Health Hazard (5). If Dr Brånemark** is the God of oral surgeons, Dr Friedman is the AntiChrist. Dr Friedman refutes the usual arguments put forwad by oral surgeons to go ahead with the third molar extractions:
Myth Number 1 - Third Molars have a High Incidence of pathology
Not more than 12% of impacted teeth have associated pathology. This incidence is the same as for
appendicities (10%) and cholecystitis (12%), yet prophylactic appendictomies and cholecystectomies are not
the standard of care. Why then prophylactic third-molar extractions?
What about pericoronitis, the pain and infection of the gum tissue surrounding a partially erupted or erupted
third molar? Excluding the normal discomfort of teething as the tooth erupts, the incidence of inflammation
and infection of the gum tissue ranges from 6% to 10%. Adding an average 8% incidence of pericoronitis to
the 12% pathology brings the maximum pathology associated with the third molars to 20%. However, as ingle
episode of pericoronitis is not a reason to remove a third molar; this should be considered only if the problem
fails to respond to conservative treatment or recurs.
...
Myth Number 2 - Early Removal of Third Molars are Less Traumatic
...dry socket, secondary infection, and paresthesia are less likely to occur in persons aged 35 to 83 years than
in those aged 12 to 24
......
Myth Number 3 - Pressure of Erupting Third Molars Cause Crowding of Anterior Teeth
It is not possible for the third molara, which develop in the spongy interior cancellous tissue of bone with no
firm support, to push 14 other teeth with roots implanted vertically like the pegs of a picket fence so that the
incisors in the middle twist and overlap. Yet that is the reason often given for removal of the third molars,
even though studies have produced contrary evidence. Third molars do not possess sufficient force to move
other teeth. They cannot cause crowding and overlapping of the incisors, and any such association is not
causation.
......
Myth Number 4 - the Risk of Pathology in Impacted Third Molars Increase With Age
There is no evidence of a significant increase in third-molar pathology with age.
.....
Myth Number 5 - There is Little Risk of Harm in the Removal of Third Molars
...ignored is the risk of incidental injury such as broken jaws, fractured teeth, damage to the
temporomandibular joints, temporary and, especially, permanent paresthsia or dysthesia (numbness and
dysfunction of the lower lip and the tongue. Data on the number of fractured jaws and damaged teeth are
lacking
A powerpoint presentation by Dr Friedman from 2012 can be found on:
http://www.nationaloralhealthconference.com/docs/presentations/2012/05-02/Jay%20Friedman.pdf
It has images like this:


Dr Friedman writes about the economic side of third molars, a 3 billion dollar affair:
Two thirds of all third-molar extractions are unnecessary. Eliminating these extractions would reduce the oral
and maxillofacial surgeons's annual income by $347 486 [from $518 636], resulting in an annual savings to
patients of more than $1.9 billion, or $ 2.2 billion if extractions by general practiononers are included.
Cochrane.org reviewed the literature and wrote about 'Surgical removal versus retention for the management of asymptomatic impacted wisdom teeth' in 2012. The conclusion was:
Insufficient evidence was found to support or refute routine prophylactic removal of asymptomatic impacted
wisdom teeth in adults. A single trial comparing removal versus retention found no evidence of a difference on
late lower incisor crowding at 5 years, however no other relevant outcomes were measured. Watchful
monitoring of aymptomatic third molar teeth may be a more prudent strategy.
This viewpoint was reflected in a Point/Counterpoint article by Dr Kandasamy (Dental School, University of Western Australia) in 2011:
Although indications for the removal of symptomatic third molars are well established, a convincing case for the routine removal of unerupeted asymptomatic, pathology-free third molars has not been made.(7)
In the 'Brazilian Oral Research' (4) from 2013 trying to answer whether there is justification for prophylactic extraction of third molars, looked at 260 randomized clinical trials, and found only four that were eligible, but even they were not very good quality or with a large enough sample size so that any conclusions could be made other than that there is a lack of scientific evidence to base extraction of third molars on.
The issue of third molars most have been ongoing for half a century, and there is still are no evidence based guidelines!
Dr Friedman also wrote an article in 1993: The standard of Care: An Ethical Responsibility of Public Health Dentistry (3)
Abstract
Wide variation in the diagnosis and treatment of dental problems is indicative of the lack of standard of care
to guide the practitioner and to protect the public. Examples of questionable dental practices are described to
illustrate how the public may be over treated, overcharged, and put at risk of iatrogen injury, practices that
are no longer valid in light of current knowledge of dental diseases and their treatment. Public health
dentistry traditionally concerns itself with community preventive, educational, and curative programs. It also
has the ethical responsibility -the moral duty and obligation - to recognize and contend with paternalistic
professional behavior that, intentionally or otherwise, violates the public trust, and to promote systems that
will improve access, quality, and financing of dentistry for everyone.
Two thirds of all third-molar extractions are unnecessary. Eliminating these extractions would reduce the oral
and maxillofacial surgeons's annual income by $347 486 [from $518 636], resulting in an annual savings to
patients of more than $1.9 billion, or $ 2.2 billion if extractions by general practiononers are included.
Cochrane.org reviewed the literature and wrote about 'Surgical removal versus retention for the management of asymptomatic impacted wisdom teeth' in 2012. The conclusion was:
Insufficient evidence was found to support or refute routine prophylactic removal of asymptomatic impacted
wisdom teeth in adults. A single trial comparing removal versus retention found no evidence of a difference on
late lower incisor crowding at 5 years, however no other relevant outcomes were measured. Watchful
monitoring of aymptomatic third molar teeth may be a more prudent strategy.
This viewpoint was reflected in a Point/Counterpoint article by Dr Kandasamy (Dental School, University of Western Australia) in 2011:
Although indications for the removal of symptomatic third molars are well established, a convincing case for the routine removal of unerupeted asymptomatic, pathology-free third molars has not been made.(7)
In the 'Brazilian Oral Research' (4) from 2013 trying to answer whether there is justification for prophylactic extraction of third molars, looked at 260 randomized clinical trials, and found only four that were eligible, but even they were not very good quality or with a large enough sample size so that any conclusions could be made other than that there is a lack of scientific evidence to base extraction of third molars on.
The issue of third molars most have been ongoing for half a century, and there is still are no evidence based guidelines!
Dr Friedman also wrote an article in 1993: The standard of Care: An Ethical Responsibility of Public Health Dentistry (3)
Abstract
Wide variation in the diagnosis and treatment of dental problems is indicative of the lack of standard of care
to guide the practitioner and to protect the public. Examples of questionable dental practices are described to
illustrate how the public may be over treated, overcharged, and put at risk of iatrogen injury, practices that
are no longer valid in light of current knowledge of dental diseases and their treatment. Public health
dentistry traditionally concerns itself with community preventive, educational, and curative programs. It also
has the ethical responsibility -the moral duty and obligation - to recognize and contend with paternalistic
professional behavior that, intentionally or otherwise, violates the public trust, and to promote systems that
will improve access, quality, and financing of dentistry for everyone.
From (8)
This is how a 'Brit' puts it in his humorous introduction to a more scientific expose.
It is perhaps, a reflection of our different health care systems that a "Brit" has been asked to write an
opposing view on the removal of symptomless third molars. Indeed , surveying American oral surgeons about
whether symptomless third molars should be removed would be as predictable as asking turkeys to vote for
Christmas. Such opinions are always going to be more heavily colored by a potential threat to livelihood than
by balanced reference to scientific research. This is neither surprising nor condemning; it is simply to state
the obvious and to request a fair hearing on the subject. Indeed after speaking in the United
States in 2004 on the controversies surrounding third molar removal in the United Kingdom, I began to
wonder if I should buy body armor before venturing over the pond again! (6)
(Unfortunately I'm unable to read the whole thing since these articles cost $ 36 if you don't have a subscription or are attached to some institution with access.) Dr Hill references NICE, National Institue for Health and Care Excellence in Great Britain. Their recommendation in 2000 was to not operate on wisdom teeth 'free from disease
(healthy)' (of course 'healthy' that might not be seen as a black and white issue) because
– There is no reliable research to suggest this benefits patients
– Patients who do have healthy wisdom teeth removed are being exposed to the risks of surgery. These can
include, nerve damage, damage to other teeth, infection, bleeding, and, rarely, death. Also, after surgery
to remove wisdom teeth, patients may have swelling, pain and be unable to open their mouth fully.
opposing view on the removal of symptomless third molars. Indeed , surveying American oral surgeons about
whether symptomless third molars should be removed would be as predictable as asking turkeys to vote for
Christmas. Such opinions are always going to be more heavily colored by a potential threat to livelihood than
by balanced reference to scientific research. This is neither surprising nor condemning; it is simply to state
the obvious and to request a fair hearing on the subject. Indeed after speaking in the United
States in 2004 on the controversies surrounding third molar removal in the United Kingdom, I began to
wonder if I should buy body armor before venturing over the pond again! (6)
(Unfortunately I'm unable to read the whole thing since these articles cost $ 36 if you don't have a subscription or are attached to some institution with access.) Dr Hill references NICE, National Institue for Health and Care Excellence in Great Britain. Their recommendation in 2000 was to not operate on wisdom teeth 'free from disease
(healthy)' (of course 'healthy' that might not be seen as a black and white issue) because
– There is no reliable research to suggest this benefits patients
– Patients who do have healthy wisdom teeth removed are being exposed to the risks of surgery. These can
include, nerve damage, damage to other teeth, infection, bleeding, and, rarely, death. Also, after surgery
to remove wisdom teeth, patients may have swelling, pain and be unable to open their mouth fully.
An extremely informative website on 'Wisdom teeth - Myths and realities' can be found at
www. orthodontisteenligne.com/en/dentition-en/wisdom-teeth-myths-and-realities/
It's the website of an orthodontist in Quebec. Dr Lemaystates (in red) that "Removing third molars will not prevent lower anterior dental crowding' which is something you will still hear in the US. Read this because information like this doesn't seem to be had in the US, for reasons stated above.
Another helpful website would be : www.animated-teeth.com/wisdom_teeth, but it says nothing about who is behind the website which is kind of disconcerting.
www. orthodontisteenligne.com/en/dentition-en/wisdom-teeth-myths-and-realities/
It's the website of an orthodontist in Quebec. Dr Lemaystates (in red) that "Removing third molars will not prevent lower anterior dental crowding' which is something you will still hear in the US. Read this because information like this doesn't seem to be had in the US, for reasons stated above.
Another helpful website would be : www.animated-teeth.com/wisdom_teeth, but it says nothing about who is behind the website which is kind of disconcerting.
* Dr Jay W Friedman was born in 1927, he is 88! He served as a researcher at the UCLA School of Public
Health and as a clinical professor at USC School of dentistry. In 1971 he published a 'Guide for the Evaluation
of Dental Care', and in 1991 'Complete Guide to Dental Health: How to Maintain Your Dental Health and
Avoid Being Overcharged and Overtreated' (revised and reissued in 2002). He first publized criticism of the
third molar extractions in 1977. I got the information from a you tube clip from 2013 where Dr Friedman
received the John W. Knutson Distinguished Service Award in Dental Public Health' in San Francisco 2012, at
the APHA Annual Meeting.
Health and as a clinical professor at USC School of dentistry. In 1971 he published a 'Guide for the Evaluation
of Dental Care', and in 1991 'Complete Guide to Dental Health: How to Maintain Your Dental Health and
Avoid Being Overcharged and Overtreated' (revised and reissued in 2002). He first publized criticism of the
third molar extractions in 1977. I got the information from a you tube clip from 2013 where Dr Friedman
received the John W. Knutson Distinguished Service Award in Dental Public Health' in San Francisco 2012, at
the APHA Annual Meeting.
** Per-Ingvar Brånemark, who died in December 2014 at age 85, is 'the father of modern dental implantology'.
'The Brånemark Osseointegration Center' is located where he worked, Göteborg, Sweden. Brånemark, a
Professor of Anatomy, did a study in 1952 using a titanium implant chamber to study blood
flow in rabbit bone. The titanium could not be removed after the experiment, it had integrated...In 1965 the
titanium was tried out in a patient. It held up and the patient died with it in place in 2002. Brånemark's
work lives on in the 'Nobel Biocare' implants. A conference in 1982 in Toronto spread the technique of
titanium implants to the rest of the world.
'The Brånemark Osseointegration Center' is located where he worked, Göteborg, Sweden. Brånemark, a
Professor of Anatomy, did a study in 1952 using a titanium implant chamber to study blood
flow in rabbit bone. The titanium could not be removed after the experiment, it had integrated...In 1965 the
titanium was tried out in a patient. It held up and the patient died with it in place in 2002. Brånemark's
work lives on in the 'Nobel Biocare' implants. A conference in 1982 in Toronto spread the technique of
titanium implants to the rest of the world.
Here's a link with more links: teethremoval.com
(1) http://www.ada.org/~/media/ADA/About%20the%20ADA/Files/code_of_ethics_2012.ashx
(2) Am J Orthod Dentofacial Orthop. 1999 Feb;115(2):220-2. Ethics case analysis: another doctor's
mistreatment. Litigation, legislation, and ethics.Chiodo G1, Tolle S, Jerrold L.
(3) Journal of Public Health Dentistry. Vol 53, Issue 3 pp 165-169, September 1993.
(4) 'Is there justification for prophylactic extraction of third molars? A systemic Review'
'http://www.ncbi.nlm.nih.gov/pubmed/23538430
(5) Jay W. Friedman. The Prophylactic Extraction of Third Molars: A Public Health Hazard. Am J Public Health.
2007 Sep; 97(9): 1554-1559.
doi: 10.2105/AJPH.2006.100271
(6) C Michael Hill (at the Department of Oral and Maxillofacial Surgery, the Dental Hospital in Cardiff, UK)
Removal of Aymptomatic
Third Molars: An Opposing View. J Oral Maxillofac Surg 64;1816-1820, 2006
(7) Sanjivan Kandasamy. Evaluation and management of asymptomatic third molars: Watchful monitoring is a
low-risk alternative to extraction. American Journal of Orthodontics and Dentofacial Orthopedics. July 2011,
Vol.140(1):11,13,15,17, doi:10.1016/j.ajodo.2011.05.008
(8) John E. Speck. The Wisdom Tooth.Can. Fam. Physician Vol. 27:April 1981.
(2) Am J Orthod Dentofacial Orthop. 1999 Feb;115(2):220-2. Ethics case analysis: another doctor's
mistreatment. Litigation, legislation, and ethics.Chiodo G1, Tolle S, Jerrold L.
(3) Journal of Public Health Dentistry. Vol 53, Issue 3 pp 165-169, September 1993.
(4) 'Is there justification for prophylactic extraction of third molars? A systemic Review'
'http://www.ncbi.nlm.nih.gov/pubmed/23538430
(5) Jay W. Friedman. The Prophylactic Extraction of Third Molars: A Public Health Hazard. Am J Public Health.
2007 Sep; 97(9): 1554-1559.
doi: 10.2105/AJPH.2006.100271
(6) C Michael Hill (at the Department of Oral and Maxillofacial Surgery, the Dental Hospital in Cardiff, UK)
Removal of Aymptomatic
Third Molars: An Opposing View. J Oral Maxillofac Surg 64;1816-1820, 2006
(7) Sanjivan Kandasamy. Evaluation and management of asymptomatic third molars: Watchful monitoring is a
low-risk alternative to extraction. American Journal of Orthodontics and Dentofacial Orthopedics. July 2011,
Vol.140(1):11,13,15,17, doi:10.1016/j.ajodo.2011.05.008
(8) John E. Speck. The Wisdom Tooth.Can. Fam. Physician Vol. 27:April 1981.