STANDARDS
The dental profession holds a special position of trust within society. As a consequence, society affords the profession certain privileges that are not available to members of the public-at-large. In return, the profession makes a commitment to society that its members will adhere to high ethical standards of conduct. [...]these standards are embodied in the ADA Principles of Ethics and Code of Professional Conduct (ADA Code).(1)
I wished they'd explain what the 'certain privileges' are.( It's like using the expression 'thank, you for understanding', when one is requesting information or complaining and actually have in no way expressed any 'understanding'.) Unfortunately, I think the above can be translated into the following:
We know that dentistry is a largely unregulated form of healthcare, involving large amounts of money gained by the dental practitioner, and large costs for the patients, with often quite time-consuming and painful procedures that can largely affect the patients quality of life in the immediate and for the rest of their lives. We hope that you, the dental practitioner, are applying high standards when you go about treating your patient, because it is basically up to your personal skill and ethics what your patient will have to live with.
We know that dentistry is a largely unregulated form of healthcare, involving large amounts of money gained by the dental practitioner, and large costs for the patients, with often quite time-consuming and painful procedures that can largely affect the patients quality of life in the immediate and for the rest of their lives. We hope that you, the dental practitioner, are applying high standards when you go about treating your patient, because it is basically up to your personal skill and ethics what your patient will have to live with.
I think most people of my generation have had a dentist look in our mouths, declare something, then proceed to do something, you were not exactly sure what and why, leaving you with a bad feeling afterwards, that something went really wrong. My husband and I went dentist hunting 15 years ago and came to a dentist who declared that all our fillings had to be removed, reason being there was a 99% chance that there was decay underneath, and then he layed out a plan worth $ 5000 or for each of us and years of dental work. We did get a second opinion and saved our time and money.
John Featherstone, dean of the UCSF school of dentistry advocates for fluoride treatment for children as well as adults to prevent cavities, but also says
Cost could also be a factor for dentists. Featherstone and Wendell [Wendell Evans, associate professor of
dentistry at the University of Sydney] say some dentists may be reluctant to embrace the preventive method
because they worry they'll lose money if they do fewer costly procedures.
How is that for ethics!
Cost could also be a factor for dentists. Featherstone and Wendell [Wendell Evans, associate professor of
dentistry at the University of Sydney] say some dentists may be reluctant to embrace the preventive method
because they worry they'll lose money if they do fewer costly procedures.
How is that for ethics!
Orthodontic Ethics, "The Code", and the difference and definition of simply bad work, 'mistreatment' and 'substandard' treatment.
An orthodontist does emergency work on someone else's patient, fixing a bracket, and wire. He also notes that "significant periodontal problems, excessive unremoved bonding material, incorrect bracket placement, and questionable midtreatment mechanics." The parent asks
how long the substitute orthodontist think the whole treatment will take and if "everything looks all right". The article (2) advices what the orthodontist should do in this situation. The 'Code' admonishes dentists to proceed with caution when advising patients of prior care that is not that good, but still not 'substandard' by stating:
"patients should be informed of their present oral health status without disparaging comments about prior services."
"The Code warns us that a difference of opinion as to preferred treatment may not be a justifiable criticism; it may simply represent two doctors who use different, acceptable approaches to treat the same case"
In this case, which the article doesn't deem 'substandard', the orthodontist is supposed to be diplomatic and say that if he was the treating orthodontist, he might take a different approach, and leave it at that.
The reasoning here is that there is no clear right and wrong in orthodontics, there are different ways to get to the same result. All professions do this, the circling of the wagons. (It is very hard to get the Teachers' Union to acknowledge that there are any 'bad' teachers out there.)
From a parental perspective you wonder what the difference is between bad treatment that is going to take more time with a worse result than what could have been and 'substandard'. In this case there are 'periodontal problems', 'incorrect bracket placement' and so forth, it sounds like 'bad treatment' and a 'bad orthodontist' in a layman's ears and you would want to find a 'good orthodontist' instead. According to the code there is a big grey zone as it sounds, the treatment may take longer, the result may not be as good, but that is still acceptable treatment.
So much for second opinions.
When it comes to the Dental Board the bar for negligence is set very high.
An orthodontist does emergency work on someone else's patient, fixing a bracket, and wire. He also notes that "significant periodontal problems, excessive unremoved bonding material, incorrect bracket placement, and questionable midtreatment mechanics." The parent asks
how long the substitute orthodontist think the whole treatment will take and if "everything looks all right". The article (2) advices what the orthodontist should do in this situation. The 'Code' admonishes dentists to proceed with caution when advising patients of prior care that is not that good, but still not 'substandard' by stating:
"patients should be informed of their present oral health status without disparaging comments about prior services."
"The Code warns us that a difference of opinion as to preferred treatment may not be a justifiable criticism; it may simply represent two doctors who use different, acceptable approaches to treat the same case"
In this case, which the article doesn't deem 'substandard', the orthodontist is supposed to be diplomatic and say that if he was the treating orthodontist, he might take a different approach, and leave it at that.
The reasoning here is that there is no clear right and wrong in orthodontics, there are different ways to get to the same result. All professions do this, the circling of the wagons. (It is very hard to get the Teachers' Union to acknowledge that there are any 'bad' teachers out there.)
From a parental perspective you wonder what the difference is between bad treatment that is going to take more time with a worse result than what could have been and 'substandard'. In this case there are 'periodontal problems', 'incorrect bracket placement' and so forth, it sounds like 'bad treatment' and a 'bad orthodontist' in a layman's ears and you would want to find a 'good orthodontist' instead. According to the code there is a big grey zone as it sounds, the treatment may take longer, the result may not be as good, but that is still acceptable treatment.
So much for second opinions.
When it comes to the Dental Board the bar for negligence is set very high.
Sometimes I find 'frustrated comments' from dental professionals on the internet, and I think they express what is not always so clear in the scientific articles. The one below is about impacted canines in adults. That seems to be a problem in itself: Why are there adults with impacted canines? The author explains why he succeeds with
ALL impactions, so why his thinking the gold standard set for handling impacted canines?
ALL impactions, so why his thinking the gold standard set for handling impacted canines?
I think this was beat to death already, but I have my 2 cents on impacted canines on adults. First, there are good published articles on this. Overall, the consensus is under 18 is well over 95% success...over age 18 about 50% success. That is not my experience, however. This will ramble, but I have a point that I think is important about impacted canines on adults. I know there are canines that cannot be brought in. I just have never had that. The canines are always movable...but not always easily. And here is my point. YOU NEED A SURGEON INVOLVED on the treatment planning who you trust and is good. They need to know what you want done and you have to talk to them. Simply referring them to someone is not enough. And the patient has to understand this is a difficult process. It should not take 3-4 years...it's either done quick or not at all. And there are canines that are just not worth the effort. But you need to diagnose the movement and the condition of the canine at each visit. It is not tug tug tug...have your assistant tie it again. You have to do it yourself. As soon as movement is slow, a surgeon needs to go in and loosen it immediately before you beat on the other teeth. I have a specific surgeon that I work with where we have teamed up for "hopeless canines" that other orthos said was hopeless. In the extreme, if you have a badly impacted canine that is ankylosed (and the surgeon should check for ankylosis when exposing the canine on any adult) it needs to be loosened, sometimes to the point of extraction. The patient then has to come to your office immediately and a severe load has to placed on that ankylosed tooth. You need to see them weekly, if not more often. Your office staff has to know the level of importance of getting this patient in. If it was ankylosed, assume it will fuse again if given the chance and aggressively move it. The entire dentition has to prepped for this. It is not like treating a teenager. As he said the first time we did this, "be careful how hard you pull, it may come out". You cannot delegate this stuff. And a laser can be invaluable for chasing tissue out of the way of engaging the chain. And further exposing it. I have seen impacted palatal canines approached from the buccal by a surgeon (did you want to keep this alveolar bone?). I have seen bonded chains on root surfaces...try pulling on that and see how far you get. I have had chains come loose the 1st time traction is applied. With adults, these screw-ups are devastating. Talk flap design and why. Open v. closed. Check for ankylosis. Get them to use a chain with loops large enough to engage. The cone-beam can be valuable, but not necessary. I had a girl whose canines both destroyed the laterals prior to treatment...and then her brother looked about the same and we were debating starting early or waiting. The cone beam let us see whether the laterals were truly in the path of the canines or not, which a pano can't really show. In an adult, the cone beam would mostly be valuable to better understand orientation and surgical feasibility.
(University of Illinois at Chicago http://www.uic.edu/depts/dort/esco2007-60.html)
This kind of reasoning should be standard and text book worthy! Why isn't It? As it is, the success of
bringing an impacted canine to a happy conclusion is up to the individual orthodontist's skill or lack thereof, his/her ability to collaborate with the oral surgeon and willingness to put in the necessary time and effort...Impacted canines should not be left to the conveyor belt operation with assistants doing the work with occasional checks by the orthodontist himself/herself.
(University of Illinois at Chicago http://www.uic.edu/depts/dort/esco2007-60.html)
This kind of reasoning should be standard and text book worthy! Why isn't It? As it is, the success of
bringing an impacted canine to a happy conclusion is up to the individual orthodontist's skill or lack thereof, his/her ability to collaborate with the oral surgeon and willingness to put in the necessary time and effort...Impacted canines should not be left to the conveyor belt operation with assistants doing the work with occasional checks by the orthodontist himself/herself.
The British Royal College of Surgeons (rcseng.ac.uk) sets up guidelines, that are updated from time to time, for their different treatments, there is one for "Management of the Palatally Ectopic Maxillary Canine", and that seems like a good idea. Their 'Management of the Palatally Ectopic Maxillary Canine' (2010), mentions CBCT, but refers to a set of 2008 recommendations, and technology has moved much faster than the guidelines. I guess some lag is good when it comes to setting new standards, but if it is too slow then it has a negative general effect.
The need for logic, planning, analysis
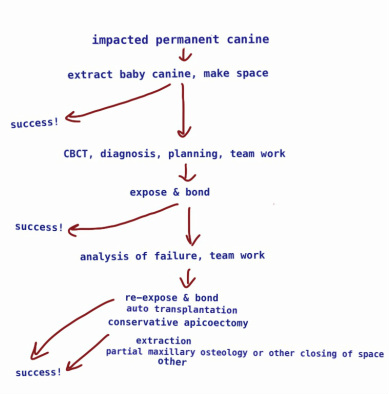
Every case is different, but you should be able to make a basic flow chart for the basic treatment of impacted canines. In children it is very rare that a canine cannot be saved if it is taken care of properly. Every level of treatment needs increased expertise, so along with the flow chart, it would also be appropriate to have a hierarchy of referral.
Every case is different, but you should be able to make a basic flow chart for the basic treatment of impacted canines. In children it is very rare that a canine cannot be saved if it is taken care of properly. Every level of treatment needs increased expertise, so along with the flow chart, it would also be appropriate to have a hierarchy of referral.
|
1-2 % of canines are impacted Some canines descend by themselves when space is opened up by removing the baby tooth. (Dr Kokich recommends surgery for the sole purpose opening up a path for the canine, but without bonding). Surgery should successfully erupt most canines Reasons for failure: 1. poor biomechanical planning of anchorage: wrong direction of force, debonding.. 2. incorrect diagnosis and location and resorption. Undiagnosed ICRR - caused by the first surgery, or idiopathic. PEIR. 3. ankylosis re-surgery should raise the success rate if the reason for failure is analysed. The remaining impacted canines need extra attention!!! |
A Swedish article from 2010 (3) suggest treamtment plans that in some cases use autotransplantation or a premolar in the place of the canine as possible treatments. When the root is developed, it says that a root canal is done after autotransplantation. The periodental ligament needs to be intact (not sure why). If the transplant doesn't work out it still works as a semi-permanent solution, the transplanted tooth functions as a place-holder for a future implant and keeps the bone volume intact.
Even if most canines are good and do erupt just by getting the room to do it, or, at least, do so after an expose & bond, what is the plan when they don't?
Dr Chausu (2) recommends that you test the impacted tooth with the means of a miniscrew (skeletal anchorage)
that is placed in the alveolar bone to see if a tooth is ankylosed or not. That will save time, because you know that you have adequate anchorage for your traction, so that aspect of failure is out of question, and you are not creating an open bite by pulling on other teeth.
There is a risk that the exasperated orthodontist either nervously reaches for the 'extraction, please' referral, or try pulling on the tooth harder:
Subsequent attempts with ever increasing traction forces may provoke periradicular trauma, aggravating the
underlying conditions and leading to ankylosis. Optimal orthodontic force to erupt the impacted teeth might
be as subtle as 50 grams, and preferably not over 150 grams5-7,9,11,15.(1)
If the orthodontist can't analyse cause for failure, it is better the canine is referred to someone with more experience.
Dr Chausu (2) recommends that you test the impacted tooth with the means of a miniscrew (skeletal anchorage)
that is placed in the alveolar bone to see if a tooth is ankylosed or not. That will save time, because you know that you have adequate anchorage for your traction, so that aspect of failure is out of question, and you are not creating an open bite by pulling on other teeth.
There is a risk that the exasperated orthodontist either nervously reaches for the 'extraction, please' referral, or try pulling on the tooth harder:
Subsequent attempts with ever increasing traction forces may provoke periradicular trauma, aggravating the
underlying conditions and leading to ankylosis. Optimal orthodontic force to erupt the impacted teeth might
be as subtle as 50 grams, and preferably not over 150 grams5-7,9,11,15.(1)
If the orthodontist can't analyse cause for failure, it is better the canine is referred to someone with more experience.
This is the 'flow chart' as described by Dr Puricelli:
When orthodontic traction is attempted and does not succeed, even with no clearobservabe obstruction, it is
usually due to apical root dilacerations, improper orthodontic force direction, surgical wire retentions or
ankylosis. When, after six months of orthodontic force application, the tooth does not show clear evidence of
movement, a reevaluation is necessary. Orthodontic planning must be accessed. If the tooth is submerged,
surgical re-intervention is recommended. If the canine's apical third is situated by the Enny's inverted Y or if
signs of apical root dilacerations are visible, an apicotomy, if not yet performed, must be undertaken. If
after all these measures were accounted for with no prognosis of success, radical treatment by means of
extraction is recommended. (1)
When orthodontic traction is attempted and does not succeed, even with no clearobservabe obstruction, it is
usually due to apical root dilacerations, improper orthodontic force direction, surgical wire retentions or
ankylosis. When, after six months of orthodontic force application, the tooth does not show clear evidence of
movement, a reevaluation is necessary. Orthodontic planning must be accessed. If the tooth is submerged,
surgical re-intervention is recommended. If the canine's apical third is situated by the Enny's inverted Y or if
signs of apical root dilacerations are visible, an apicotomy, if not yet performed, must be undertaken. If
after all these measures were accounted for with no prognosis of success, radical treatment by means of
extraction is recommended. (1)
Another of my "frustrated commentators" writes:
Traction needs to be continuous and renewed every two weeks. If eruption has not occurred in 4 months,
another exposure should be performed to remove scar tissue, expand the path of eruption created through
cortical bone, ascertain possible interference with adjacent roots, and, it is hoped, leave the impacted tooth
uncovered.(2)
Traction needs to be continuous and renewed every two weeks. If eruption has not occurred in 4 months,
another exposure should be performed to remove scar tissue, expand the path of eruption created through
cortical bone, ascertain possible interference with adjacent roots, and, it is hoped, leave the impacted tooth
uncovered.(2)
Standards and 'academic vs. clinical' dentistry
A Swedish study (4) that wanted to "document and analyze factors involved in decision-making by orthodontists in managing disturbances of eruption of maxillary canines" came to the conclusion that "the lack of consensus
[after seeing the results of CBCTs] among specialist orthodontists can have negative implications for patients."
From talking to all these dental professionals around Sam's case I've noticed that there is an 'academic' and a 'clinical' version of dental care. The purely 'clinical' professionals who are nor involved in writing papers or talk at conferences (though I suspect they have to participate in some kind of furthering education) are sceptical of the
'academics' and base their decisions on personal experience and 'gut feeling', while the 'academics' (whom I'm supposing can't escape actual patients even if they wanted to) get engrossed in the finer points of treatment.
A Swedish study (4) that wanted to "document and analyze factors involved in decision-making by orthodontists in managing disturbances of eruption of maxillary canines" came to the conclusion that "the lack of consensus
[after seeing the results of CBCTs] among specialist orthodontists can have negative implications for patients."
From talking to all these dental professionals around Sam's case I've noticed that there is an 'academic' and a 'clinical' version of dental care. The purely 'clinical' professionals who are nor involved in writing papers or talk at conferences (though I suspect they have to participate in some kind of furthering education) are sceptical of the
'academics' and base their decisions on personal experience and 'gut feeling', while the 'academics' (whom I'm supposing can't escape actual patients even if they wanted to) get engrossed in the finer points of treatment.
(1) Edela Puricelli. Partial maxillary apicotomy following an unsuccessful forced eruption of an impacted
maxillary canine. J Appl Oral Sci. 2012 Nov-Dec: 20(6): 667-672.
(2) Chaushu S, Chaushu G. Skeletal Implant Anchorage in the Treatment of Impacted Teeth -
A Review of the State of the Art. Seminars in Orthodontics, Vol 16, No 3 (September),
2010: pp 234-241.
(3) Swedish dental journal: http://www.tandlakartidningen.se/media/3255958/andersson_wannfors_10.pdf
(4) Bjerklin K, Bondemark L. Management of ectopic maxillary canines: variations among orthodontists. Angle
Orthod. 2008 Sep; 78(5):852-9.doi 10.2319/070307-306.1.
(5) http://www.npr.org/sections/health-shots/2016/03/14/469959427/no-drill-dentistry-fluoride-treatments-
can-prevent-cavities-in-adults
maxillary canine. J Appl Oral Sci. 2012 Nov-Dec: 20(6): 667-672.
(2) Chaushu S, Chaushu G. Skeletal Implant Anchorage in the Treatment of Impacted Teeth -
A Review of the State of the Art. Seminars in Orthodontics, Vol 16, No 3 (September),
2010: pp 234-241.
(3) Swedish dental journal: http://www.tandlakartidningen.se/media/3255958/andersson_wannfors_10.pdf
(4) Bjerklin K, Bondemark L. Management of ectopic maxillary canines: variations among orthodontists. Angle
Orthod. 2008 Sep; 78(5):852-9.doi 10.2319/070307-306.1.
(5) http://www.npr.org/sections/health-shots/2016/03/14/469959427/no-drill-dentistry-fluoride-treatments-
can-prevent-cavities-in-adults