Dr Bohannan, oral surgeon, Burlingame
I contact Dr Beck, and gets informed that he will retire at the end of the year, so we go about finding a new surgeon.
9/22/2017: Visit Dr William Bohannan, oral surgeon, Burlingame
9/22/2017: Visit Dr William Bohannan, oral surgeon, Burlingame
There are differences:
Dr Lakha could only take bone grafting material from under the wisdom teeth which he would extract in the same session. He was talking of multiple grafting sessions. He did not give us a treatment plan, and never gave an estimate of cost.
Dr Bohannan said you can’t take the bone under wisdom teeth if not a long time pass between extracting them and taking the graft some time after. He said he would take bone from chin, later changed it to back of the mandible.
Dr #3 said autolog bone grafts are old fashioned, he would just use particulate xenografts. He had us out the door with a full estimate, pain killers, and appointment date for surgery. He was out-of-network, so double cost from in-network.
Dr Lakha could only take bone grafting material from under the wisdom teeth which he would extract in the same session. He was talking of multiple grafting sessions. He did not give us a treatment plan, and never gave an estimate of cost.
Dr Bohannan said you can’t take the bone under wisdom teeth if not a long time pass between extracting them and taking the graft some time after. He said he would take bone from chin, later changed it to back of the mandible.
Dr #3 said autolog bone grafts are old fashioned, he would just use particulate xenografts. He had us out the door with a full estimate, pain killers, and appointment date for surgery. He was out-of-network, so double cost from in-network.
Oct 2017: Dr Becker's October Bulletin mentions this website in his arguments:'Surgeon & Orthodontist at the Surgical Exposure' https://www.dr-adrianbecker.com/page.php?pageId=281&nlid=198
Dr Becker tirelessly argues from the point of view of best result for the patient, which would be surgery as a collaborative effort, while the opposite view is that it is impractical for an orthodontist to be present, and concern of the legal aspects.
11/11/2017: Visit Dr William Bohannan
Treatment plan:
| bohannan_surgery.pdf |
12/15/2017: Surgery (
Took 1 1/2 hour, intravenous general anesthesia.
#6 was extracted, allograft bone to the socket and a collagen membrane.
Bone graft from external oblique ridge of the maxilla.
Fixing bone to site 6 with cortical bone screws.
Platelet rich plasma (autogenous) biological membrane to cover graft.
One complication mentioned was a 'through-and-through', an iatrogenic hole through the bone that had not healed with bone, but tissue was filling it up. The whole had to have a graft too, and apparently there is trouble healing a through-and-through, which is a problem since the implant has to anchor through it.
Took 1 1/2 hour, intravenous general anesthesia.
#6 was extracted, allograft bone to the socket and a collagen membrane.
Bone graft from external oblique ridge of the maxilla.
Fixing bone to site 6 with cortical bone screws.
Platelet rich plasma (autogenous) biological membrane to cover graft.
One complication mentioned was a 'through-and-through', an iatrogenic hole through the bone that had not healed with bone, but tissue was filling it up. The whole had to have a graft too, and apparently there is trouble healing a through-and-through, which is a problem since the implant has to anchor through it.

|

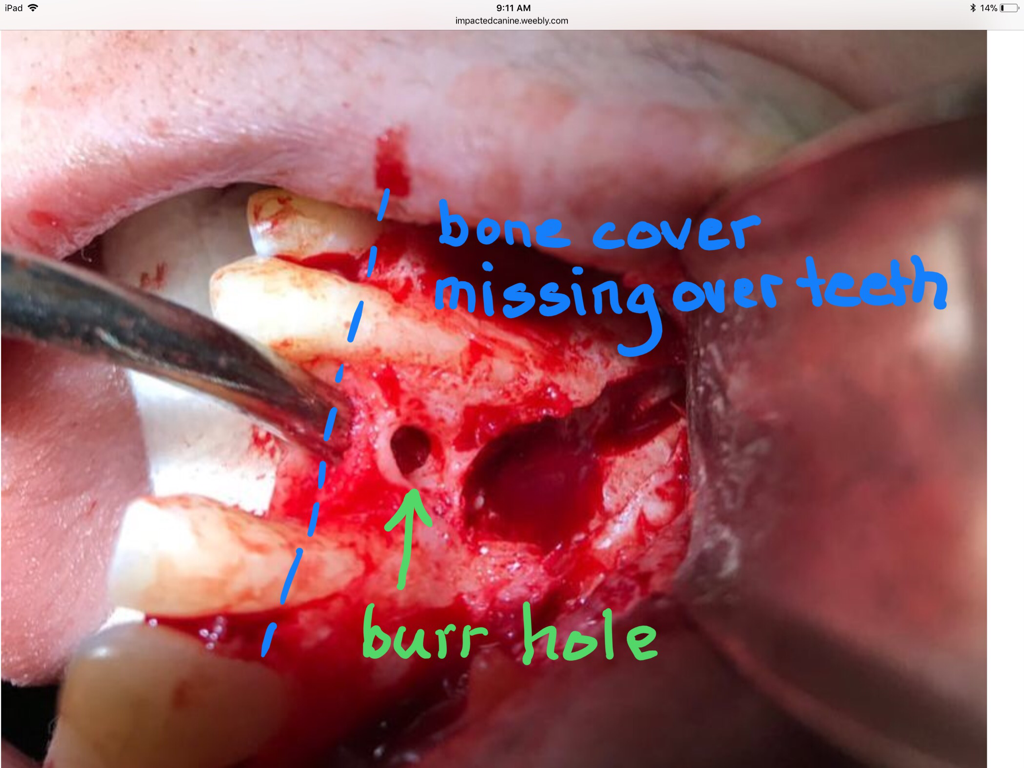
‘Thru-and-thru’ fenestration.
And...as I later figured out, #5 and #7 are affected by dehiscence = the facial surface of the teeth are not covered by bone.
|
Week following op a lot of back-and-forth about the upper retainer, that might have to be redone so as not to impinge on the grafting area. It gets messy because of the holidays. In the end it sounds like we don't want the area touch before Dr Bohannan takes a look at it, even if that means that the retainer has to wait until after the holidays.
12/22/2017: Postop visit
The good news is it is healing ok. But still swollen, so no retainer until inspected at follow up visit.
BAD news!!!:
The adjacent teeth has periodontal disease, I don’t really know if Dr Bohannan meant the gum, but he was
talking of resorption/boneloss of the face of the teeth. I think he said he had tried to graft during surgery, but don't know if it would help, it's a hard spot for grafts to stick. If the adjacent teeth aren't holding up, they can't support an implant next to them...The premolar might have to be extracted. What you do after that I don't know. I don't know what a periodontist can do about it.
The 'through-and-through, Dr Bohanan said looked as if a drill had gone through. Tissue had filled the hole, so it had't healed with bone. It's another defect that is hard to fix. I think Dr Bohannan said he tried putting grafting here. It might need more grafting.
Sounded like there is nothing more that can be done now. Just carefully supervise how it heals. A CBCT would be taken in 6 months.Next check-up in 2 weeks.
I asked for the surgery notes to better understand what Dr Bohannan had just told us. The only thing he has is the notes jotted on the side of the form below.
12/22/2017: Postop visit
The good news is it is healing ok. But still swollen, so no retainer until inspected at follow up visit.
BAD news!!!:
The adjacent teeth has periodontal disease, I don’t really know if Dr Bohannan meant the gum, but he was
talking of resorption/boneloss of the face of the teeth. I think he said he had tried to graft during surgery, but don't know if it would help, it's a hard spot for grafts to stick. If the adjacent teeth aren't holding up, they can't support an implant next to them...The premolar might have to be extracted. What you do after that I don't know. I don't know what a periodontist can do about it.
The 'through-and-through, Dr Bohanan said looked as if a drill had gone through. Tissue had filled the hole, so it had't healed with bone. It's another defect that is hard to fix. I think Dr Bohannan said he tried putting grafting here. It might need more grafting.
Sounded like there is nothing more that can be done now. Just carefully supervise how it heals. A CBCT would be taken in 6 months.Next check-up in 2 weeks.
I asked for the surgery notes to better understand what Dr Bohannan had just told us. The only thing he has is the notes jotted on the side of the form below.
1/4/2018: 3 weeks post op, visit Dr Bohannan:
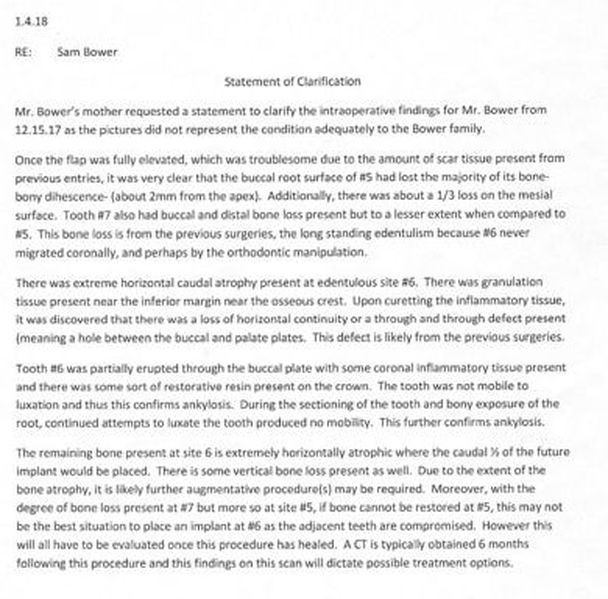
I contacted Dr Bohannan by email, since Sam and I were both kind of stunned and confused by the information at the previous meeting. I had hoped that Dr Bohannan could give me something in writing because the verbal info still left us confused after the visit and it seems unnecessary that we make our own interpretations, especially when reporting to other dental practitioners involved. (Got a new copy of the surgery notes where side wasn't cut off.) However, Dr Bohannan thinks the photos above at surgery says everything: (again, my interpretation)
The bone that is supposed to cover the roots of #7 and #5 has resorbed and is missing to a large degree, worse for the premolar, #5. Allegory, the box that the tooth root is supposed to be anchored by, is missing the front side! Sounds like even if you try repairing it periodontically, the odds are bad, and it’s unlikely that it could support an implant in #6 position, so in the worst scenario you loose both #5 and the implant. There is a risk for infection also that would come with grafting of #5, and infections endangers implants. Alternatively you extract #5 and put in 2 implants. The hole through the palate, “thru and thru” is another complication. It is perfectly round and looks as if made by made by burr.
I contacted Dr Bohannan by email, since Sam and I were both kind of stunned and confused by the information at the previous meeting. I had hoped that Dr Bohannan could give me something in writing because the verbal info still left us confused after the visit and it seems unnecessary that we make our own interpretations, especially when reporting to other dental practitioners involved. (Got a new copy of the surgery notes where side wasn't cut off.) However, Dr Bohannan thinks the photos above at surgery says everything: (again, my interpretation)
The bone that is supposed to cover the roots of #7 and #5 has resorbed and is missing to a large degree, worse for the premolar, #5. Allegory, the box that the tooth root is supposed to be anchored by, is missing the front side! Sounds like even if you try repairing it periodontically, the odds are bad, and it’s unlikely that it could support an implant in #6 position, so in the worst scenario you loose both #5 and the implant. There is a risk for infection also that would come with grafting of #5, and infections endangers implants. Alternatively you extract #5 and put in 2 implants. The hole through the palate, “thru and thru” is another complication. It is perfectly round and looks as if made by made by burr.
|
It seems the ‘thru-and-thru’ fenestration that Dr Bohannan found and says looks like a hole made by burr, matches the gash in the crown on the Anatomage enhanced 2015 CBCT. |
|
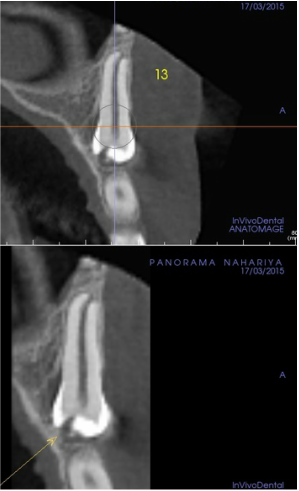
CBCT 2015 enhanced with Anatomage by Dr Becker
|
Dr Bohannan doesn’t want to say anything for sure about a revised treatment plan until the CBCT, 6 months post op.
It is very devastating news, since we have spent so much effort in saving the canine now it looks like we are going to loose two teeth. I know nothing of this kind of bone resorption, only root resorption and the height of the
alveolar bone.
Sam has had some particles of bone grafting coming out, which is supposedly normal, since they ‘overstuff’. Sam still a bit swollen over the grafting area. Small amount of pus coming out, so Sam is put on more antibiotics, amoxicillin/clavulanic acid for 10 days. Back in 2 weeks. Dr Bohannan adjusts the upper retainer so it is not impinging on graft area.
1/4/2018 Dr Giannotti. We continue on to Fremont. Sam has a cleaning (grafting area excepted). He also set up an appointment with Dr Giannotti, since we could not figure out if Dr Bohannan could adjust the retainer, or if Dr Giannotti needed to make a new one.
1/18/2018: Dr Bohannan. Healing looks good, infection cleared. New visit 4 weeks. Dr Bohannan gave Sam documentation of the findings from surgery, even though he thought the photos were enough and that asking for something else is totally superfluous. No mention of the 'thru-and-thru' in the text.
Dehiscence (corrected spelling) explained. Click.
6/19/2018: Bohannan. (Cone beam $ 195)
6 months post bone graft.
CT taken. If the bad news last time was that for an implant to work the premolars had to be taken out too, now it sounded like Dr Bohannan wasn’t into doing an implant at all.
Initially there was no mention that there could be complications, now it sounds like with 4 previous surgery attempts, complications with scar tissue and vascularisation this outcome was to have been expected.
My interpretation of Dr Bohannan:
- Bone graft worked well for the upper part. The lower part failed, but that was to be expected because it went below the bone line for the adjacent teeth. Membrane on the facial part of #5 that was hoped to generate bone did not work.
- An implant tooth now would have to be very long and look bad. Don't know if an implant would work due to the
adjacent teeth. He could try an implant, but don't know if it work. A failing implant could have the neighboring teeth fail.
- The multiple surgeries left scar tissue and compromised vascularisation.
- Alternative would be some type of prosthesis with bridge.
- Next step is to 'take out hardware', that is remove screws that were put in through bone graft. Earliest appointment for that July 3. After that periodontist consultation and prosthetics consultation. Don't know what question they are supposed to answer.
I asked Dr Bohannan what he thinks is the best option for Sam. Answer was that he would not have put him through so many surgeries originally.
I'm hoping we will have more answers soon. Bone grafts, from what I've previously understood, resorb if they don't get an implant. When the site for #6 looses the bone, how does that affect the surrounding teeth. What are the longterm effect of leaving a space in the alveolar ridge?
A year ago, it seemed the end of all this was near, and the implant would be the solution. Dr Lakha, at the time, did predict that a series of bone grafts would be needed, but without explaining what that was based on.
Now there are complications and no clear solution. Heartbreaking.
Given the ‘choices’ of how to proceed, I asked Dr Bohannan what he would chose if it was his son. He just answered he wouldn’t have done so many surgeries. I wish he would have told me what we should have done all along the way...what should we have done at each point of this story...it’s been so disappointing not to have anybody care enough to help Sam get through this.
7/3/18: Dr Bohannan: 'hardware' out.
As requested I got a CD of CBCT and since I had asked about the µSiv, I got a paper with numbers for exposure, dose and voxel size, but nothing on effective dose.
7/10/18: Dr Bohannan. (Limited oral evaluation $195)
Check after taking screw out last time. Came with my husband because we are tryig to understand where Bohannan is. The prosthodontist and periodontist he wants Sam to see, are just for evaluation of a bridge.
As for implant Dr Bohannan cites difficulties with vascularisation, scar tissue, etc. If an implant fails it could endanger neighboring teeth. An implant tooth would be very long. Already gum pulling up over #7. We said we would like a second opinion concerning implant, so we were going to get pictures from him in order for someone else to give their opinion.
Dr Bohannan talked of a 'tunneling' alternative to opening up a flap that would be less traumatic for the implant site, but difficult technically.
Dr B gave me new sheet of paper on the CBCT, it stated ‘effective dose 1.2028 mSv’ which was alarming.
After I compared with CDental’s CBCT effective dose of 160 μSiv, Dr Bohannan wrote back that the ‘effective dose
was 8 μSiv.’
As requested I got a CD of CBCT and since I had asked about the µSiv, I got a paper with numbers for exposure, dose and voxel size, but nothing on effective dose.
7/10/18: Dr Bohannan. (Limited oral evaluation $195)
Check after taking screw out last time. Came with my husband because we are tryig to understand where Bohannan is. The prosthodontist and periodontist he wants Sam to see, are just for evaluation of a bridge.
As for implant Dr Bohannan cites difficulties with vascularisation, scar tissue, etc. If an implant fails it could endanger neighboring teeth. An implant tooth would be very long. Already gum pulling up over #7. We said we would like a second opinion concerning implant, so we were going to get pictures from him in order for someone else to give their opinion.
Dr Bohannan talked of a 'tunneling' alternative to opening up a flap that would be less traumatic for the implant site, but difficult technically.
Dr B gave me new sheet of paper on the CBCT, it stated ‘effective dose 1.2028 mSv’ which was alarming.
After I compared with CDental’s CBCT effective dose of 160 μSiv, Dr Bohannan wrote back that the ‘effective dose
was 8 μSiv.’
7/11/2018, Dr Giannotti. Check-up. #27 needs some gum coverage.
Letter from Dr Bohannan: Sam surgery summary.
After the letter below, I asked about the 'through-and-through'. The response was that it's referred to in paragraph 3: "Once tooth #6 was removed, the fenestration was occluded with autogenous bone...", also noted in "Fig 5. Note unhealthy bone. Horizontally compromised inferiorly. Fenestration repaired. Note periostal thickening."
After the letter below, I asked about the 'through-and-through'. The response was that it's referred to in paragraph 3: "Once tooth #6 was removed, the fenestration was occluded with autogenous bone...", also noted in "Fig 5. Note unhealthy bone. Horizontally compromised inferiorly. Fenestration repaired. Note periostal thickening."
| letter.sam_bower_summary.7.12.18.pdf |
7/18/2018, Dr Pechak, periodontist, Sunnyvale, $ 192
Concerning adjacent teeth Dr P said a little gum recession, nothing too bad, he was not concerned about any mobility, the measurements were pretty good. Root of #7 is a bit short, but it is not a ‘bad‘ tooth, neither is #5. There is a mucogingival defect at #27 that should be taken care of at some point.
The CD shows one screw in bone graft that took, the other screw is sitting in soft tissue. Dr P made a partial treatment plan using the CD showing where an implant should go. There needs to be a 5mm vertical and some lateral augmentation. Bone at base looks good, but at neck there is no bone. Just doing the lateral augmentation would have been easy, but the vertical part is the challenge. Using just particulate is not predictable, or 50/50, so Dr P doesn’t want to do He recommends a Dr Lee who has done none augmentation in similar cases, but he doesn’t do the implant itself. I asked about the dehiscence problem, but sounded like it was not a problem as long as you got the vertical grafting to work.
Dr P thought it preferable to treat as a localized issue, with implant, rather than doing a bridge, which would be a very aggressive, a last resort option, where you have to cut down the adjacent teeth which eventually would fail, and then you would have a domino effect problem with the other teeth.
Concerning adjacent teeth Dr P said a little gum recession, nothing too bad, he was not concerned about any mobility, the measurements were pretty good. Root of #7 is a bit short, but it is not a ‘bad‘ tooth, neither is #5. There is a mucogingival defect at #27 that should be taken care of at some point.
The CD shows one screw in bone graft that took, the other screw is sitting in soft tissue. Dr P made a partial treatment plan using the CD showing where an implant should go. There needs to be a 5mm vertical and some lateral augmentation. Bone at base looks good, but at neck there is no bone. Just doing the lateral augmentation would have been easy, but the vertical part is the challenge. Using just particulate is not predictable, or 50/50, so Dr P doesn’t want to do He recommends a Dr Lee who has done none augmentation in similar cases, but he doesn’t do the implant itself. I asked about the dehiscence problem, but sounded like it was not a problem as long as you got the vertical grafting to work.
Dr P thought it preferable to treat as a localized issue, with implant, rather than doing a bridge, which would be a very aggressive, a last resort option, where you have to cut down the adjacent teeth which eventually would fail, and then you would have a domino effect problem with the other teeth.
| ct_sam_june_2018.pdf |
| pechak_7_18_18.pdf |
7/25/2018, Dr Kevin Consani, periodontist, Burlingame
Dr Consani thinks the implant option would be best for Sam and recommends Dr Lakha.
Dr Consani thinks the implant option would be best for Sam and recommends Dr Lakha.