Part 3: Dr Becker and Jerusalem - March 2014
|

Hadassah Hebrew University, Ein Kerim, Jerusalem
|


'You're going where... doing what?!' was what people said when we told of our trip to Dr. Becker and Jerusalem.
You really need the full and very long version of Sam's orthodontic experience in the Bay Area to understand that this was a logical next step.
Dr. Becker advised against waiting for summer. You do not linger with resorption. We needed at least three weeks so Dr Becker could get the traction going. Dr Becker prepared by looking through all Sam's x-rays, including the two CBCTs. He also ordered complementary periapicals of the impacted canines to check for signs of ICRR, and a fresh panorama. Dr Zeltser, the surgeon, wanted a report from Sam's physician and some blood work.
At UCSF the surgeons said they could not reach the canines, could not do the glass ionomer filling, and also said
there was an infection risk. Dr Becker explained to Dr Nelson that ICRR and PEIR are not bacterial.
Dr Nelson agreed with Dr Becker's reasoning on recommended treatment, but ,illogically , would rather have Dr Hossaini extract the canines, if not he would end his treatment. With Dr Nelson's dismissal of Sam from treatment at UCSF, I had to try finding a local orthodontist to be orthodontist # 5 before the trip, not an easy thing.
Off we went.
You really need the full and very long version of Sam's orthodontic experience in the Bay Area to understand that this was a logical next step.
Dr. Becker advised against waiting for summer. You do not linger with resorption. We needed at least three weeks so Dr Becker could get the traction going. Dr Becker prepared by looking through all Sam's x-rays, including the two CBCTs. He also ordered complementary periapicals of the impacted canines to check for signs of ICRR, and a fresh panorama. Dr Zeltser, the surgeon, wanted a report from Sam's physician and some blood work.
At UCSF the surgeons said they could not reach the canines, could not do the glass ionomer filling, and also said
there was an infection risk. Dr Becker explained to Dr Nelson that ICRR and PEIR are not bacterial.
Dr Nelson agreed with Dr Becker's reasoning on recommended treatment, but ,illogically , would rather have Dr Hossaini extract the canines, if not he would end his treatment. With Dr Nelson's dismissal of Sam from treatment at UCSF, I had to try finding a local orthodontist to be orthodontist # 5 before the trip, not an easy thing.
Off we went.
Dr. Becker's advice for continued treatment:
...
The canine in the right side of both maxilla and mandible are impacted and have resisted every attempt to resolve them until the present time. Surgery and orthodontics have been performed more than once and by several people, to no avail. Dr. Bower is a very resourceful person and, from her internet searches, has maintained an e-mail correspondence with me over the past several months.
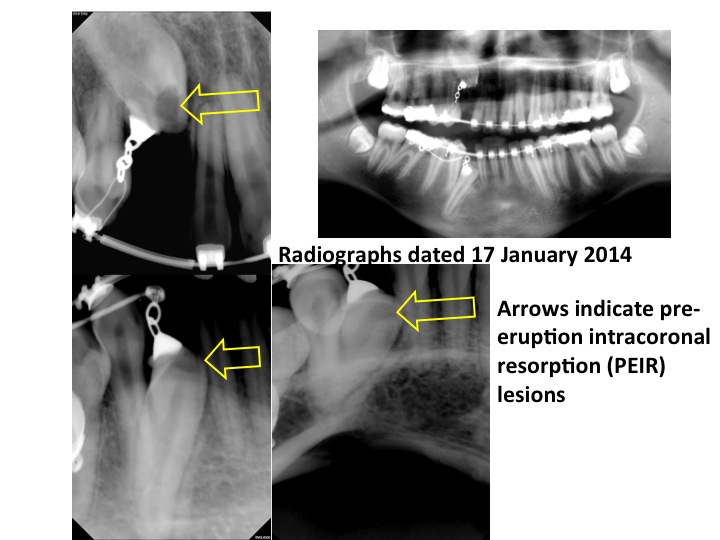
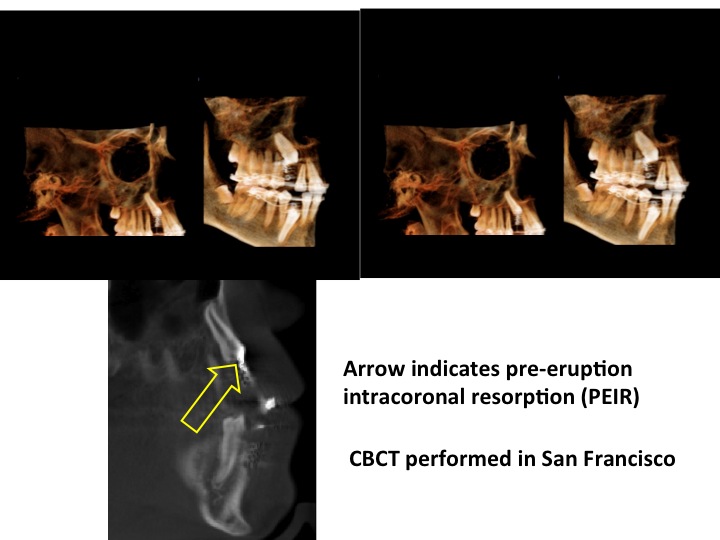
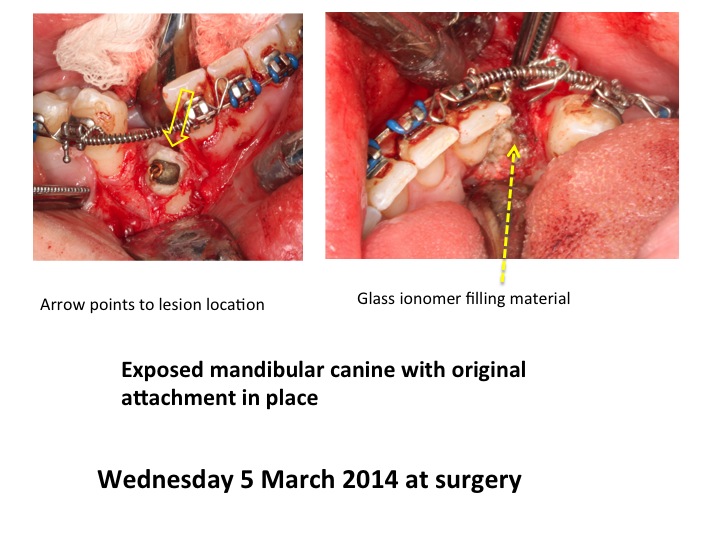
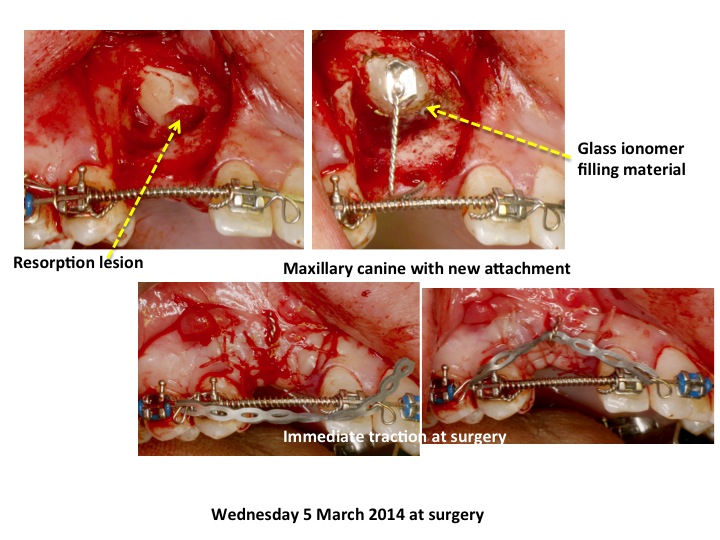
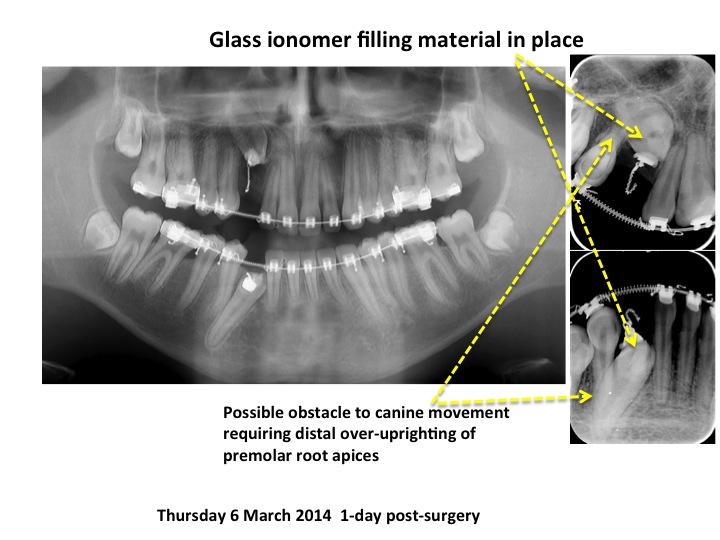
My concern was that in each canine, there was an advanced lesion of pre-eruptive crown resorption, which is not present in any other teeth. This raised my suspicions that this was the only likely remaining untried reason for the two teeth not to have responded to orthodontic traction. Accordingly, I recommended that the teeth be re-exposed and the lesions partially excavated and then sealed off from the surrounding tissues using a glass ionomer cement filling material. Since these lesions are nourished from the surrounding tissues and not from the pulp, this should be sufficient to arrest the resorption. It is almost certain that any attempt to complete excavation of the mush would lead to exposure of the pulp and the need for root canal therapy, even though the pulp is not involved and entirely symptomless.
The orthodontist and surgeons consulted in San Francisco have refused to follow this recommendation and so Dr. Bower decided to have the surgical part of the treatment done here, in Jerusalem. The operation was performed on Wednesday 5 March under general anesthetic and successfully completed as planned. Traction was re-applied immediately and it is hoped that the teeth will now respond, although Dr. Bower accepts that this still may not occur.
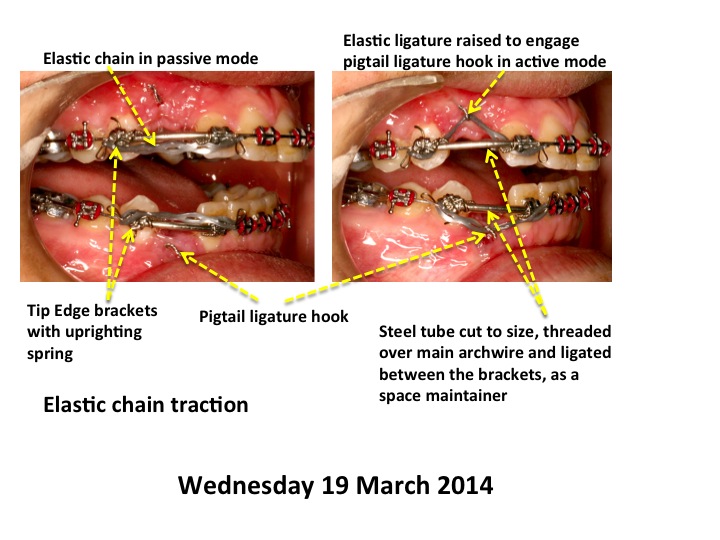
I have seen Sam on two post-surgical visits and have set up the orthodontic appliances to continue the needed traction in what I regard as the most efficient manner. It will be noted from the immediate post-operative radiographs that the first premolars adjacent to both teeth require distal root uprighting, in order to clear the way for the canines to erupt. Since the Bower's stay in Jerusalem has been very short, there has been no time for me to distally upright these roots and to further expand the space available at the crown level. In order for these tasks to be undertaken while still using a heavy rectangular base arch, I have substituted the original straight wire brackets on these two teeth with Tip-Edge brackets which, because of the unique configuration of their slot, permit full engagement of the heavy rectangular archwire in an angulated orientation of the bracket. The slot configuration will allow uprighting to occur with the use of an uprighting spring, which I placed in the vertical slot yesterday.
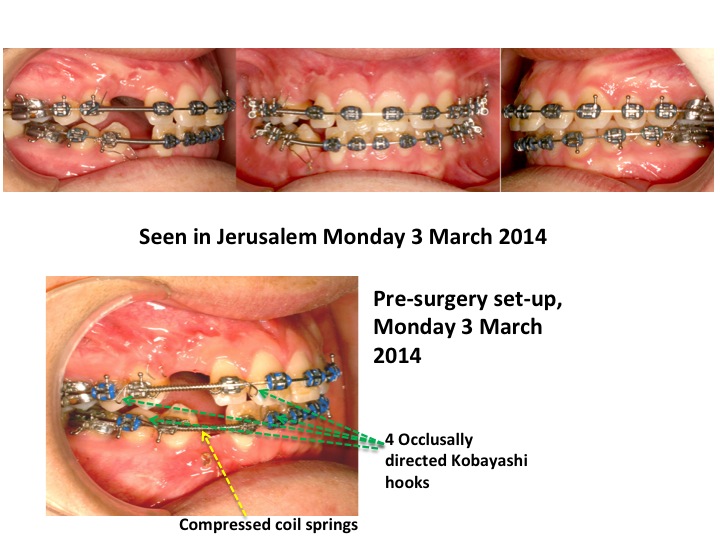
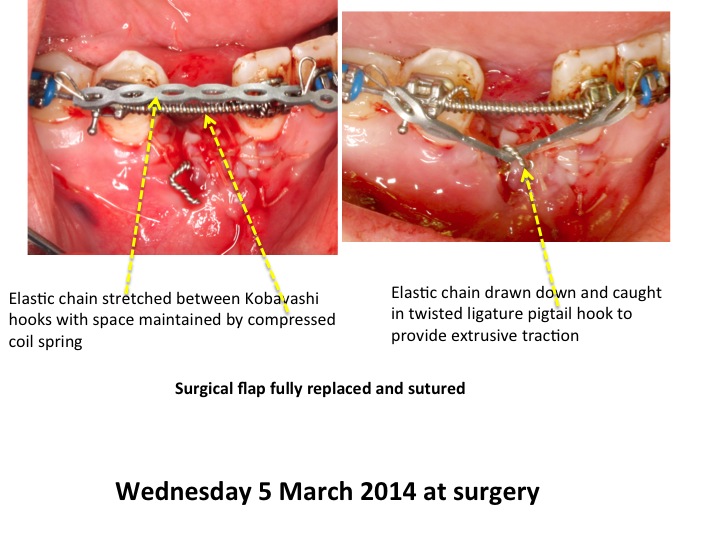
At the same time, I have inserted a measured length of tube over the archwire and between the lateral incisor and first premolar brackets in each jaw, to hold the spaces for the canine. An elastic chain was then stretched horizontally between the lateral incisor and first premolar brackets. In the maxilla, the middle section of the chain was stretched upwards and ensnared on the ligature hook from the canine, as it exited the tissue, to produce vertical elastic traction. The same procedure was followed in the mandible. Any progress that hopefully occurs will be recognizable by the fact that the ligature hook becomes longer, more exposed and closer to the archwire. It is recommended that the hook be rolled up and shortened in line with this progress and a new chain substituted every 10-14 days.
Applying traction to these canines has already caused loss of anchorage as witnessed by the lateral open bite on the right side. Accordingly, vertical “up-and-down” elastics are indicated to buttress the anchorage on the right side of the mouth. However, I have not made provision for this at the moment, in order not to over-complicate things. I am hopeful of movement of both canines and any further bite opening on that side may be later addressed with up-and-down elastics at a more convenient time. Obviously, if the teeth do not respond to the traction, their extraction will be advised and the Bowers are aware of this possibility. In this unfortunate event, vertical elastics may be re-applied to close down the bite.
...
The canine in the right side of both maxilla and mandible are impacted and have resisted every attempt to resolve them until the present time. Surgery and orthodontics have been performed more than once and by several people, to no avail. Dr. Bower is a very resourceful person and, from her internet searches, has maintained an e-mail correspondence with me over the past several months.
My concern was that in each canine, there was an advanced lesion of pre-eruptive crown resorption, which is not present in any other teeth. This raised my suspicions that this was the only likely remaining untried reason for the two teeth not to have responded to orthodontic traction. Accordingly, I recommended that the teeth be re-exposed and the lesions partially excavated and then sealed off from the surrounding tissues using a glass ionomer cement filling material. Since these lesions are nourished from the surrounding tissues and not from the pulp, this should be sufficient to arrest the resorption. It is almost certain that any attempt to complete excavation of the mush would lead to exposure of the pulp and the need for root canal therapy, even though the pulp is not involved and entirely symptomless.
The orthodontist and surgeons consulted in San Francisco have refused to follow this recommendation and so Dr. Bower decided to have the surgical part of the treatment done here, in Jerusalem. The operation was performed on Wednesday 5 March under general anesthetic and successfully completed as planned. Traction was re-applied immediately and it is hoped that the teeth will now respond, although Dr. Bower accepts that this still may not occur.
I have seen Sam on two post-surgical visits and have set up the orthodontic appliances to continue the needed traction in what I regard as the most efficient manner. It will be noted from the immediate post-operative radiographs that the first premolars adjacent to both teeth require distal root uprighting, in order to clear the way for the canines to erupt. Since the Bower's stay in Jerusalem has been very short, there has been no time for me to distally upright these roots and to further expand the space available at the crown level. In order for these tasks to be undertaken while still using a heavy rectangular base arch, I have substituted the original straight wire brackets on these two teeth with Tip-Edge brackets which, because of the unique configuration of their slot, permit full engagement of the heavy rectangular archwire in an angulated orientation of the bracket. The slot configuration will allow uprighting to occur with the use of an uprighting spring, which I placed in the vertical slot yesterday.
At the same time, I have inserted a measured length of tube over the archwire and between the lateral incisor and first premolar brackets in each jaw, to hold the spaces for the canine. An elastic chain was then stretched horizontally between the lateral incisor and first premolar brackets. In the maxilla, the middle section of the chain was stretched upwards and ensnared on the ligature hook from the canine, as it exited the tissue, to produce vertical elastic traction. The same procedure was followed in the mandible. Any progress that hopefully occurs will be recognizable by the fact that the ligature hook becomes longer, more exposed and closer to the archwire. It is recommended that the hook be rolled up and shortened in line with this progress and a new chain substituted every 10-14 days.
Applying traction to these canines has already caused loss of anchorage as witnessed by the lateral open bite on the right side. Accordingly, vertical “up-and-down” elastics are indicated to buttress the anchorage on the right side of the mouth. However, I have not made provision for this at the moment, in order not to over-complicate things. I am hopeful of movement of both canines and any further bite opening on that side may be later addressed with up-and-down elastics at a more convenient time. Obviously, if the teeth do not respond to the traction, their extraction will be advised and the Bowers are aware of this possibility. In this unfortunate event, vertical elastics may be re-applied to close down the bite.
...
|

Garden of Getsemane, Jerusalem
|

Dr. Becker goes about his business in his dental office like a true master of his craft. Going back and forth a dozen times to cut the spacers to the precise length; explaining the biodynamics behind springs and chains with the passion of someone who has a full grasp of what he is doing. The true spirit of a good teacher, who engages both patient and his assistants in the the whats and whys of what he is doing.
I am sure this ordeal with Sam's teeth has cost me about ten years of expected lifetime. It is very distressing to
discover that impacted teeth in a youth has been trivialized and managed offhandedly, the more I myself understood the complexities of impacted canines.
Meeting Dr. Becker made the contrast very stark. To see competence and caring together in the person in charge, gives you a sense of relief. Ideally, Dr. Becker would have adopted Sam, or we would have emigrated, so we could have benefitted from Dr. Becker's expertise until Sam was all done; short of that, Dr. Becker has explained, in his very thorough, yet simple way, what needs to be done, to the next local orthodontist.
Adding to Sam's orthodontia bills:
$ 5066
$ 5066