Part 6: Dr Lakha and Dr Beck: The long (and expensive) road to an implant
Visit Feb 23rd, 2015, Dr Azeem Lakha, oral surgeon, Palo Alto
($250)
Dr Lakha's observations: Sam is lacking 70-80% of bone mass where #6 should be. Mentioned in passing, Sam could loose all his front teeth (!!!). Sam is a complicated case, needs prosthodontist, only three competent enough locally. Info on platelets with growth hormones for the bone graft.
Dr Lakha's plan: CBCT, extract #6, extract all the wisdom teeth (they are headed the wrong way anyway, according to Dr Lakha) in the same session take bone from wisdom teeth are and graft defect and add a platelet cocktail of growth enzymes. Put in implant after bone graft healed.
No concerns about Sam's age for implant...we can do it now, at 17, or wait till Sam is 23 to be sure all facial growth is done with. Dr Lakha doesn't see any advantage in waiting. Since Sam already has a cephalogram from July 2014, we could do another one, but doesn't sound like the result would make much of a difference. (Should be done at the same lab for better comparison.)
($250)
Dr Lakha's observations: Sam is lacking 70-80% of bone mass where #6 should be. Mentioned in passing, Sam could loose all his front teeth (!!!). Sam is a complicated case, needs prosthodontist, only three competent enough locally. Info on platelets with growth hormones for the bone graft.
Dr Lakha's plan: CBCT, extract #6, extract all the wisdom teeth (they are headed the wrong way anyway, according to Dr Lakha) in the same session take bone from wisdom teeth are and graft defect and add a platelet cocktail of growth enzymes. Put in implant after bone graft healed.
No concerns about Sam's age for implant...we can do it now, at 17, or wait till Sam is 23 to be sure all facial growth is done with. Dr Lakha doesn't see any advantage in waiting. Since Sam already has a cephalogram from July 2014, we could do another one, but doesn't sound like the result would make much of a difference. (Should be done at the same lab for better comparison.)
Visit March 5th, 2015 (one-year-anniversary of Dr Becker's surgery!),
Dr Donald Beck, prosthodontist, San Mateo
($280)
Long discussion on pros and cons. The advantages of implants, the technique developed by Dr Brånemark, the
procedures and what the timeline is going to be.
Plan: get mold & CBCT
Dr Donald Beck, prosthodontist, San Mateo
($280)
Long discussion on pros and cons. The advantages of implants, the technique developed by Dr Brånemark, the
procedures and what the timeline is going to be.
Plan: get mold & CBCT
March 12: For the mold we need to go to DR Kai's office first an remove the archwires.
Each drive one hour, so full day on the road.
Drive to Dr Kai's office
Dental assistant removed the archwire (Dr Kai came and said "only the lower". Confusion. )
Drive to Dr Beck
($ 560)
- New patient exam (head and neck cancer examination: soft tissue examination and periodontal charting; TMJ and muscle examination; charting of existing teeth, restoration and caries; functional occlusion examination)
- Mold, old fashioned kind (not Dr Kai's 'wand').
Sam asked about gum around #27 that he feels is irritated. Dr Beck gave advice on using prescription fluoride, Prevident.
Drive to Dr Kai,
Putting back archwire.
For some reason Sam now has the elastic back.
Dr Kai has spoken with Dr Lakha, but not Dr Beck, this is what he thinks we are doing:
- Extract #6, bone graft
- Complete orthodontic therapy & remove braces (Dr Kai)
- Place retainer
- Place a temporary prosthesis (Maryland bridge?) (Dr Beck)
- Make new upper retainer with temporary prosthesis in place. (Dr Kai)
- Take serial cephs to monitor growth until no growth
- Place bone graft at implant site if needed 6 mo prior to implant
- Place implant and crown (Dr Beck)
- Place new upper retainer with implant crown (Dr Kai)
The alternative of extracting #6 and moving the lateral teeth to fill the space, Dr Kai says would take too long,
1 1/2 year.
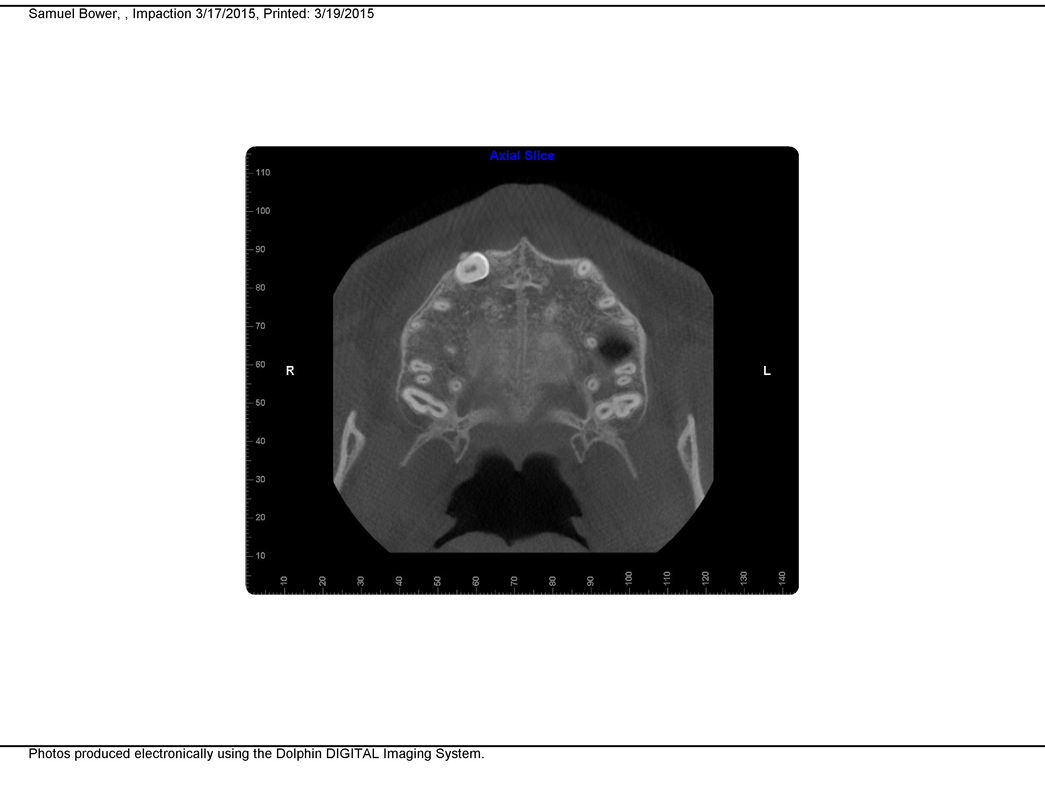
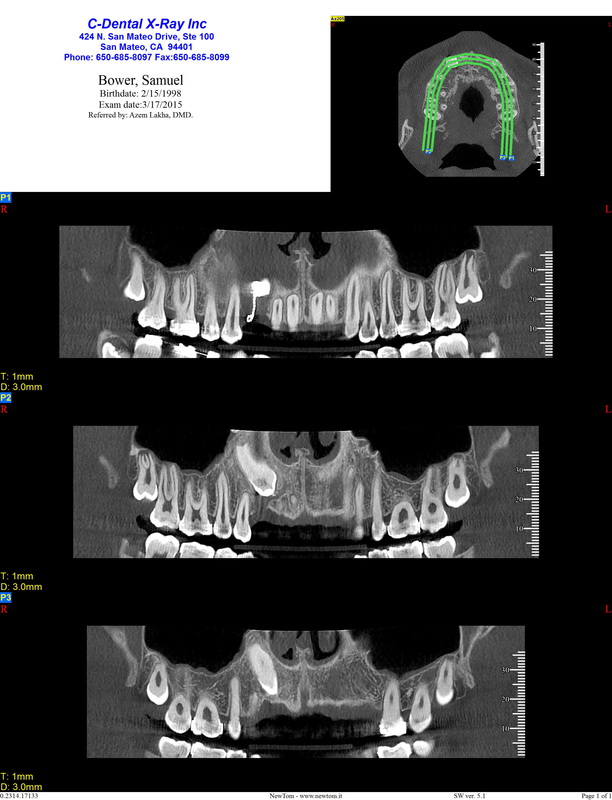
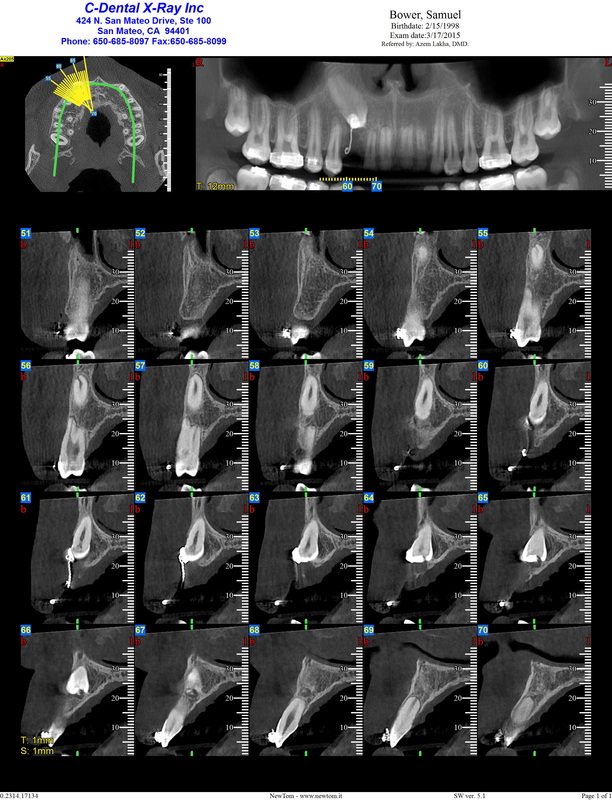
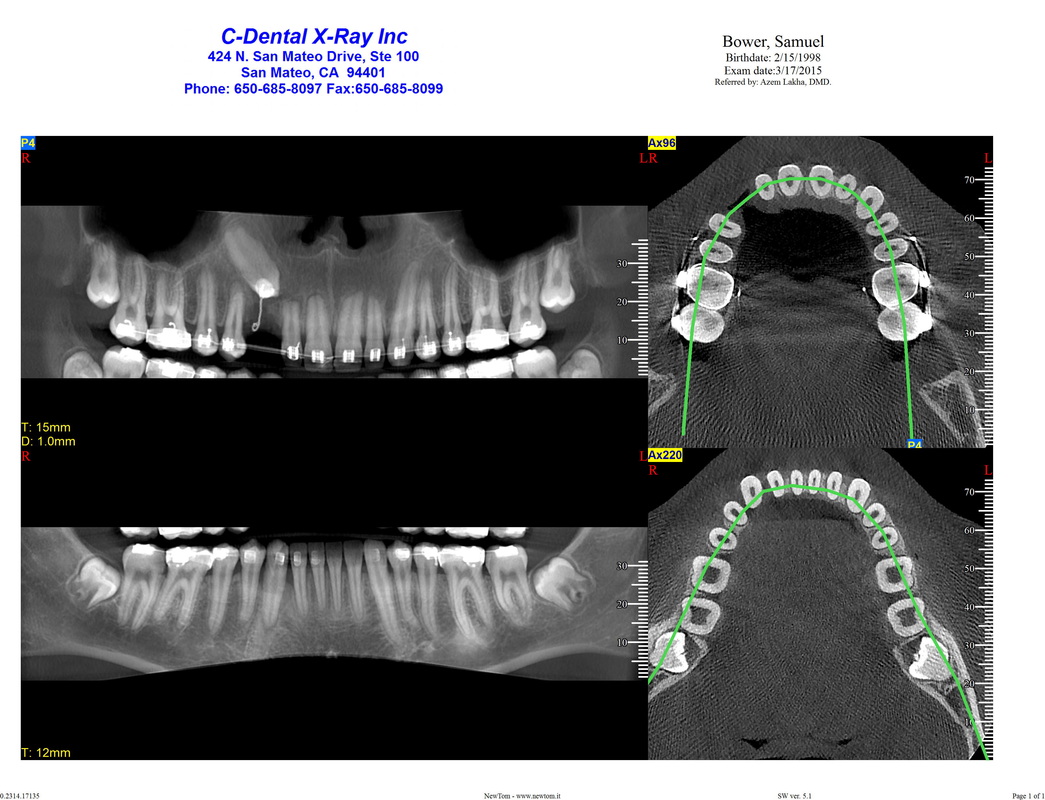
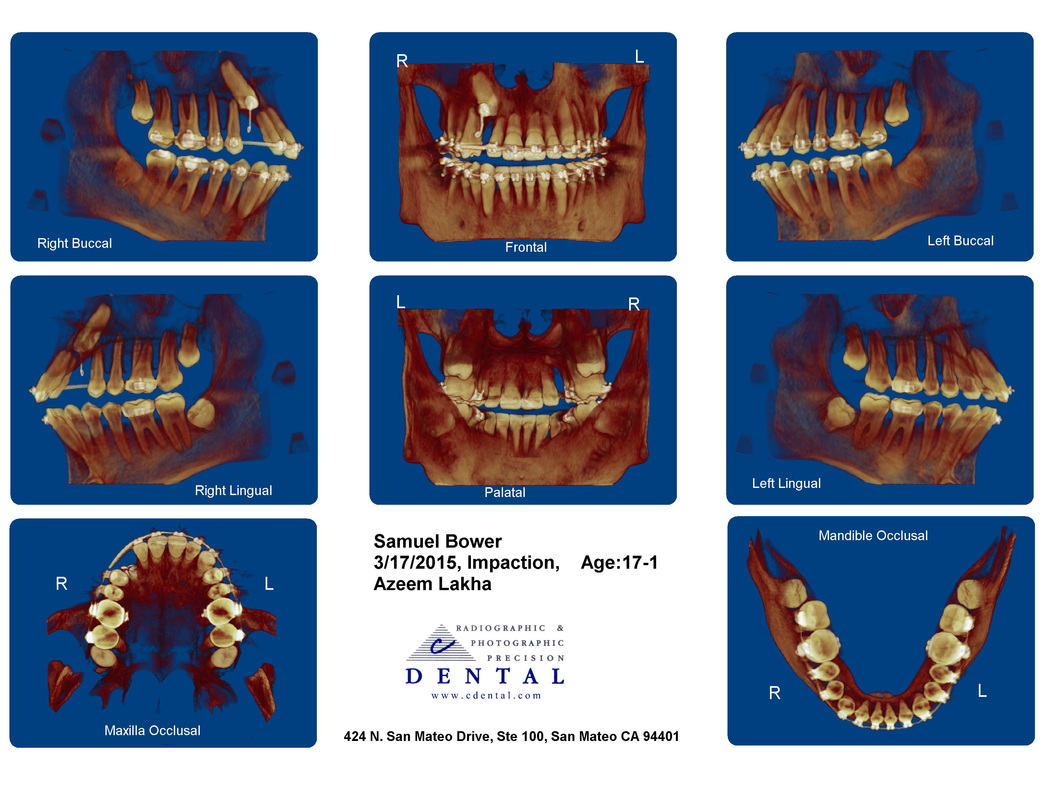
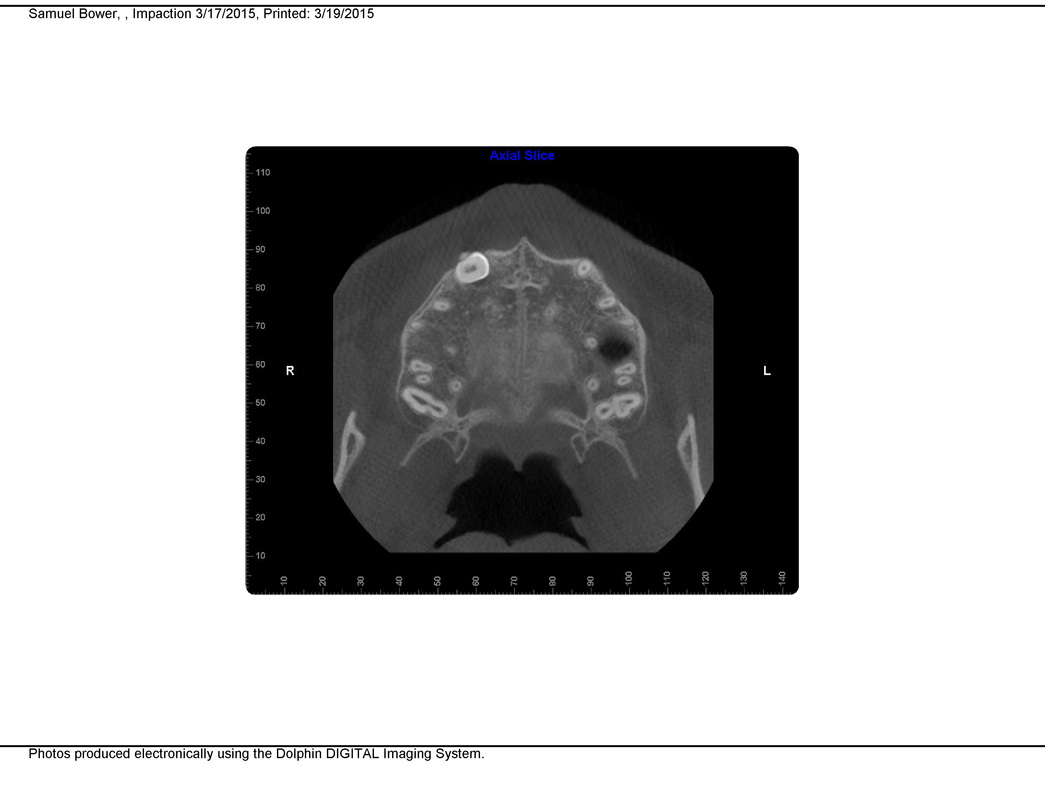
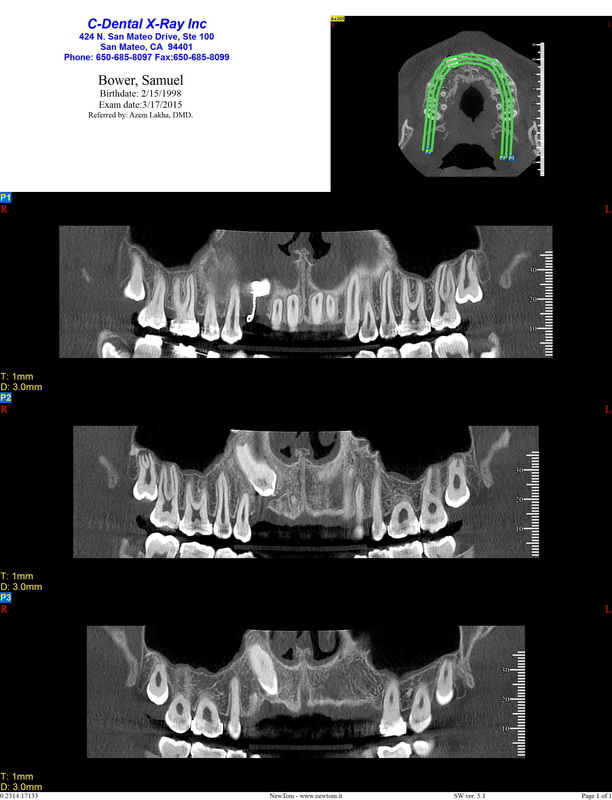
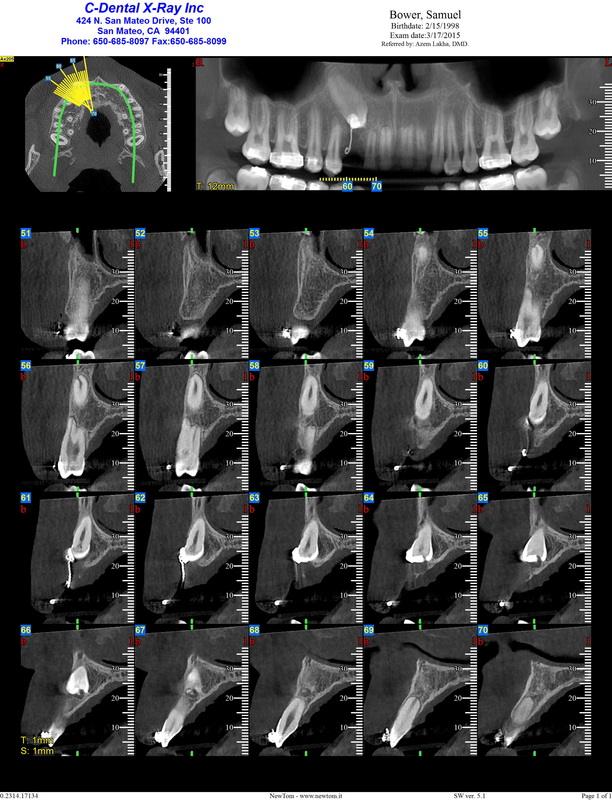
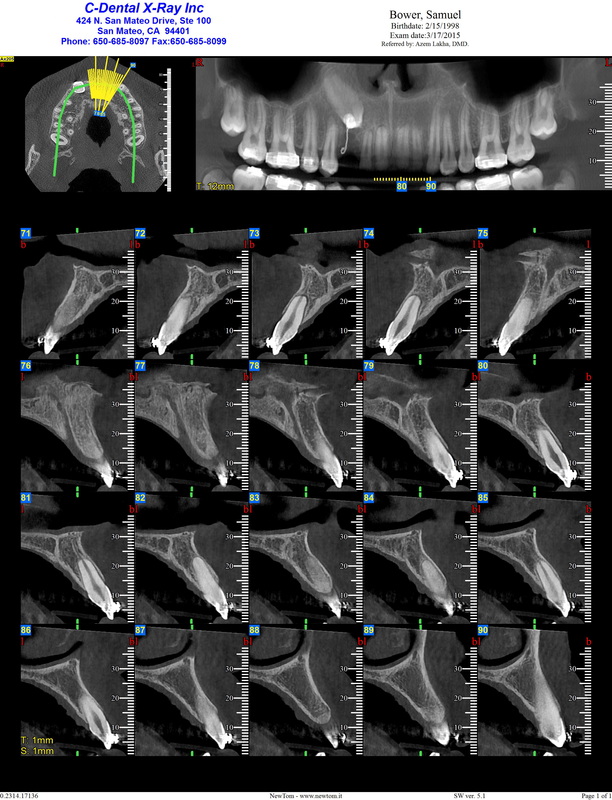
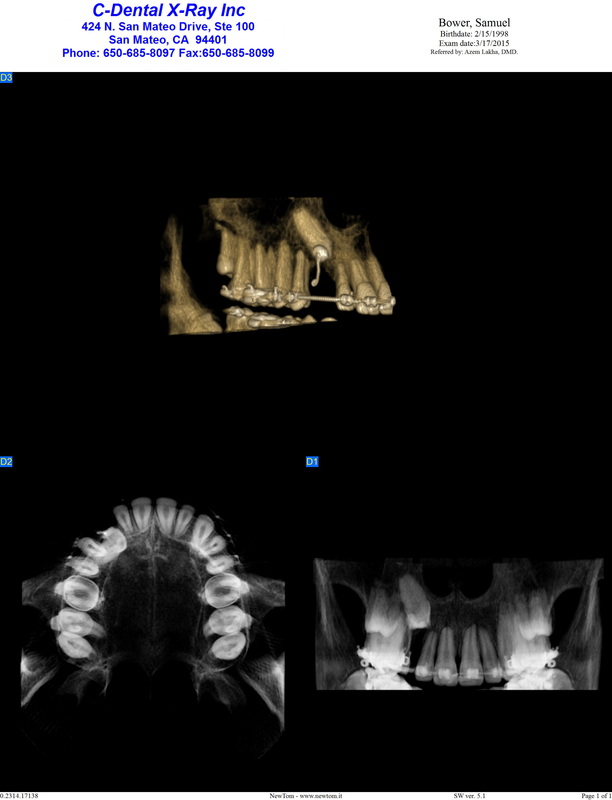
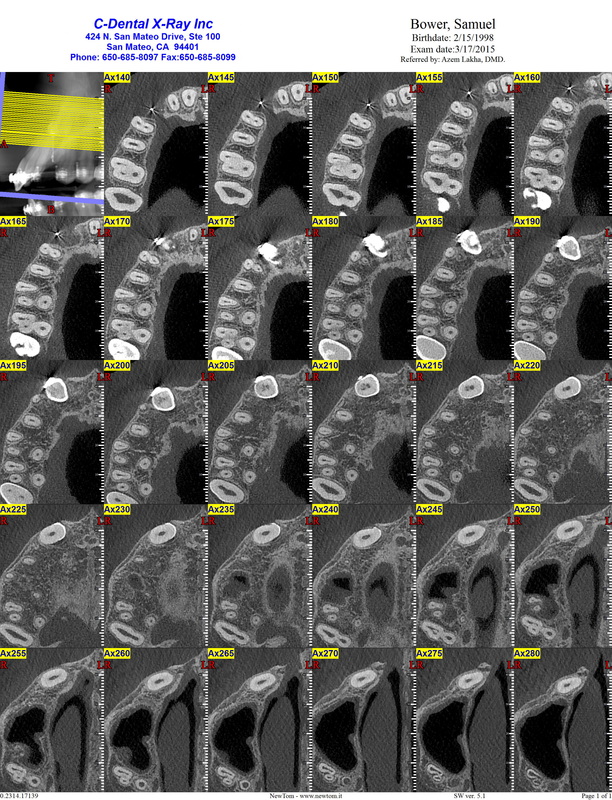
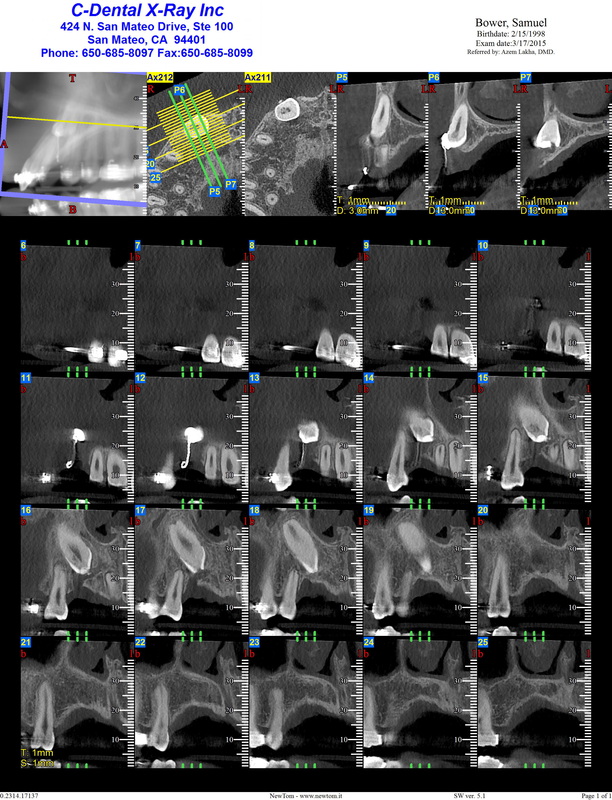
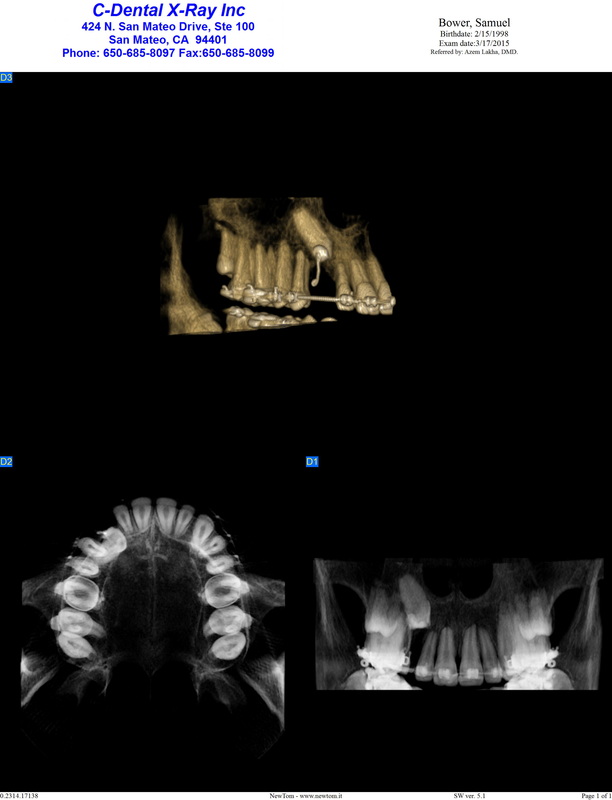
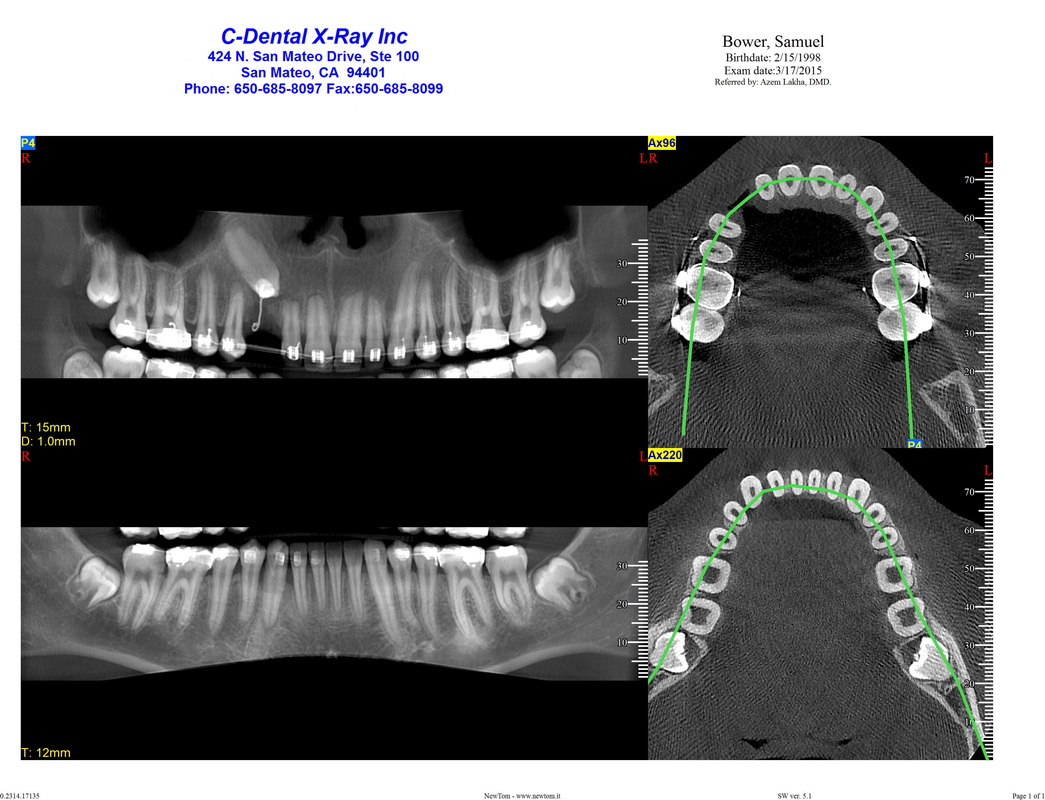
March 17:
($ 375)
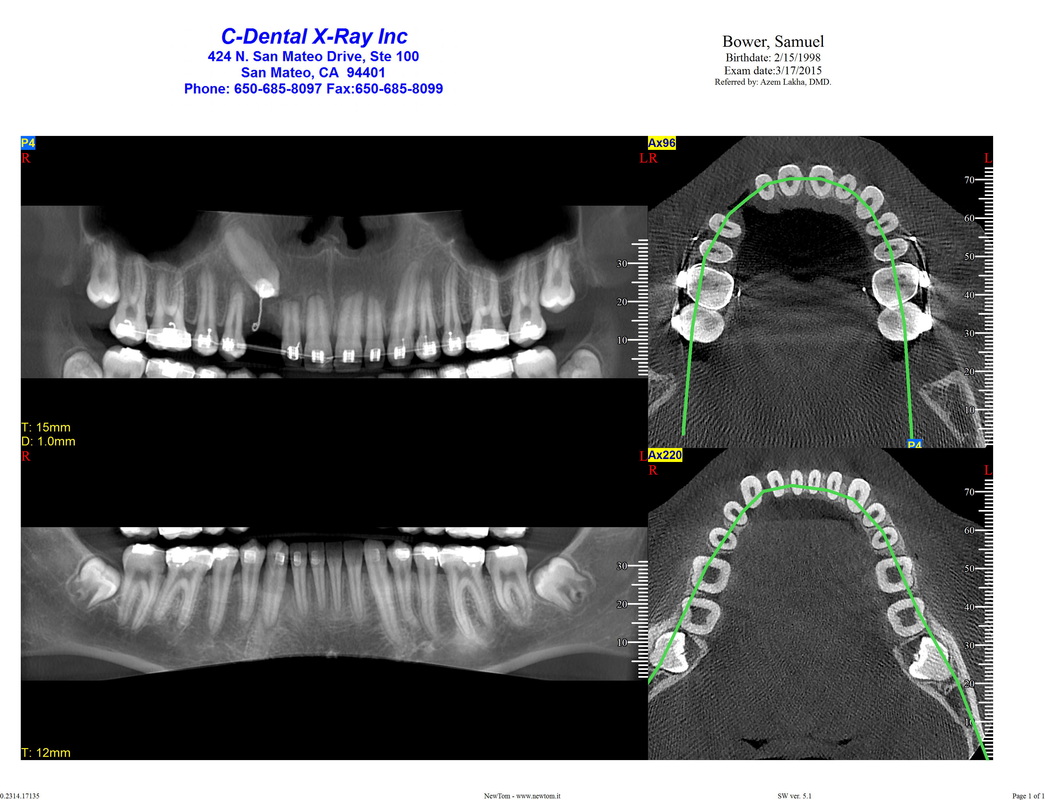
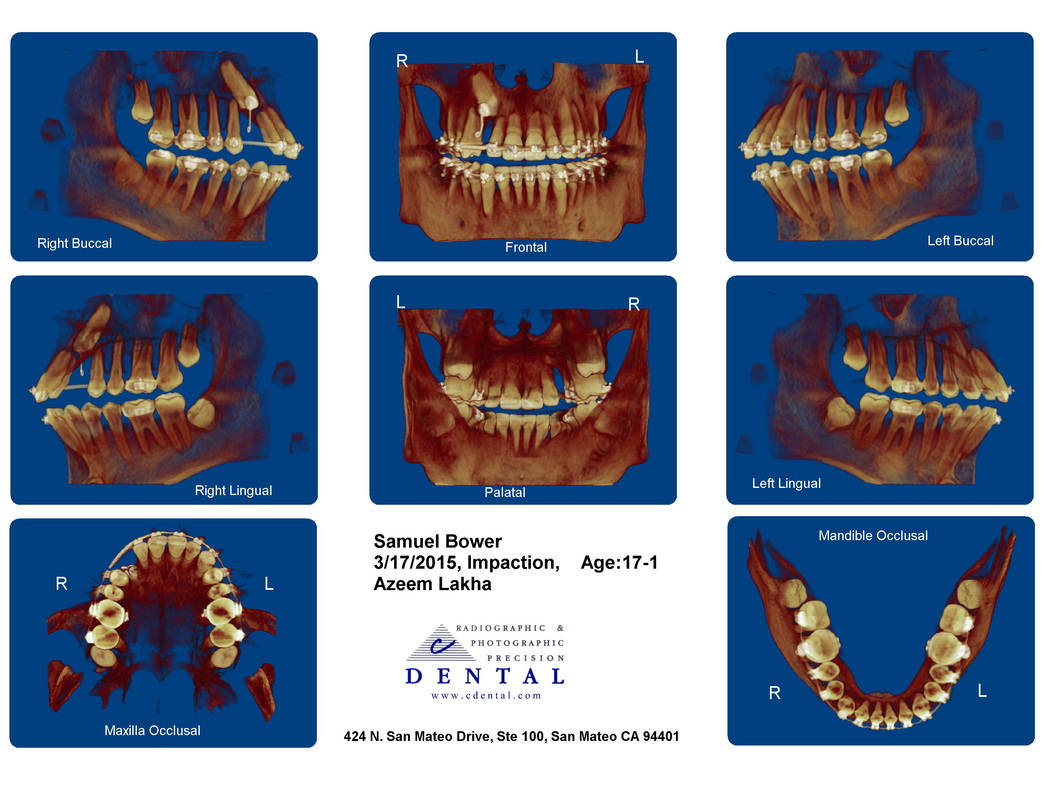
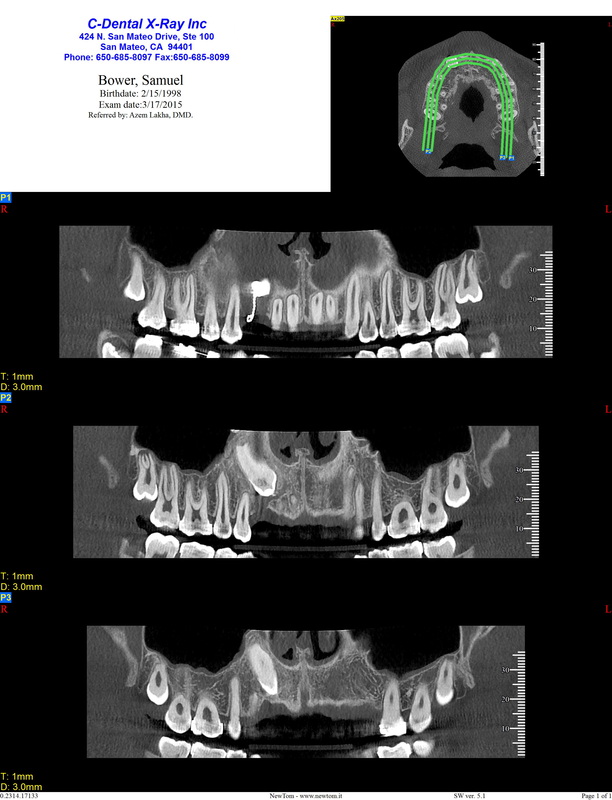
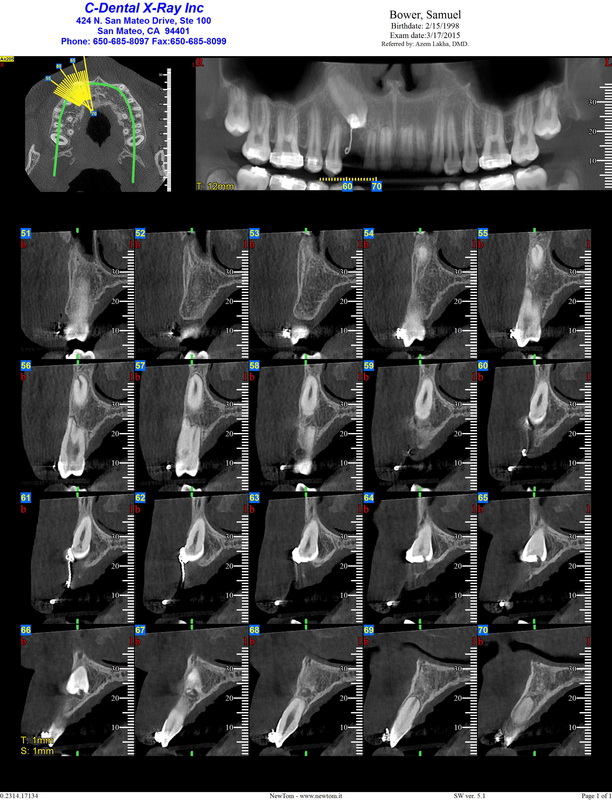
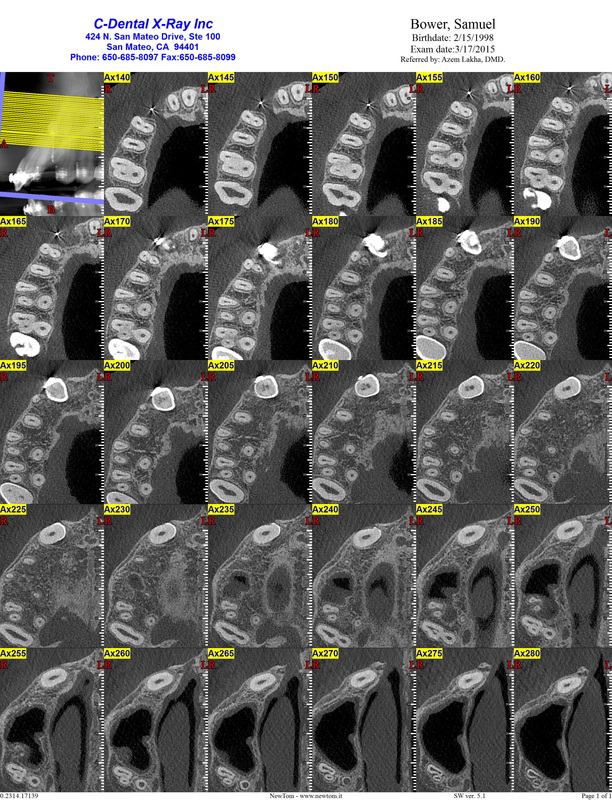
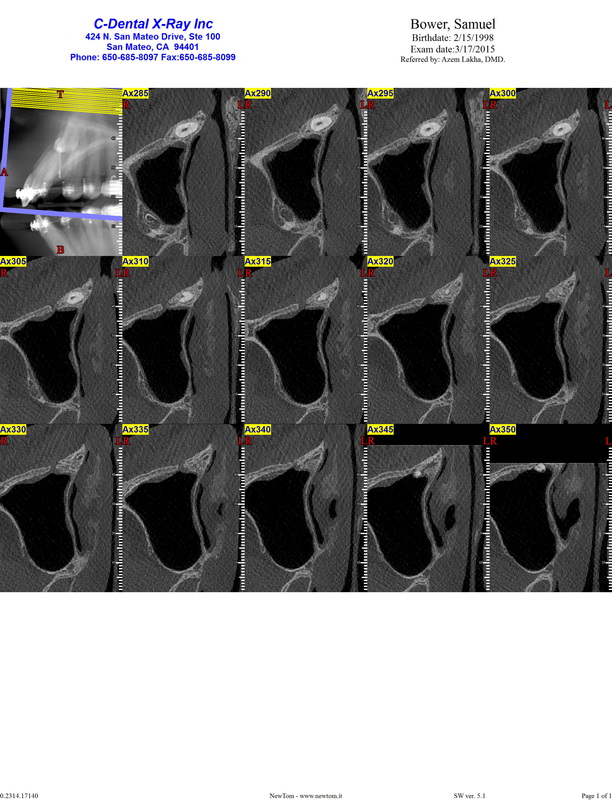
CBCT #3, at C Dental San Mateo
They use high resolution 12 x 8 scan which gives 160 µSiv (Cf previous CBCTs with 25 µSiv and 15 µSiv)
(A 'large scan' CBCT takes 52 µSiv at C Dental)
Each drive one hour, so full day on the road.
Drive to Dr Kai's office
Dental assistant removed the archwire (Dr Kai came and said "only the lower". Confusion. )
Drive to Dr Beck
($ 560)
- New patient exam (head and neck cancer examination: soft tissue examination and periodontal charting; TMJ and muscle examination; charting of existing teeth, restoration and caries; functional occlusion examination)
- Mold, old fashioned kind (not Dr Kai's 'wand').
Sam asked about gum around #27 that he feels is irritated. Dr Beck gave advice on using prescription fluoride, Prevident.
Drive to Dr Kai,
Putting back archwire.
For some reason Sam now has the elastic back.
Dr Kai has spoken with Dr Lakha, but not Dr Beck, this is what he thinks we are doing:
- Extract #6, bone graft
- Complete orthodontic therapy & remove braces (Dr Kai)
- Place retainer
- Place a temporary prosthesis (Maryland bridge?) (Dr Beck)
- Make new upper retainer with temporary prosthesis in place. (Dr Kai)
- Take serial cephs to monitor growth until no growth
- Place bone graft at implant site if needed 6 mo prior to implant
- Place implant and crown (Dr Beck)
- Place new upper retainer with implant crown (Dr Kai)
The alternative of extracting #6 and moving the lateral teeth to fill the space, Dr Kai says would take too long,
1 1/2 year.
March 17:
($ 375)
CBCT #3, at C Dental San Mateo
They use high resolution 12 x 8 scan which gives 160 µSiv (Cf previous CBCTs with 25 µSiv and 15 µSiv)
(A 'large scan' CBCT takes 52 µSiv at C Dental)










March 23: Dr Lakha & Dr Beck conference
March 31: Visit Dr Beck
Dr Beck spent two hours with us explaining and answering questions.
Dr Beck said the CBCT was very informative. #6 is not causing root resorption where it is now, but the roots of the 4 upper incisors have been shortened, as happens after lengthy orthodontic treatments.
After bone graft there is a 3-6 months window for the implant to be placed. After 6 months, without the stimulation of a tooth, the graft will tend to resorb.
An implant is a one-time effort, you don't want to try to extract an implant. If the maxilla does any growth that changes the placement of the implant, you have to live with it. Dr Beck leaning towards giving Sam a break with braces and operations. Would be wearing removable retainer with fake tooth (preferable to 'Maryland bridge') until ready for operation. To wait is not going to cause any more bone resorption since the bone over the tooth is already gone. The orthodontic work needs to prepare for an implant such that the implant doesn't have to bear the force and strains that a natural canine has to. Dr Beck would discuss this with Dr Kai. (The strain on a tooth in the canine position is also a reason why premolar can't be moved to take a canine's place.)
To extract and move the lateral teeth to fill the space, is not a good solution, since a premolar can't fill the function or hold up to the forces a canine has to deal with. To make the implant work as a canine, the orthodontics has to be changed to accommodate it. Also concerns about the temporomandibular joint.
Dr Beck sounded pessimistic about giving Sam a 'perfect smile'. Sam wants a functional and OK smile, he is not picky at this point.
(As Sam said afterward he doesn't really think a 'break' from braces feels really like a brake as long as he knows that there is more to come.)
March 6: Visit Dr Lakha
($ 175 - oral evaluation)
Dr Lakha doesn't see any advantage in delaying surgery. He wants to pull all 4 wisdom teeth and use the bone underneath for grafts. He thinks it is probably going to take 2 or 3 bone grafts, each time with general anesthesia. The window for putting in the implant, would be up to 9 months after the final graft?
Again, no advantage to wait, can't be sure if there will be a growth spurt at age 23 anyway in Dr Lakha's view, but could do cephalogram.
Sounds like the expected lifetime of the implant would be 20 years, so with a 80-year-lifespan, Sam is in for 3 of these extract & graft & implant, the really depressing downside with implants in children.
(As we haven't seen the financial person yet, the amount of $$$ for the whole enterprise is still an unknown.)
March 27: Requested visit Dr Kai
Sam lost a molar bracket; also the UR3 was being twisted inward by the bracket, the dental assistant looked a bit worried when she went to get Dr Kai. Dr Kai took old-fashioned molds to compare with Dr Beck's findings and recommendations. Dr Kai's recommendation leans towards waiting for implant until Sam is 19, 20...
May 14, 2015: Dr Kai
Put substantial rain into the Bay Area commute equation, and a one-hour-drive turned into almost 2 and a half.
Dr Kai's recommendation is to wait with implant a couple of years, sounded like he thought that a graft could be done before that in one session. I asked about the four upper front incisors and Dr Lakha's statement that they could be lost. Dr Kai first wanted to remember how long we had been with him, he suggested since Christmas.
(I would have thought 'Sam's case' would have been more memorable than that. We saw Dr Kai July 15, 2014 and had the apicotomy on September 15, 2014. It took quite long after that to get #27 finally fixed and an oral surgeon.)
Dr Kai said the roots were a bit shortened, but covered with bone so he saw no risk of that. He didn't see any indication to remove the wisdom teeth per se. He considers his orthodontial work completed, except for minor tweaks according to Dr Beck's specifications.
(I sent Dr Kai the 2D CBCT images; he has not received the DICOM, but doesn't understand how to use the 3D
function so he isn't interested in that. Quite disappointing.)
March 31: Visit Dr Beck
Dr Beck spent two hours with us explaining and answering questions.
Dr Beck said the CBCT was very informative. #6 is not causing root resorption where it is now, but the roots of the 4 upper incisors have been shortened, as happens after lengthy orthodontic treatments.
After bone graft there is a 3-6 months window for the implant to be placed. After 6 months, without the stimulation of a tooth, the graft will tend to resorb.
An implant is a one-time effort, you don't want to try to extract an implant. If the maxilla does any growth that changes the placement of the implant, you have to live with it. Dr Beck leaning towards giving Sam a break with braces and operations. Would be wearing removable retainer with fake tooth (preferable to 'Maryland bridge') until ready for operation. To wait is not going to cause any more bone resorption since the bone over the tooth is already gone. The orthodontic work needs to prepare for an implant such that the implant doesn't have to bear the force and strains that a natural canine has to. Dr Beck would discuss this with Dr Kai. (The strain on a tooth in the canine position is also a reason why premolar can't be moved to take a canine's place.)
To extract and move the lateral teeth to fill the space, is not a good solution, since a premolar can't fill the function or hold up to the forces a canine has to deal with. To make the implant work as a canine, the orthodontics has to be changed to accommodate it. Also concerns about the temporomandibular joint.
Dr Beck sounded pessimistic about giving Sam a 'perfect smile'. Sam wants a functional and OK smile, he is not picky at this point.
(As Sam said afterward he doesn't really think a 'break' from braces feels really like a brake as long as he knows that there is more to come.)
March 6: Visit Dr Lakha
($ 175 - oral evaluation)
Dr Lakha doesn't see any advantage in delaying surgery. He wants to pull all 4 wisdom teeth and use the bone underneath for grafts. He thinks it is probably going to take 2 or 3 bone grafts, each time with general anesthesia. The window for putting in the implant, would be up to 9 months after the final graft?
Again, no advantage to wait, can't be sure if there will be a growth spurt at age 23 anyway in Dr Lakha's view, but could do cephalogram.
Sounds like the expected lifetime of the implant would be 20 years, so with a 80-year-lifespan, Sam is in for 3 of these extract & graft & implant, the really depressing downside with implants in children.
(As we haven't seen the financial person yet, the amount of $$$ for the whole enterprise is still an unknown.)
March 27: Requested visit Dr Kai
Sam lost a molar bracket; also the UR3 was being twisted inward by the bracket, the dental assistant looked a bit worried when she went to get Dr Kai. Dr Kai took old-fashioned molds to compare with Dr Beck's findings and recommendations. Dr Kai's recommendation leans towards waiting for implant until Sam is 19, 20...
May 14, 2015: Dr Kai
Put substantial rain into the Bay Area commute equation, and a one-hour-drive turned into almost 2 and a half.
Dr Kai's recommendation is to wait with implant a couple of years, sounded like he thought that a graft could be done before that in one session. I asked about the four upper front incisors and Dr Lakha's statement that they could be lost. Dr Kai first wanted to remember how long we had been with him, he suggested since Christmas.
(I would have thought 'Sam's case' would have been more memorable than that. We saw Dr Kai July 15, 2014 and had the apicotomy on September 15, 2014. It took quite long after that to get #27 finally fixed and an oral surgeon.)
Dr Kai said the roots were a bit shortened, but covered with bone so he saw no risk of that. He didn't see any indication to remove the wisdom teeth per se. He considers his orthodontial work completed, except for minor tweaks according to Dr Beck's specifications.
(I sent Dr Kai the 2D CBCT images; he has not received the DICOM, but doesn't understand how to use the 3D
function so he isn't interested in that. Quite disappointing.)
Done Growing?
At least height wise Sam doesn't appear to be done:
June 30, 2015 193.4 cm
May 20, 2015 192.2 cm
Oct 14, 2014 189.0 cm
April, 2014 187.6 cm
Feb 17, 2014 183.8 cm
At least height wise Sam doesn't appear to be done:
June 30, 2015 193.4 cm
May 20, 2015 192.2 cm
Oct 14, 2014 189.0 cm
April, 2014 187.6 cm
Feb 17, 2014 183.8 cm
June 30, 2015: Dr Beck
Long 'therapy' session with Dr Beck. Dr Beck is very generous with his time in order to make us understand the procedure and answer any questions after putting them through Dr Lakha. I am afraid he has to deal with the frustration that all our previous experiences have resulted in.
Dr Beck will coordinate with Dr Lakha and Dr Kai and make a treatment plan.
July 3, 2015: Dr Kai
Dr Beck was going to contact Dr Beck about some adjustments, but Dr Kai hadn't heard from him, but thought that he knew what Dr Beck wants. Sam is back in rubber bands which is no fun for him.
Long 'therapy' session with Dr Beck. Dr Beck is very generous with his time in order to make us understand the procedure and answer any questions after putting them through Dr Lakha. I am afraid he has to deal with the frustration that all our previous experiences have resulted in.
Dr Beck will coordinate with Dr Lakha and Dr Kai and make a treatment plan.
July 3, 2015: Dr Kai
Dr Beck was going to contact Dr Beck about some adjustments, but Dr Kai hadn't heard from him, but thought that he knew what Dr Beck wants. Sam is back in rubber bands which is no fun for him.

1/8" heavy
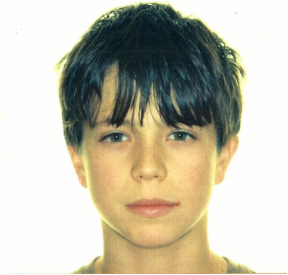
Ortho image of face. Sam almost 13, just before starting braces in 2011,
the beginning of this 'impacted canine' story',
A dental version of 'Boyhood'.
|

1/4" medium

Sam now at 17 1/2 years. Almost done with braces, but at the start of extraction, grafting, implant...
|

another round of rubber bands

(Crazy hair, due to a wrestling team ploy to have everyone blond 6 months ago)
|
July 13, 2015: Dr Lakha
$ 175
Dr Lakha wants to extract #6 and put in a preliminary bone graft now. This would not be time dependent and the graft would not resorb if an implant did not follow immediately. He wants to get rid of the chain that could allow bacteria to get in. We'll do a cephalogram now and in 6 months to compare growth.
Dr Beck and Dr Kai have recommended Sam taking a brake. The braces are coming of in two or three months when Dr Beck has his final adjustments, instead there will be a retainer with a fake tooth, but after 5 years of braces it will be a nice change I'm hoping.
Sam is not too keen on having all his molars and #6 pulled out right now. He is going on a trip (we are trying to make up for last year's abominable summer of me being in Sam's face, literally, and seeing a bunch of 'nice', but unhelpful orthodontists) now before school starts up again, and he is very into windsurfing and wrestling, and would like to wait until sometime next spring. Sam's worry is that with the gap his upper arch doesn't have the
same stability as an intact arch, and that he could get punched in the mouth doing his sports. Dr Lakha said that
it wasn't an issue, the teeth are not more vulnerable because of the gap.
Dr Lakha's argument is that the wisdom teeth are easier to pull the younger the patient, before they start growing into the nerves, they are growing in the wrong direction anyway. As he says, Sam can do what he wants, live, as they do in third world countries with a gap, and do nothing; or do what Dr Lakha recommends. There are
consequences with surgery and without surgery.
Good news is that Dr Lakha says he never said that the front teeth were in danger of falling out, and that given
Sam's age and good health he should bounce back quickly after the extraction of #6 and wisdom teeth.
In the end, Dr Lakha seemed OK with Sam taking his time a bit.
$ 175
Dr Lakha wants to extract #6 and put in a preliminary bone graft now. This would not be time dependent and the graft would not resorb if an implant did not follow immediately. He wants to get rid of the chain that could allow bacteria to get in. We'll do a cephalogram now and in 6 months to compare growth.
Dr Beck and Dr Kai have recommended Sam taking a brake. The braces are coming of in two or three months when Dr Beck has his final adjustments, instead there will be a retainer with a fake tooth, but after 5 years of braces it will be a nice change I'm hoping.
Sam is not too keen on having all his molars and #6 pulled out right now. He is going on a trip (we are trying to make up for last year's abominable summer of me being in Sam's face, literally, and seeing a bunch of 'nice', but unhelpful orthodontists) now before school starts up again, and he is very into windsurfing and wrestling, and would like to wait until sometime next spring. Sam's worry is that with the gap his upper arch doesn't have the
same stability as an intact arch, and that he could get punched in the mouth doing his sports. Dr Lakha said that
it wasn't an issue, the teeth are not more vulnerable because of the gap.
Dr Lakha's argument is that the wisdom teeth are easier to pull the younger the patient, before they start growing into the nerves, they are growing in the wrong direction anyway. As he says, Sam can do what he wants, live, as they do in third world countries with a gap, and do nothing; or do what Dr Lakha recommends. There are
consequences with surgery and without surgery.
Good news is that Dr Lakha says he never said that the front teeth were in danger of falling out, and that given
Sam's age and good health he should bounce back quickly after the extraction of #6 and wisdom teeth.
In the end, Dr Lakha seemed OK with Sam taking his time a bit.
July 18
Dr Becker checked in on Sam through an email, having lost the URL.
His comment regarding an implant was:
However, there is no question in my mind, having seen Sam and his mum [referring to height], that he still has some growth left in him and that a final implant-borne restoration would look short and ugly in a couple of years from now.
Dr Becker checked in on Sam through an email, having lost the URL.
His comment regarding an implant was:
However, there is no question in my mind, having seen Sam and his mum [referring to height], that he still has some growth left in him and that a final implant-borne restoration would look short and ugly in a couple of years from now.
July 28: Dr Kai
Sam says Dr Kai told him he could get the braces off now if he wanted. Dr Kai would make the lower retainer and Dr Beck the upper.
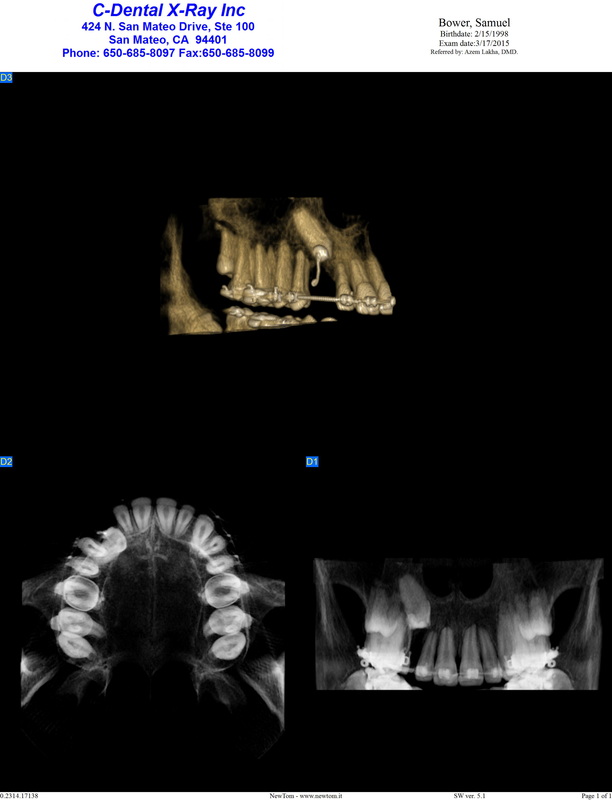
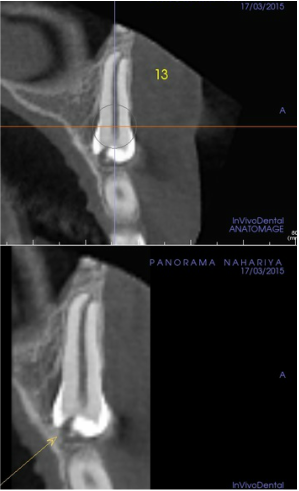
CBCT # 3 and Anatomage
I asked Dr Beck to look at the March CBCT because I haven't been able to look at the DICOMs myself (old computer). Dr Becker was encourage by the good quality (160 MSiv) and sent it on to a radiologist CBCT specialist who analysed it with the help of Anatomage. He made some slides. Dr Becker thinks there are signs of ICRR. At the time of surgery it was hard to fully see the lingual side of #6. The quality of previous imaging is not good enough to totally exclude it. Also there is a break in the glass ionomer filling on the crown.
Dr Becker thinks there is a chance that #6 could move, with a new exposure and treatment of resorptions. If we
could do it in the States is one thing, but where we are now, it's very hard to make another Israel trip without very good odds; on the other hand, the implant is going to take a bunch of steps and operations with grafting and fake flip teeth and waiting for Sam's growth to be done with.
Sam says Dr Kai told him he could get the braces off now if he wanted. Dr Kai would make the lower retainer and Dr Beck the upper.
CBCT # 3 and Anatomage
I asked Dr Beck to look at the March CBCT because I haven't been able to look at the DICOMs myself (old computer). Dr Becker was encourage by the good quality (160 MSiv) and sent it on to a radiologist CBCT specialist who analysed it with the help of Anatomage. He made some slides. Dr Becker thinks there are signs of ICRR. At the time of surgery it was hard to fully see the lingual side of #6. The quality of previous imaging is not good enough to totally exclude it. Also there is a break in the glass ionomer filling on the crown.
Dr Becker thinks there is a chance that #6 could move, with a new exposure and treatment of resorptions. If we
could do it in the States is one thing, but where we are now, it's very hard to make another Israel trip without very good odds; on the other hand, the implant is going to take a bunch of steps and operations with grafting and fake flip teeth and waiting for Sam's growth to be done with.
There is a new gash in the crown.
|
This is the 2012 CBCT, with 25 µSiv, for quality comparison
|

Can't see the piece that the apicotomy should have broken off. Dr Becker says it couldn't have resorbed in 6 months, he thought it was 'ground off', but the surgical notes say : 'A curved root was then identified and curving to the medial and internal aspect, it was gently fractured off with the oseotome and left in place'.
August 27: Dr Beck
Dr Beck wants to close the space for the implant from 11 to 9 mm to match the left side.
September 4: Dr Kai
Dr Kai pulls to make the space 9 mm.
Dr Beck wants to close the space for the implant from 11 to 9 mm to match the left side.
September 4: Dr Kai
Dr Kai pulls to make the space 9 mm.

photo of omputer image of Sam's teeth.
|

|
October 1: Dr Beck
Still 11 mm space
Still 11 mm space
October 4: Dr Kai
Turns out that Dr Kai left the spacer in as it was, so the space couldn't lessen, instead the archwire just bent on the sides. We wasted a month. Also Dr Kai thinks it was 3 months ago we had to give up on the apicotomy, instead of a year ago! Dr Kai took off 2 mm on the spacer.
Turns out that Dr Kai left the spacer in as it was, so the space couldn't lessen, instead the archwire just bent on the sides. We wasted a month. Also Dr Kai thinks it was 3 months ago we had to give up on the apicotomy, instead of a year ago! Dr Kai took off 2 mm on the spacer.
October 16: Dr Kai
Now the space is 9mm
Now the space is 9mm

|

|

|
October 22th: Dr Beck
$ 280
Dr Beck took a mold where he is going to fit a fake tooth and show to Dr Kai in order to get the space right.
Dr Beck also wanted to correct something with the lower molar position on the left side.
$ 280
Dr Beck took a mold where he is going to fit a fake tooth and show to Dr Kai in order to get the space right.
Dr Beck also wanted to correct something with the lower molar position on the left side.
November 2nd: Dr Kai
Teeth tied in again. Three weeks to next appointment.
Sam says it hurts to eat because of the molars being rotated.
Teeth tied in again. Three weeks to next appointment.
Sam says it hurts to eat because of the molars being rotated.
November 24th: Dr Kai
December 16th: Dr Beck
December 18th: Dr Kai
Sam's plastic chain is broken, so we had to see Dr Kai. The chain is trying to pull the molar outward.
Dr Kai said he wanted to grind down the sides of the four lower front teeth since they are a bit crowded, but the bite is good. Sam instinctively said no since this was a totally new technique to him, and me.
I later found that this is called IPR = interproximal reduction.
Sam's plastic chain is broken, so we had to see Dr Kai. The chain is trying to pull the molar outward.
Dr Kai said he wanted to grind down the sides of the four lower front teeth since they are a bit crowded, but the bite is good. Sam instinctively said no since this was a totally new technique to him, and me.
I later found that this is called IPR = interproximal reduction.

January 19th 2016: Dr Beck
Anterior resin composite: $ 600
One of the mended chips from 9 years ago on one of Sam's front teeth was lost to a pizza, so Dr Beck fixed that.
Sounds like it's at the point where the braces can come off.
So that is 5 years of braces!
Anterior resin composite: $ 600
One of the mended chips from 9 years ago on one of Sam's front teeth was lost to a pizza, so Dr Beck fixed that.
Sounds like it's at the point where the braces can come off.
So that is 5 years of braces!
January 19th 2016: Dr Kai
Almost a year and a half after the failed apicotomy, and it looks like the adjustment for an implant are done finally.
Almost a year and a half after the failed apicotomy, and it looks like the adjustment for an implant are done finally.

|
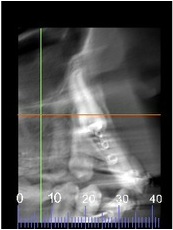
January 19, 2016: lateral cephalogram ($ 75)
To assess end of growth you take a series of these lateral cephs and compare. |
February 8th: Dr Kai
Last adjustment...
Last adjustment...
BRACES OFF AFTER 5 YEARS!
Feb 24 Dr Kai: Removes braces in the morning. Sam turned 18 last week, so his first act as 'adult' was that he was able to sign the paper authorizing the removal of braces.
Feb 24 Dr Beck:
Retainer replacement $ 300
Interim denture - upper $ 1,645.00
Impression for upper stayplate: $ 845
Takes mold. Provides Sam with upper retainer that has a 'tooth' in the canine space. It's temporary, while a lab makes the 'more authentic tooth' contraption. This retainer will then be for night wear.
(It's hard to taste when the palate is covered.)
Feb 26 Dr Kai: Sam received the lower retainer that he is supposed to wear 24/7 for 6 months, after that just night time. (We were warned that a replacement will be $ 200).
Instead of metal, Sam now has a mouth full of plastic. Very frustrating to a teen. Sam doesn't want to eat lunch in school now. School bathrooms are no fun apparently and too much of a hassle. We have detected one visible cavity (Sam's first), I'm not sure if there are white spots, waiting for an evaluation of what the status is.
Feb 24 Dr Beck:
Retainer replacement $ 300
Interim denture - upper $ 1,645.00
Impression for upper stayplate: $ 845
Takes mold. Provides Sam with upper retainer that has a 'tooth' in the canine space. It's temporary, while a lab makes the 'more authentic tooth' contraption. This retainer will then be for night wear.
(It's hard to taste when the palate is covered.)
Feb 26 Dr Kai: Sam received the lower retainer that he is supposed to wear 24/7 for 6 months, after that just night time. (We were warned that a replacement will be $ 200).
Instead of metal, Sam now has a mouth full of plastic. Very frustrating to a teen. Sam doesn't want to eat lunch in school now. School bathrooms are no fun apparently and too much of a hassle. We have detected one visible cavity (Sam's first), I'm not sure if there are white spots, waiting for an evaluation of what the status is.

|

|

You can see the end of the chain to the canine.
|

With the retainer filling the gap
|

|
|
March 16, Dr Beck:
( $ 1645) Sam got his daytime retainer. It has wrought gold clips that go around the molars On the question of what and when to do about the upper front teeth where Sam right now has resin, Dr Beck said he wanted to wait for now. It's good to know where the gum ends up. Sam apparently has a thin and transparent gum covering the top of his front teeth. The alternatives eventually are porcelaine veneer, however Dr Beck warned that when performing this, wrapping the veneer around the tooth, it could shatter the tooth; then you would have to move on with a porcelaine crown, where you have to remove a layer of the tooth, then have it go the length of the tooth, and if the gum recedes the top of the crown would show as a dark line....if all of that fails...then there's more implants.... |

|
April 11, Dr Giannotti:
Paying the price of 5 years of braces, Sam has his first ever cavities, four of them.
Paying the price of 5 years of braces, Sam has his first ever cavities, four of them.
May 6th, Dr Kai:
Sam now experienced enough a driver, and can do the hour-long-drive to Dr Kai who wanted to check the retainers. Not much to it now, except wait for implant when the face is fully grown.
Sam now experienced enough a driver, and can do the hour-long-drive to Dr Kai who wanted to check the retainers. Not much to it now, except wait for implant when the face is fully grown.
May 31st, Dr Beck:
The second front tooth chip broke off after Sam bit into a stew that happened to have a little bone in it.
Dr BEck fixed it right after the Memorial weekend.
The second front tooth chip broke off after Sam bit into a stew that happened to have a little bone in it.
Dr BEck fixed it right after the Memorial weekend.
June 6th, Dr Kai
Dr Kai had Sam come for his assistant to take photos and to give him a referral for imaging: lateral ceph and a pano to 'check root stability'. Next appointment in 6 months.
Dr Kai had Sam come for his assistant to take photos and to give him a referral for imaging: lateral ceph and a pano to 'check root stability'. Next appointment in 6 months.
July 14th, CDental Imaging
$ 205
$ 205

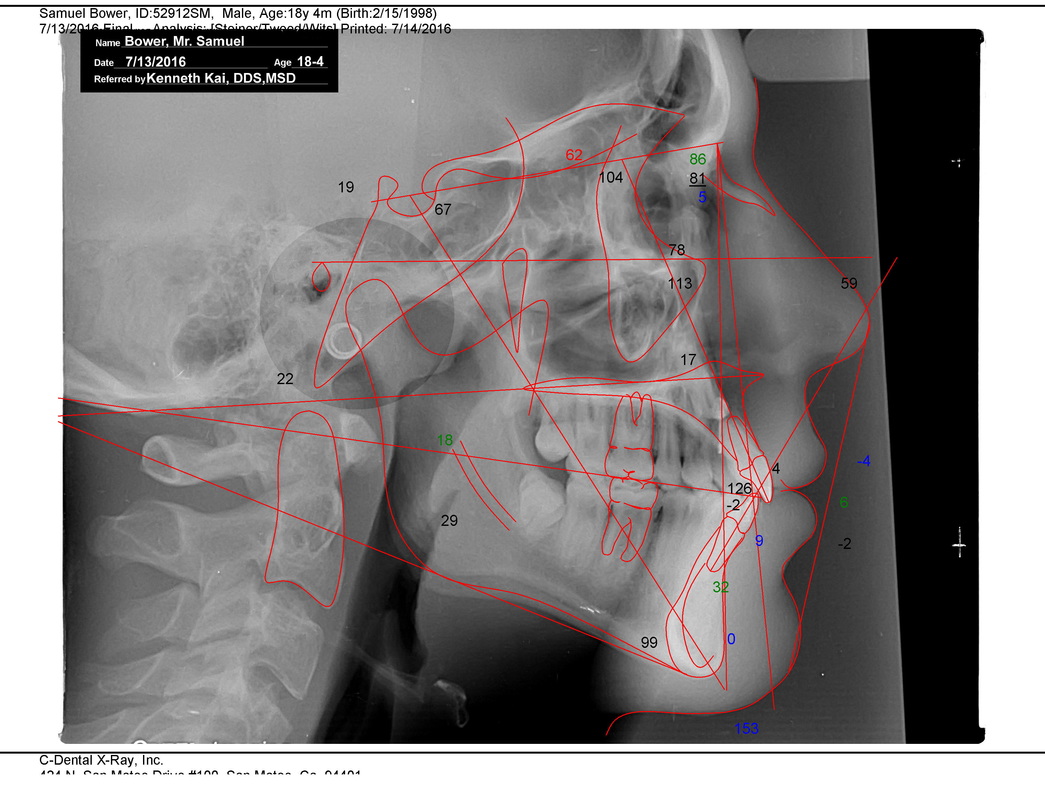
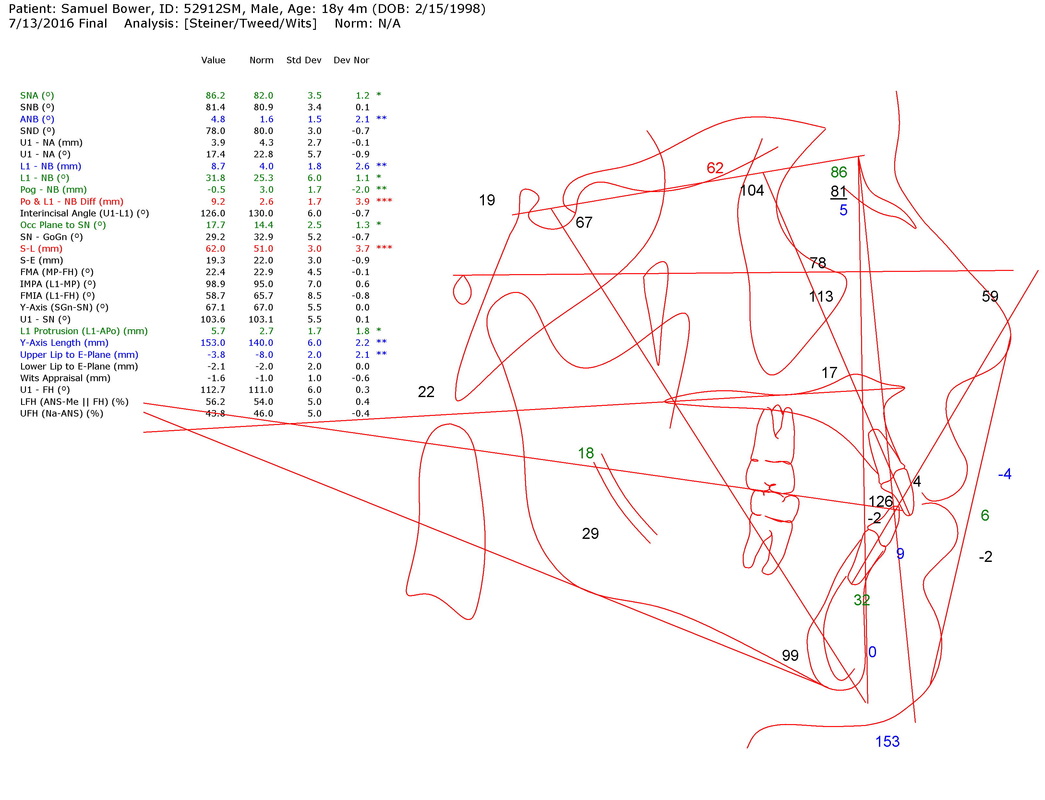
The structures on the lateral cephalogram are all within normal limits with a very pleasing facial profile. The upper right cuspid remains vertically impacted at the floor of the nasal cavity. The third molars are upright with their roots half formed and still lacking room but if Sam continues to grow a bit more they may erupt fully. Whenever your dentist takes Xrays to monitor them, have him/her share the radiographs with me. The inferior border of the mandible (lower jaw bone) are not superimposing, which is not uncommon, and may be due to the short right mandibular ramus. (Dr Kai)

On the panoramic radiograph, all the permanent dentition are present with their roots parallel. The impacted upper right cusid remains high near the apecies of the other permanent teeth. There is a bony defect where the lower right cuspid was impacted but it may slowly fill in. You may want to have a periodontist exam that site to get another opinion. All the third molar crowns are still at the level of the alveolar bone crest. There is blunting of the upper incisors with more on the upper left lateral incisor. The right TMJ condyle and fossa (the ball and socket joint) are abnormally shaped (was present on the initial panoramic radiograph taken July 2014) with the right condylar neck shorter than the respective left structures. I recommend we order a CT scan of the TMJ from C-Dental X-ray lab and get a second opinion from a diagnostic center which C-Dental could arrange. (Dr Kai)
Very upsetting to hear that Sam after his 5 years of braces, and now waiting for grafting, canine extraction and implant, should have a problem with his TMJ!
I am left to googling and I can find nothing that would explain an abnormal condyle other than Progressive Condylar Resorption, unless it was deformed through the trauma Sam had when his upper front teeth hit the counter when he was 8.
Sam has been x-rayed extensively through the years.
So when did the condyle & ramus change? Is it a stable or active process? PCR sounds bad, is described as 'aggressive', 'serious'. How can you stop it/ treat it?
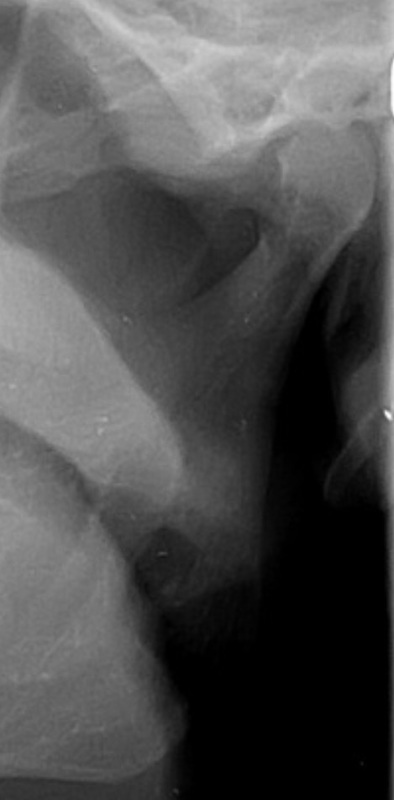
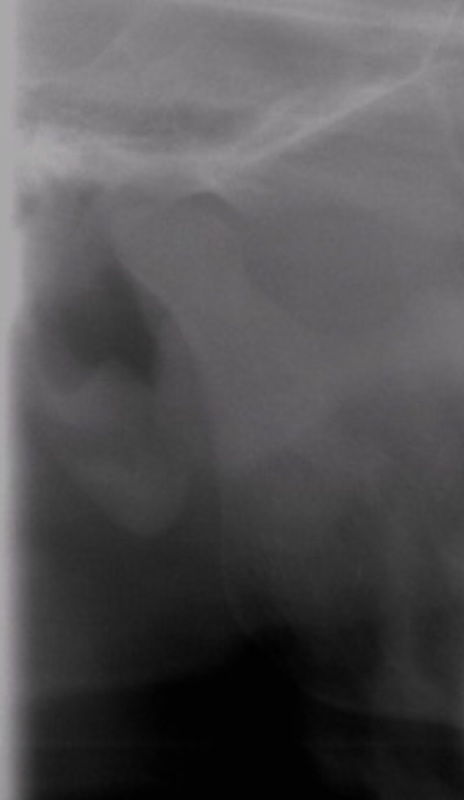
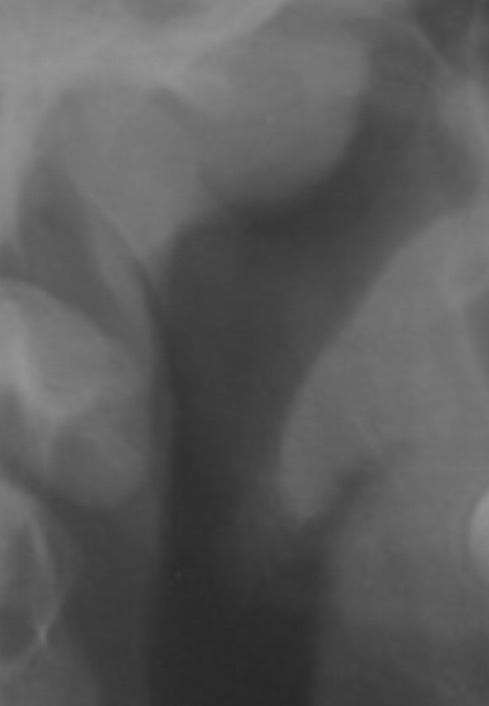
Below is Sam's LEFT condyle 2008-2016. Dr Kai says the RIGHT one is the defect one, but to my eye,
the left is the one that looks like the outline is broken up, but the right condyle is shorter/stubbier. I am hoping someone can give me some answers soon.
I am left to googling and I can find nothing that would explain an abnormal condyle other than Progressive Condylar Resorption, unless it was deformed through the trauma Sam had when his upper front teeth hit the counter when he was 8.
Sam has been x-rayed extensively through the years.
So when did the condyle & ramus change? Is it a stable or active process? PCR sounds bad, is described as 'aggressive', 'serious'. How can you stop it/ treat it?
Below is Sam's LEFT condyle 2008-2016. Dr Kai says the RIGHT one is the defect one, but to my eye,
the left is the one that looks like the outline is broken up, but the right condyle is shorter/stubbier. I am hoping someone can give me some answers soon.

|

|

|

|

|
|
The RIGHT condyle:

|

|
|

|

|
|

|
CDental, San Mateo: TMJ CBCT
9/13/2016, $515
15 x 15 standard 112 µSv + 15 x 15 ecco (open mouth) 72 µSv
So Sam has done the CBCT of the temperomandibular joint, and there is the radiological report in pdf below. I've had no professional interpretation, but the radiological report doesn't speak of anything 'progressive' which is comforting, but of "regressive osseous remodelling for the TMJs, most likely functional in origin". There is no comparison, or talk of the right mandibular condyle, fossa, ramus, looking different from the left as described by Dr Kai.
I am now waiting to hear Dr Beck and Dr McNeil (TMJ expert at UCSF) have to say.
9/13/2016, $515
15 x 15 standard 112 µSv + 15 x 15 ecco (open mouth) 72 µSv
So Sam has done the CBCT of the temperomandibular joint, and there is the radiological report in pdf below. I've had no professional interpretation, but the radiological report doesn't speak of anything 'progressive' which is comforting, but of "regressive osseous remodelling for the TMJs, most likely functional in origin". There is no comparison, or talk of the right mandibular condyle, fossa, ramus, looking different from the left as described by Dr Kai.
I am now waiting to hear Dr Beck and Dr McNeil (TMJ expert at UCSF) have to say.












| 2016-09-13_bower_samuel_-_beamreaders_report.pdf |
Since there was no mention of anything different with the right side as described by Dr Kai, I wrote Dr Francisco Eraso twice for clarification. When I did not get any reply I turned to David Hatcher of Beamreader's who wrote on Oct 24:
I had a look at the report from Dr. Eraso and the images in the report show the right TMJ and mandible fairly well. Everything is relatively normal radiographically. The right condyle is slightly smaller than the left ( perhaps regressive remodeling) but I don’t suspect any progressive issues. The mandible appears to be growing symmetrically.
FYI, A panoramic projection is a screening image and may alter the size and shape perception of the anatomy. The CBCT scan that Sam had is much more accurate.
Then Dr Beck forwarded a response from Dr McNeil on Nov 4:
The right and left condyles are within normal biologic limits as to their size and shape. There are very subtle biological variation in condylar shape that is the normal case as opposed to perfect symmetry. There are normal superior and posterior joint spaces with slightly posteriorly positioned condyles that again falls into normal biological variation in condylar position. The cortical surface bone is intact without any evidence of subchondral bone cysts. The range of condylar translation on opening is normal and just beyond the height of the eminentia. Lastly, there appears to be normal and relatively symmetrical growth of the maxillae and mandible.”
So, in the end, much todo about nothing.
I had a look at the report from Dr. Eraso and the images in the report show the right TMJ and mandible fairly well. Everything is relatively normal radiographically. The right condyle is slightly smaller than the left ( perhaps regressive remodeling) but I don’t suspect any progressive issues. The mandible appears to be growing symmetrically.
FYI, A panoramic projection is a screening image and may alter the size and shape perception of the anatomy. The CBCT scan that Sam had is much more accurate.
Then Dr Beck forwarded a response from Dr McNeil on Nov 4:
The right and left condyles are within normal biologic limits as to their size and shape. There are very subtle biological variation in condylar shape that is the normal case as opposed to perfect symmetry. There are normal superior and posterior joint spaces with slightly posteriorly positioned condyles that again falls into normal biological variation in condylar position. The cortical surface bone is intact without any evidence of subchondral bone cysts. The range of condylar translation on opening is normal and just beyond the height of the eminentia. Lastly, there appears to be normal and relatively symmetrical growth of the maxillae and mandible.”
So, in the end, much todo about nothing.
Dec 15, 2016: Dr Kai
Dec 22, 2016: Dr Beck: new retainer, old one getting worn.
Dec 22, 2016: Dr Beck: new retainer, old one getting worn.
Dr Adrian Becker made Sam's case the subject of his January 2017 Bulletin:
"Is PEIR a casual factor for non-eruption?"
"Is PEIR a casual factor for non-eruption?"
| prof._adrian_becker__newsletters_archive.html |

Sam has done 3 lateral cephs to check for growth. I asked Dr Beck to review them and heard back that he is retiring.
Nov 20, 2017: Sam calls and says a piece of pizza took off one of his front teeths’ mended chips. They were last fixed in January and May of last year. We hope Dr Giannotti can fix it asap after Thanksgiving. Another composite bonding, or veneer?