Part 5: Dr Kai and Dr Schendel
 Cephalogram, 7/15/14
Cephalogram, 7/15/14
July 15, 2014. Dr Kenneth Kai (San Jose)
Dr Kai took a cephalogram ($ 90) and some oral imaging with a digital wand instead of the plaster mold. Very nifty
(and $ 200). He is interested in persuing the apicotomy for dilacerated canines in 'the inverted Y of Ennis' as described by Dr Puricelli. He saw the dilacerated root of #6 and thought it could be acting as a hook and preventing traction. He looked at my collected material on dilaceration and apicotomy and had an open mind right away!
Actually, now having heard a good number of opinions, it sounds like it's about 50/50 on Sam's dilaceration and if it is the reason or not for #6 not moving, which just goes to show that orthodontics can be a matter of opinion. However, apicotomy seems a reasonable choice where we are, it's a last resort (but, Dr Puricelli recommends it as first choice in her 2007 article!). There are only so many reasons for a tooth not to move, and blaming the dilaceration with or without ankylosis, seems the logical next step. So, now we are looking for a skilled oral surgeon.
First try didn't go so well. Turns out the San Francisco surgeon, Dr Martin Chin, we went to for a consultation had been approached by Dr Nelson for the PEIR surgery last fall, and declined. Too out of the box. He had not read my email, which I had hoped would make the consultation more efficient. The strange thing was that he kept asking if we thought #27 had really moved. When we said 'yes!', he insisted that movement is relative, and that it could instead be all the neighboring teeth were moving. Looking at the panos, with the socket outlined with the lamina dura, and #27 clearly moving out, it seemed really bizarre. It was as if the surgeon in question just didn't want to see it moving, since he didn't approve of the surgery. A wasted trip to San Francisco (and $ 150).
According to Dr Kai, Dr Chin thought apicotomy too experimental and he (and/or Dr Nelson) thought we should abandon #6 where it is until Sam is older. That is a new take on things, and seems to just be postponing treatment, and I think it would be very frustrating for Sam after everything.
Dr Kai took a cephalogram ($ 90) and some oral imaging with a digital wand instead of the plaster mold. Very nifty
(and $ 200). He is interested in persuing the apicotomy for dilacerated canines in 'the inverted Y of Ennis' as described by Dr Puricelli. He saw the dilacerated root of #6 and thought it could be acting as a hook and preventing traction. He looked at my collected material on dilaceration and apicotomy and had an open mind right away!
Actually, now having heard a good number of opinions, it sounds like it's about 50/50 on Sam's dilaceration and if it is the reason or not for #6 not moving, which just goes to show that orthodontics can be a matter of opinion. However, apicotomy seems a reasonable choice where we are, it's a last resort (but, Dr Puricelli recommends it as first choice in her 2007 article!). There are only so many reasons for a tooth not to move, and blaming the dilaceration with or without ankylosis, seems the logical next step. So, now we are looking for a skilled oral surgeon.
First try didn't go so well. Turns out the San Francisco surgeon, Dr Martin Chin, we went to for a consultation had been approached by Dr Nelson for the PEIR surgery last fall, and declined. Too out of the box. He had not read my email, which I had hoped would make the consultation more efficient. The strange thing was that he kept asking if we thought #27 had really moved. When we said 'yes!', he insisted that movement is relative, and that it could instead be all the neighboring teeth were moving. Looking at the panos, with the socket outlined with the lamina dura, and #27 clearly moving out, it seemed really bizarre. It was as if the surgeon in question just didn't want to see it moving, since he didn't approve of the surgery. A wasted trip to San Francisco (and $ 150).
According to Dr Kai, Dr Chin thought apicotomy too experimental and he (and/or Dr Nelson) thought we should abandon #6 where it is until Sam is older. That is a new take on things, and seems to just be postponing treatment, and I think it would be very frustrating for Sam after everything.
|
September 1st, 2014.
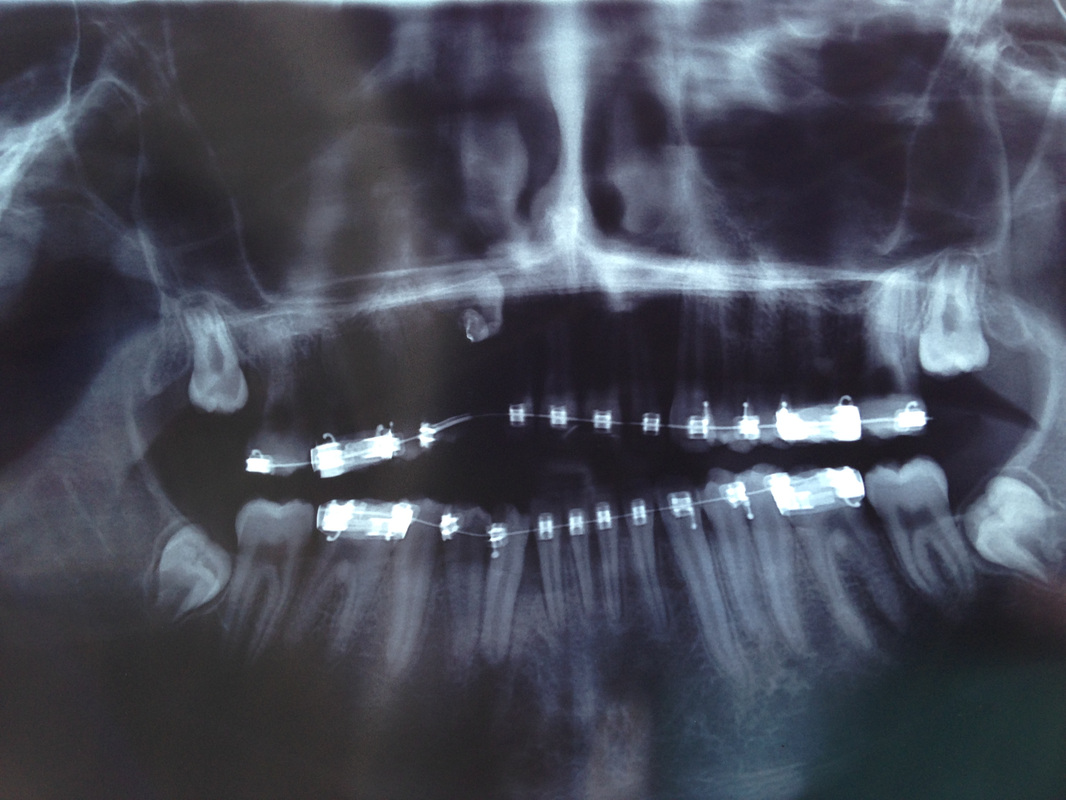
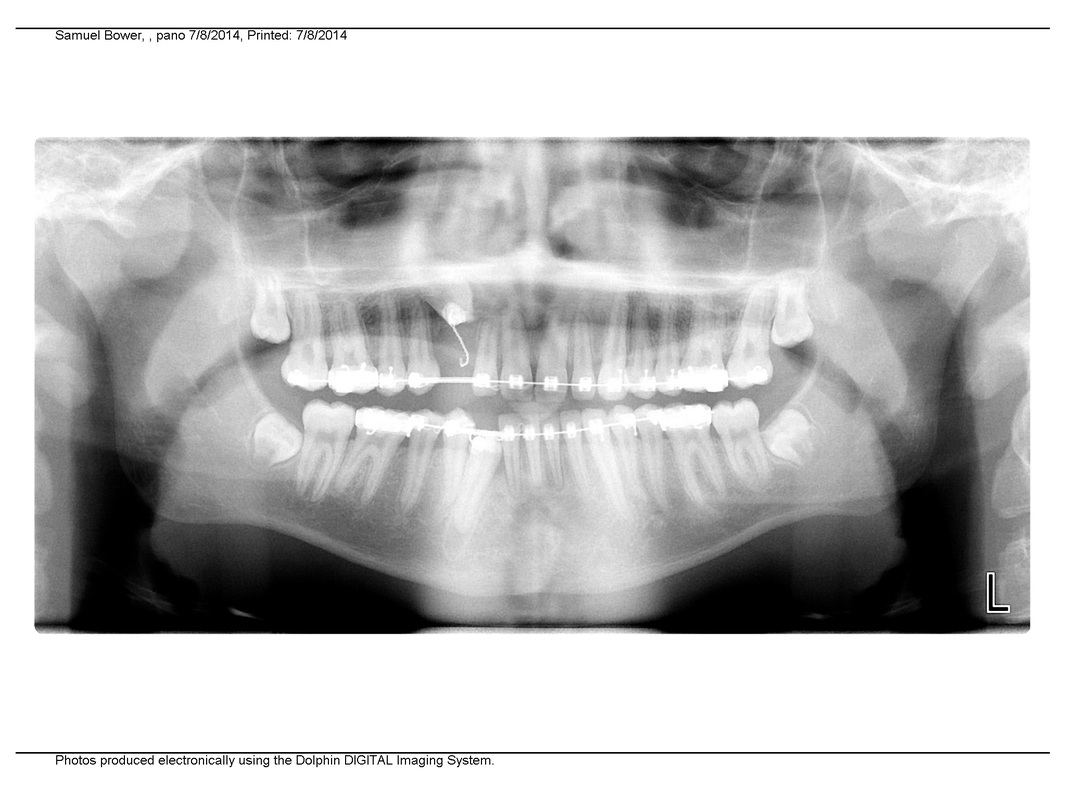
It took half the summer to find an orthodontist and the other half to find an oral surgeon! Surgery has to be after school starts regrettably. Unfortunately as above with Dr Chin, Dr Kai did not directly contact the surgeon, but what I had to bring along to consultations was a paper referral from Dr Kai asking: For the lower right cuspid: Please expose & replace attachment. For the upper right impacted cuspid with apical dilaceration: Please expose & perform "apicotomy" as per mom's reference. |

The upper canine's pigtail can be seen where it was left.
|

A speck of the lower canine is visible. (Would be interesting to know if it actually can move on it's own at this point. Can the periodontal ligament do anything by itself?) Theory is that we need a spring and more room.
|
We met with Dr Schendel and his assistant Dr Gupta twice before surgery. Dr Schendel said the apicotomy was an easy operation.
I was worried when they didn't open the 'Dropbox' to look at the CBCT. After he said he looked at it, Dr Schendel said he couldn't see the dilaceration. I showed him the images I had put on top of the gallery for easy access. Dr Schendel would look again.
Dr Schendel, when questioned, said that you can apply a force of 500 gram after an osteotomy.
Unfortunately, Dr Schendel does not communicate with his patients directly, you have to go through his secretary. In one email via Dr Schendel's assistant I asked if it would be possible to takes some photos during the surgery, a practice that Dr Becker recommends, Dr Schendel never answereed.
I was worried when they didn't open the 'Dropbox' to look at the CBCT. After he said he looked at it, Dr Schendel said he couldn't see the dilaceration. I showed him the images I had put on top of the gallery for easy access. Dr Schendel would look again.
Dr Schendel, when questioned, said that you can apply a force of 500 gram after an osteotomy.
Unfortunately, Dr Schendel does not communicate with his patients directly, you have to go through his secretary. In one email via Dr Schendel's assistant I asked if it would be possible to takes some photos during the surgery, a practice that Dr Becker recommends, Dr Schendel never answereed.

September 8th, Dr Kai
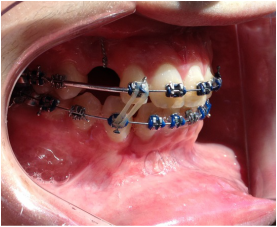
Dr Kai puts a spring over #27, and attaches #6's pigtail to the archwire which he has bent a bit upward.
Restarting rubber bands for the open bite.
Orthodontics will be $ 4 200 on top of
200 initial 'consultations'
90 cephalogram
200 oral imaging
Total: $ 4 590
Dr Kai puts a spring over #27, and attaches #6's pigtail to the archwire which he has bent a bit upward.
Restarting rubber bands for the open bite.
Orthodontics will be $ 4 200 on top of
200 initial 'consultations'
90 cephalogram
200 oral imaging
Total: $ 4 590
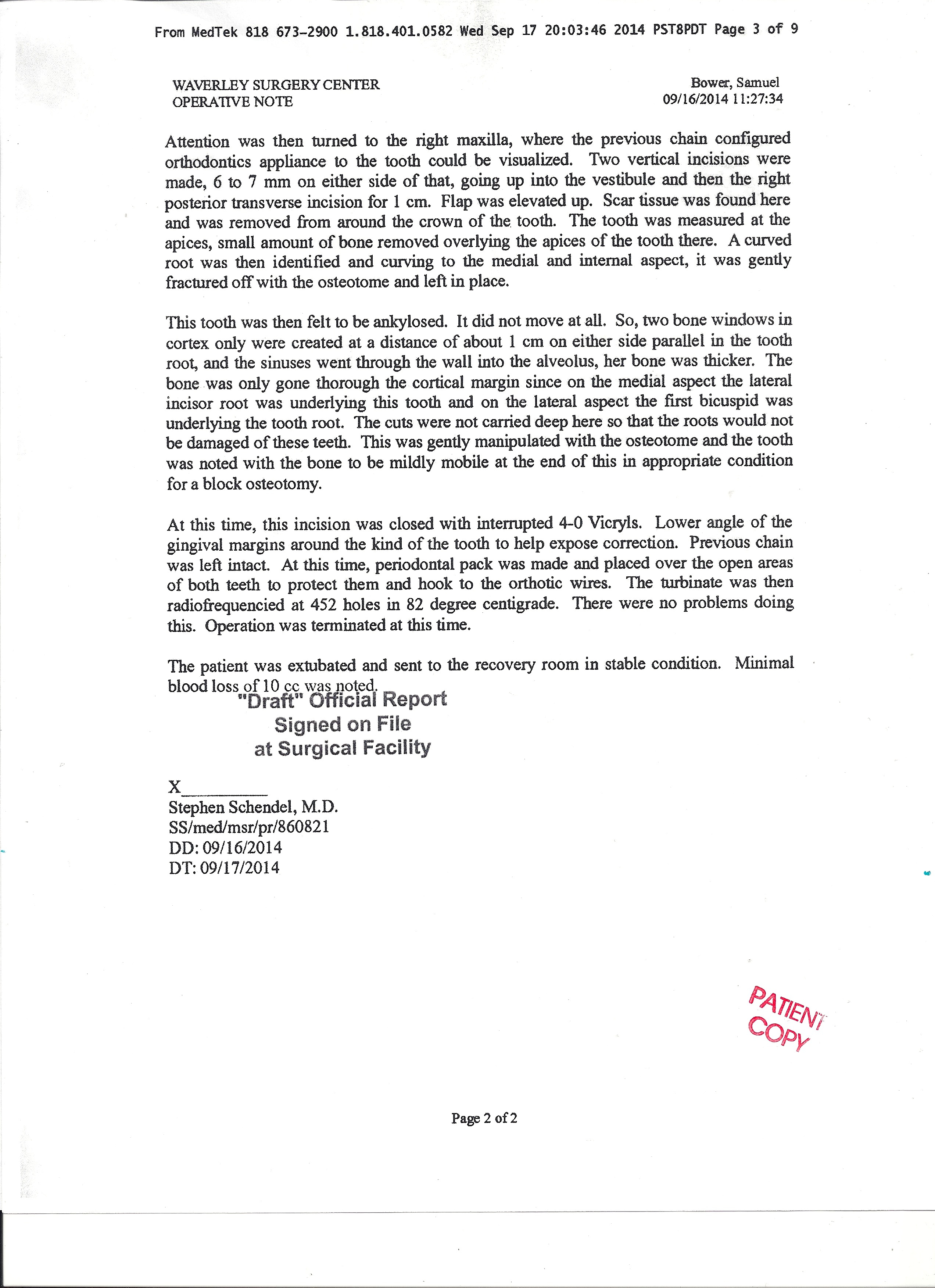
September 16th, Surgery: APICOTOMY (See http://impactedcanine.weebly.com/dilaceration-and-apicotomy.html) and BLOCK OSTEOTOMY and exposing of #27.
Reading through the material I've found on the subject, I find that Dr Puricelli says that the treated canines
of her 26 successfull cases had an 'average period for total coronary eruption is eighteen months' (article from 2007). She recommends traction with 100-150 g from the 5th day post surgery. More vertical traction during the first 60 days, radiologic control examinations on day 45 and 90. Dr Araujo's paper talks of Patient 1 having a
totally erupted canine in 10 weeks, for Patient 3 it took one month. Dr Araujo reactivates tension every two weeks: The force should be monitored every two weeks because long periods without activation can
lead to new ankylosis.
Reading through the material I've found on the subject, I find that Dr Puricelli says that the treated canines
of her 26 successfull cases had an 'average period for total coronary eruption is eighteen months' (article from 2007). She recommends traction with 100-150 g from the 5th day post surgery. More vertical traction during the first 60 days, radiologic control examinations on day 45 and 90. Dr Araujo's paper talks of Patient 1 having a
totally erupted canine in 10 weeks, for Patient 3 it took one month. Dr Araujo reactivates tension every two weeks: The force should be monitored every two weeks because long periods without activation can
lead to new ankylosis.
September 16, Surgery at the Waverly, Palo Alto by Dr Stephen Schendel an Dr Rishi Gupta
General anesthesia 1 1/2 hours.
Apicotomy of #6 and 'block osteotomy', which is perforation of the bone around the tooth to mobilize it.
Dr Schendel writes that the tooth was 'mildly mobile' after the osteotomy.
Broken off apex left in place.
Dr Kai had asked for a new attachment on #27, but Dr Schendel instead just exposed the crown
and put a dental pack on top. No explanation.
Periodontal packs as 'bandages'. Post op visit in 10 days so that the periodontal packs can be removed and a bracket put on #27.
Sam very sleepy, somewhat grumpy afterwards.
Oral Surgeon: $ 1 000
Clinic (Waverly, Palo Alto): $ 2 400
Anesthesiologist: $ 1 430
Total: $ 4830 (plus $ 875 for 'turbinate hypertrophy treatment, burning off excess mucosa in the nose with
radiofrequency waves. Sam sometimes has 'loud breathing'.)
Surgery notes. Unfortunately the surgery notes take many weeks before they are ready, so it's very much an after-the-fact information. The notes talk of #7, but the upper right canine, is actually #6.
General anesthesia 1 1/2 hours.
Apicotomy of #6 and 'block osteotomy', which is perforation of the bone around the tooth to mobilize it.
Dr Schendel writes that the tooth was 'mildly mobile' after the osteotomy.
Broken off apex left in place.
Dr Kai had asked for a new attachment on #27, but Dr Schendel instead just exposed the crown
and put a dental pack on top. No explanation.
Periodontal packs as 'bandages'. Post op visit in 10 days so that the periodontal packs can be removed and a bracket put on #27.
Sam very sleepy, somewhat grumpy afterwards.
Oral Surgeon: $ 1 000
Clinic (Waverly, Palo Alto): $ 2 400
Anesthesiologist: $ 1 430
Total: $ 4830 (plus $ 875 for 'turbinate hypertrophy treatment, burning off excess mucosa in the nose with
radiofrequency waves. Sam sometimes has 'loud breathing'.)
Surgery notes. Unfortunately the surgery notes take many weeks before they are ready, so it's very much an after-the-fact information. The notes talk of #7, but the upper right canine, is actually #6.
| schendelsurgery1.jpg |
{kind=link}
| schendelsurgery2.jpg |
{kind=link}

|

|
|
September 17, Dr Kai
Sam more swollen today, should have done more ice yesterday. Dr Kai's intention was to apply immediate traction, or rather, day after surgery, to #6. He poked into the dental pack. When he saw the blue elastic he asked me if that was 'his elastic'. Thanks to iPad I could show Dr Kai that he had put on a blue power chain at the previous visit. Dr Kai was satisfied with this and left #6 it like that until next visit Sep 29 when we will also get the bracket on #27. He thinks the force on #6 right now is about 200g. (A bit frustrating that we made this 8 am appointment in commute traffic, basically a 3 hour drive altogether, for nothing more than a look at the dental packs.) |

|
|
September 19,
Peak of swelling |

Right side = Swollen Sam
|

Left side = Normal Sam
|
September 26, Post op visit with Dr Gupta: NO TRACTION!
Removing the periodontal pack. I did not know that #6 was still exposed, at the end of a little tunnel. A bit scary seeing it up there. Thin line around it where Dr Schendel cut/drilled? to dislodge it, the 'coniotomy'.
A rather shocking piece of information: The power chain and wire to #6 was totally embedded in the dental pack cement so there has not been any active traction yet according to Dr Gupta. The need for traction to successfully extrude the canine after apicotomy and osteotomy was apparently not a surgical concern.
#27 right is fully exposed. Dr Kai had asked for an attachment, but Dr Schendel for some reason preferred having Dr Kai put a bracket instead and just laid the tooth open.
Good healing. Stitches out in a week.
Sam has loss of sensitivity on a patch of right cheek and right upper lip. Dr Gupta says it's the infraorbital nerve and Sam will get his sensitivity back in a few weeks. The swelling is still not completely gone.
Removing the periodontal pack. I did not know that #6 was still exposed, at the end of a little tunnel. A bit scary seeing it up there. Thin line around it where Dr Schendel cut/drilled? to dislodge it, the 'coniotomy'.
A rather shocking piece of information: The power chain and wire to #6 was totally embedded in the dental pack cement so there has not been any active traction yet according to Dr Gupta. The need for traction to successfully extrude the canine after apicotomy and osteotomy was apparently not a surgical concern.
#27 right is fully exposed. Dr Kai had asked for an attachment, but Dr Schendel for some reason preferred having Dr Kai put a bracket instead and just laid the tooth open.
Good healing. Stitches out in a week.
Sam has loss of sensitivity on a patch of right cheek and right upper lip. Dr Gupta says it's the infraorbital nerve and Sam will get his sensitivity back in a few weeks. The swelling is still not completely gone.

|

|

|
|
September 29, 2 weeks post op. Dr Kai
Dr Kai got on a bracket on #27 and restarted the traction after the 10 week lapse. #6 got a new power chain, 13 days post surgery. There are three kinds of elastics according to Dr Kai, and the ones he put on are good for four weeks, and apparently not the kind of elastics used in Dr Puricelli and Dr Araujo's article on apicotomy, where they recommend reapplied force every two weeks to avoid ankylosis. Dr Kai wanted four weeks till next appointment. Still, I preferred changing elastics every two weeks, at least in this immediate post operative period, and Dr Kai was a bit annoyed, but OK with that. |

|
Oct 3, Dr Schendel
Dr Schendel removed the stitches. (Lidocaine/ benzocaine? was first dabbed on to the area with stitches.) As Dr Schendel said, it appears that the lower canine has already moved some. The gum tissue will follow the tooth up. We have an appointment in 3 weeks.
Oct 4
Sam woke up in the morning with his cheek really swollen again. We can't figure out why. Taking the stitches out was a very minor thing, and there are no other signs of infection, no redness, no warmth, no pain, no lymphnodes...
Dr Schendel removed the stitches. (Lidocaine/ benzocaine? was first dabbed on to the area with stitches.) As Dr Schendel said, it appears that the lower canine has already moved some. The gum tissue will follow the tooth up. We have an appointment in 3 weeks.
Oct 4
Sam woke up in the morning with his cheek really swollen again. We can't figure out why. Taking the stitches out was a very minor thing, and there are no other signs of infection, no redness, no warmth, no pain, no lymphnodes...

|

|

|
Lidocaine?
(According to the surgery notes: 'the surgical areas were preinjected with lidocaine') |
Oct 5
Less swelling in the morning, and almost gone by evening. After a bit of research I think that Sam had a
type 4 delayed hypersensitivity reaction in the form of angioedema to the topical lidocaine that was put on before the stitches were taken off. It's rare, but so is PEIR
Less swelling in the morning, and almost gone by evening. After a bit of research I think that Sam had a
type 4 delayed hypersensitivity reaction in the form of angioedema to the topical lidocaine that was put on before the stitches were taken off. It's rare, but so is PEIR
Oct 17, 4 weeks post op. Dr Lisa
Dr Lisa. #27 moved a lot. The bracket is put into the archwire. Sam says he feels a bit sore around the tooth, looks a bit red.
New power chain on #6. Dr Lisa said she increased the force pulling it.
(Dr Schendel said you can put 500 grams of force on a tooth that has been loosened by osteotomy.
Don't know if it was meant that there would be no rubber bands on the upper left side. (Dr Lisa called to say the assistant forgot the rubber bands, but we can leave it until next appointment)
Dr Lisa. #27 moved a lot. The bracket is put into the archwire. Sam says he feels a bit sore around the tooth, looks a bit red.
New power chain on #6. Dr Lisa said she increased the force pulling it.
(Dr Schendel said you can put 500 grams of force on a tooth that has been loosened by osteotomy.
Don't know if it was meant that there would be no rubber bands on the upper left side. (Dr Lisa called to say the assistant forgot the rubber bands, but we can leave it until next appointment)

|

|
Oct 27, 6 weeks post op, Dr Schendel
The pano shows that the upper teeth are misaligned and the open bite increased. The upper canine does not seem to be doing anything but pulling up its neighbors into a tent.
I asked about how and when you apply 500 grams of force as Dr Schendel had previously said you can do in cases of osteotomy. Dr Schendel replied vaguely that maybe Dr Kai wants to pull more, but didn't say how this
cold be done. TAD?
(Sam still has the sensitivity loss. Dr Schendel doesn't believe in my lidocaine theory, but thinks the removal of stitches caused an infection. If that's the case, I guess we were lucky the infection went away after 24 hours.)
I asked about how and when you apply 500 grams of force as Dr Schendel had previously said you can do in cases of osteotomy. Dr Schendel replied vaguely that maybe Dr Kai wants to pull more, but didn't say how this
cold be done. TAD?
(Sam still has the sensitivity loss. Dr Schendel doesn't believe in my lidocaine theory, but thinks the removal of stitches caused an infection. If that's the case, I guess we were lucky the infection went away after 24 hours.)
Oct 26 2014. Photo of a hard copy, not great quality.
Dr Schendel's office does not have digital imagery.
Radiation dose = 10 µSiv
|
For comparison: August 2014
|
Oct 29, Dr Kai.
Dr Kai declared #6 ankylosed. He redid the brackets on #27 and #7, and put in new wire. Sam is wearing rubber bands between #8 and #29.
I asked Dr Kai about using a TAD and applying more force.
Dr Kia confirmed that he had no communication with Dr Schendel before or after Sam's surgery other than the
initial referral note I brought to the first consultation, asking for apicotomy and osteotomy.
Almost $ 5000 in orthodontia and $ 5000 in surgery expenses will not buy you a phone call between orthodontist and oral surgeon. How and when to apply traction after surgery, a crucial point in the whole enterprise, was never discussed. It's a crushing realization.
Dr Kia's plan is to leave #6 in until time for a temporary tooth placement keeper, then bone graft and implant when Sam's mouth is fully grown, as based on cephalograms.
Got message from Dr Kai that he was willing to have another go at #6 with TAD. He had not discussed this with Dr Schendel, so I tried getting the orthodontist and surgeon to discuss this by email. Dr Schendel replied that the tooth is ankylosed.
I tried asking Dr Schendel about why he used a dental plack if that made traction impossible, and how you can apply 500 gram of traction if you don't use a TAD. Only reply was that ''that's how it is done'. No mention of the next step to deal with #6.
I asked Dr Kai about using a TAD and applying more force.
Dr Kia confirmed that he had no communication with Dr Schendel before or after Sam's surgery other than the
initial referral note I brought to the first consultation, asking for apicotomy and osteotomy.
Almost $ 5000 in orthodontia and $ 5000 in surgery expenses will not buy you a phone call between orthodontist and oral surgeon. How and when to apply traction after surgery, a crucial point in the whole enterprise, was never discussed. It's a crushing realization.
Dr Kia's plan is to leave #6 in until time for a temporary tooth placement keeper, then bone graft and implant when Sam's mouth is fully grown, as based on cephalograms.
Got message from Dr Kai that he was willing to have another go at #6 with TAD. He had not discussed this with Dr Schendel, so I tried getting the orthodontist and surgeon to discuss this by email. Dr Schendel replied that the tooth is ankylosed.
I tried asking Dr Schendel about why he used a dental plack if that made traction impossible, and how you can apply 500 gram of traction if you don't use a TAD. Only reply was that ''that's how it is done'. No mention of the next step to deal with #6.

|

|

Looks like the glass ionomer filling was removed by Dr Schendel.
|
I updated Dr Becker on where we have ended up. Dr Becker's comment:
The upper canine #6 will need to be extracted and the only question that remains is when?
We do not know the reason that the tooth has not responded, while the lower one has. There are several possibilities and ankylosis is just one. Another possibility is invasive cervical root resorption - see http://dr-adrianbecker.com/page.php?pageId=281&nlid=54 . This is a potent reason for non-eruption and is apparently closely associated with PEIR - in fact, I believe it to be the same process - see- http://dr-adrianbecker.com/page.php?pageId=281&nlid=59. If ICRR is indeed the reason for Sam's non-erupting canine, after PEIR has been eliminated, then the invasive resorption will continue on to eat away at the tooth and its extraction may never be totally complete. Later placement of an implant will need to take note of small remnants of unresorbed root, although it is now common practice to place an implant directly through these remnants, without eliminating them and probably with a graft of artificial/bovine/dried bone. However, you should ask an implantologist what would be best.
The upper canine #6 will need to be extracted and the only question that remains is when?
We do not know the reason that the tooth has not responded, while the lower one has. There are several possibilities and ankylosis is just one. Another possibility is invasive cervical root resorption - see http://dr-adrianbecker.com/page.php?pageId=281&nlid=54 . This is a potent reason for non-eruption and is apparently closely associated with PEIR - in fact, I believe it to be the same process - see- http://dr-adrianbecker.com/page.php?pageId=281&nlid=59. If ICRR is indeed the reason for Sam's non-erupting canine, after PEIR has been eliminated, then the invasive resorption will continue on to eat away at the tooth and its extraction may never be totally complete. Later placement of an implant will need to take note of small remnants of unresorbed root, although it is now common practice to place an implant directly through these remnants, without eliminating them and probably with a graft of artificial/bovine/dried bone. However, you should ask an implantologist what would be best.
|
Nov 24, email Dr Kai
It feels to Sam as if #27 is being pulled up rather than the upper arch being pulled down, and #27 is sticking up over the other teeth. Dr Kai's response: We are all right, do not worry, I want to see the UR2 overlap with the LR2 & UR4 contacting the LR4 then stop the elastics. There is a tendency for the LR3 to relapse back down so we want it to be held up for a little while. |

|
I am relieved that Sam's dentist, Dr Giannotti, is a thoughtful person who bothers asking Dr Becker for advice on how to restore #27:
As I see it, the resorption has been totally neutralized and is now a "soft center" which does not threaten the vitality of the tooth. That being so, there is no reason to remove it unless the structure of the crown of the tooth is endangered by a physical lack of dentine body, which might cause fracture of the enamel covering it. If you decide to remove the resorption debris, it will almost inevitably result in a vital exposure of the pulp - the lesion does not stimulate secondary dentine. Then there will be the need for root canal therapy - which itself carries with it the risk of failure - albeit extremely small. Restoration will then require a post and crown - also with a modicum of risk of failure. If you consider that the tooth structure is too weak now to retain a composite filling, then this must nevertheless be your course of action. If, on the other hand, sealing the deeper part of the resorption debris in with composite filling gives a reasonable restorative prognosis, then the risks are very small - in terms of possibly re-doing the filling, if the enamel fractures. A post and crown can always be done later if and when indicated.
As I see it, the resorption has been totally neutralized and is now a "soft center" which does not threaten the vitality of the tooth. That being so, there is no reason to remove it unless the structure of the crown of the tooth is endangered by a physical lack of dentine body, which might cause fracture of the enamel covering it. If you decide to remove the resorption debris, it will almost inevitably result in a vital exposure of the pulp - the lesion does not stimulate secondary dentine. Then there will be the need for root canal therapy - which itself carries with it the risk of failure - albeit extremely small. Restoration will then require a post and crown - also with a modicum of risk of failure. If you consider that the tooth structure is too weak now to retain a composite filling, then this must nevertheless be your course of action. If, on the other hand, sealing the deeper part of the resorption debris in with composite filling gives a reasonable restorative prognosis, then the risks are very small - in terms of possibly re-doing the filling, if the enamel fractures. A post and crown can always be done later if and when indicated.
Dec 12, Visit Dr Kai.
Changed to thicker wire in the mandible. Sam instructed to keep the rubber band on even though #27 sticking up above neighboring teeth. 6 weeks till next appointment.

|

|

|
|
|

|

|

|

|
Dec 22, Visit Dr Giannotti.
Positive news: Resorption damage of #27 less than she thought, it doesn't need a crown; and Sam doesn't have a 'gummy smile' which is good as far as implants go. Dr Giannotti doesn't want #27 to be extruded further, she can repair the tooth now and is going to contact Dr Kia. Bad news: she feelt that the maxillary bone was thin and the implant would have to be placed more labially. Dr Giannotti showed the kind of see-through plastic retainer that Sam could wear between bone graft and implant, with a fake tooth sitting in it.
It's hard not to feel extremely sad that Sam's 4 surgical attempts did not work, and that we are looking at a future with extraction, bone graft, fake tooth and implants instead. And if the implant lasts 25 years, Sam will be
dealing with this in his 40s again...
We are hoping that Dr Giannotti can find Sam a good surgeon/implantologist.
Jan 28, 2015, Visit Dr Kai
Starting on fifth year of braces and it's been 6 months with Dr Kai
Dr Kai takes measurement of the width of #27 and compares it to #22. (The real discrepancy though would be in height rather than width, since #27 is 3 mm or so longer than the neighboring teeth.) Dr Kai explains that there are several options on how to angle #27 depending on how Dr Giannotti wants to repair it. Dr Giannotti and Dr Kai had still not discussed this and to avoid further delays, I finally manage to reach Dr Giannotti by phone at her office and we had a phone conference. I am very concerned with getting Sam the oral surgeon consult. Dr Giannotti suggested Dr Girod, whom she would contact.
Dr Kai wants to angle #27, pull the mesial more labial. He says the crown and root do not match, the tooth is 'deformed', so there is no ideal solution, we have to settle with a compromise. (Actually, I don't know why there would be anything other to the tooth than the resorption of part of the crown.)
Dr Kai took a lot f photos to send to Dr Giannotti. He asks Dr Giannotti to take periapicals of #22 and #27. It will take 3 visits, 15 weeks to turn the tooth. Then the wire and bracket would be removed to give Dr Giannotti full access. Dr Kai also mentioned that #27 might need a periodontist to fix the gum line.
Dr Schendel assured us previously that the gum would follow the tooth up so that would be disappointing. I am wondering if this has something to do with how the tooth was exposed. Dr Kai asked for a new attachment, which could have been accomplished by simply accessing the top of the tooth. For some reason Dr Schendel choose to
expose the entire tooth.
Thankfully, Dr Kai is done pulling on #27 with the elastic, so it is one less dental chore for Sam to deal with.
We are now starting on his 5th year of braces and I am hoping that with communication and collaboration Sam will finally see the light at the end of the tunnel.
Positive news: Resorption damage of #27 less than she thought, it doesn't need a crown; and Sam doesn't have a 'gummy smile' which is good as far as implants go. Dr Giannotti doesn't want #27 to be extruded further, she can repair the tooth now and is going to contact Dr Kia. Bad news: she feelt that the maxillary bone was thin and the implant would have to be placed more labially. Dr Giannotti showed the kind of see-through plastic retainer that Sam could wear between bone graft and implant, with a fake tooth sitting in it.
It's hard not to feel extremely sad that Sam's 4 surgical attempts did not work, and that we are looking at a future with extraction, bone graft, fake tooth and implants instead. And if the implant lasts 25 years, Sam will be
dealing with this in his 40s again...
We are hoping that Dr Giannotti can find Sam a good surgeon/implantologist.
Jan 28, 2015, Visit Dr Kai
Starting on fifth year of braces and it's been 6 months with Dr Kai
Dr Kai takes measurement of the width of #27 and compares it to #22. (The real discrepancy though would be in height rather than width, since #27 is 3 mm or so longer than the neighboring teeth.) Dr Kai explains that there are several options on how to angle #27 depending on how Dr Giannotti wants to repair it. Dr Giannotti and Dr Kai had still not discussed this and to avoid further delays, I finally manage to reach Dr Giannotti by phone at her office and we had a phone conference. I am very concerned with getting Sam the oral surgeon consult. Dr Giannotti suggested Dr Girod, whom she would contact.
Dr Kai wants to angle #27, pull the mesial more labial. He says the crown and root do not match, the tooth is 'deformed', so there is no ideal solution, we have to settle with a compromise. (Actually, I don't know why there would be anything other to the tooth than the resorption of part of the crown.)
Dr Kai took a lot f photos to send to Dr Giannotti. He asks Dr Giannotti to take periapicals of #22 and #27. It will take 3 visits, 15 weeks to turn the tooth. Then the wire and bracket would be removed to give Dr Giannotti full access. Dr Kai also mentioned that #27 might need a periodontist to fix the gum line.
Dr Schendel assured us previously that the gum would follow the tooth up so that would be disappointing. I am wondering if this has something to do with how the tooth was exposed. Dr Kai asked for a new attachment, which could have been accomplished by simply accessing the top of the tooth. For some reason Dr Schendel choose to
expose the entire tooth.
Thankfully, Dr Kai is done pulling on #27 with the elastic, so it is one less dental chore for Sam to deal with.
We are now starting on his 5th year of braces and I am hoping that with communication and collaboration Sam will finally see the light at the end of the tunnel.
Feb 18, 2015, Visit Dr Giannotti
Dr Giannotti mends the crown of #27, takes off the 'peg' that was sticking out and that she says was deformed.
(In the end there was apparently no need for her to have the bracket removed, nor the wire clipped.)
Sam choose no local anesthetics and was fine.
Dr Giannotti mends the crown of #27, takes off the 'peg' that was sticking out and that she says was deformed.
(In the end there was apparently no need for her to have the bracket removed, nor the wire clipped.)
Sam choose no local anesthetics and was fine.

Pre fixing (Dr Giannotti's photo)
|

Pre fixing (Dr Giannotti's photo)
|
Dr Giannotti mentioned how it is important that the implant gets put in a correct spot for the top parts, abutment
and crown, will work; 'If the position is too facial, then what do you do?' (I don't know what you do when something goes wrong, but it sounds like another reason to worry.)
Dr Giannotti puts in a 'stent' (an acrylic guide that fits over the teeth with predrilled holes to show the angle of the implant) before surgery, that hopefully will prevent mistakes.
Dr Giannotti told us that Dr Girord at Stanford doesn't do implants anymore, she recommends Dr Lakha.
Feb 18, Visit Dr Kai
Dr Kai forgot why we came. He guessed we had a brace emergency, second guess was that we were preparing for 'The Operation' (?!).
The plan according to the last visit and a phone conference with DR Giannotti, was that Dr Giannotti would need to clip the wire to fix #27 and Dr Kai was to put it back.
Dr Gainnotti didn't clip the wire, but since we had had to make an appointment we showed up.
Dr Kai put in a new wire and elastics to close the gaps on the sides of #27. He forgot to clip the end of the wire
so we did get an 'emergency' when the wire end's poking got painful driving back. Sam clipped it with a wire cutter.
and crown, will work; 'If the position is too facial, then what do you do?' (I don't know what you do when something goes wrong, but it sounds like another reason to worry.)
Dr Giannotti puts in a 'stent' (an acrylic guide that fits over the teeth with predrilled holes to show the angle of the implant) before surgery, that hopefully will prevent mistakes.
Dr Giannotti told us that Dr Girord at Stanford doesn't do implants anymore, she recommends Dr Lakha.
Feb 18, Visit Dr Kai
Dr Kai forgot why we came. He guessed we had a brace emergency, second guess was that we were preparing for 'The Operation' (?!).
The plan according to the last visit and a phone conference with DR Giannotti, was that Dr Giannotti would need to clip the wire to fix #27 and Dr Kai was to put it back.
Dr Gainnotti didn't clip the wire, but since we had had to make an appointment we showed up.
Dr Kai put in a new wire and elastics to close the gaps on the sides of #27. He forgot to clip the end of the wire
so we did get an 'emergency' when the wire end's poking got painful driving back. Sam clipped it with a wire cutter.