Advanced biomechanics and impacted canines
Forces at work
Here's a recent, well-informed presentation of orthodontic biomechanics:http://www.slideshare.net/almuzian/biomechanics-in-orthodontics-by-almuzian-31692045
(2):
Concerning magnitude of force:
More recently Ren et al (2003) systematically reviewed the literature concerning the optimal force or range
of forces for orthodontic tooth movement. They found that there was neiter universal consensus nor sound
scientific evidence regarding specific numeric values of optimal force magnitude.
Concerning the direction of force:
The direction of the applied force is important as it will affect the amount of force being applied to a
particular area of the root and periodontal ligament. There are five basic types of tooth movement:
1. Tipping: The forces used to tip teeth must be kept low (35-60 mg) as the pressure in the two areas where
it is concentrated is high in relation to the force applied to the crown.
2. Bodily movement: 100-150 g force to achieve an optimal PDL stress (a moment to force ratio of at least
8:1 is also required at the bracket wire interface to overcome the tipping effect)
3. Torque: It describes the differential movement of one part of a tooth, usually the root, whilst physically
restraining any movement of the crown. It is achieved by applying a force couple to the crown of the
tooth, only in this instance the moment to force ratio must be greater that 8:1.
4. Rotation: The objective being to rotate the tooth around its long axis. However, rotational vbectors
invariably result in some tipping and forces should therefore be limited to 35-60g
5. Intrusion and Extrusion: extrusive forces applied to buccal attachments will result in tipping and stress
concentration in areas of the periodontal ligament. Therefore forces need to be light, 35-60g. Intrusive
forces concentrate stress at the root apex. As this is of very small surface area the forces used need to be
very light, 10-20g.
Here's a recent, well-informed presentation of orthodontic biomechanics:http://www.slideshare.net/almuzian/biomechanics-in-orthodontics-by-almuzian-31692045
(2):
Concerning magnitude of force:
More recently Ren et al (2003) systematically reviewed the literature concerning the optimal force or range
of forces for orthodontic tooth movement. They found that there was neiter universal consensus nor sound
scientific evidence regarding specific numeric values of optimal force magnitude.
Concerning the direction of force:
The direction of the applied force is important as it will affect the amount of force being applied to a
particular area of the root and periodontal ligament. There are five basic types of tooth movement:
1. Tipping: The forces used to tip teeth must be kept low (35-60 mg) as the pressure in the two areas where
it is concentrated is high in relation to the force applied to the crown.
2. Bodily movement: 100-150 g force to achieve an optimal PDL stress (a moment to force ratio of at least
8:1 is also required at the bracket wire interface to overcome the tipping effect)
3. Torque: It describes the differential movement of one part of a tooth, usually the root, whilst physically
restraining any movement of the crown. It is achieved by applying a force couple to the crown of the
tooth, only in this instance the moment to force ratio must be greater that 8:1.
4. Rotation: The objective being to rotate the tooth around its long axis. However, rotational vbectors
invariably result in some tipping and forces should therefore be limited to 35-60g
5. Intrusion and Extrusion: extrusive forces applied to buccal attachments will result in tipping and stress
concentration in areas of the periodontal ligament. Therefore forces need to be light, 35-60g. Intrusive
forces concentrate stress at the root apex. As this is of very small surface area the forces used need to be
very light, 10-20g.
The long and the short regarding techniques for tackling an impacted canine, seems to be that it will cover the
whole range from 'I-pulled-I tried-didn't work-we have to extract-you can have an implant in 5 years instead' to people putting an immense amount of thought into the problem, writing books and papers. Even though there are conferences and easy access to articles from around the globe, the world of orthodontics can appear like isolated islands, where some places are really into saving canines, and others feel that it is not worth effort.
The difference between the casual treatment an impacted canine gets as far as we have experienced it in 'Sam's case' gets painfully poignant reading the thoughtful, careful descriptions of how it is done by professionals who bother about diagnosis, thinking about the biomechanics, traction, etc.
I found this article: Enamel drilling for canine traction: advantaged, disadvantages, description of surgical technique and biomechanics, by Brazilian authors from 2011. (1) The article holds that in order to create the space for the canine
orthopedic maxillary expansion seems unquestionable with this protocol - a sine qua non condition for a real
increase in bone mass by adding bone to the midpalatal suture - creating space and enabling a better
eruption pathway, often avoiding surgical approaches and orthodontic traction
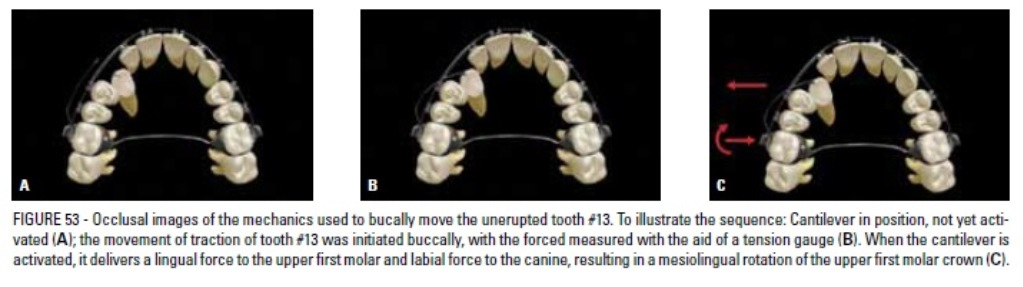
Below, an image from the article, where they use a 'palatal bar' for increased anchorage
whole range from 'I-pulled-I tried-didn't work-we have to extract-you can have an implant in 5 years instead' to people putting an immense amount of thought into the problem, writing books and papers. Even though there are conferences and easy access to articles from around the globe, the world of orthodontics can appear like isolated islands, where some places are really into saving canines, and others feel that it is not worth effort.
The difference between the casual treatment an impacted canine gets as far as we have experienced it in 'Sam's case' gets painfully poignant reading the thoughtful, careful descriptions of how it is done by professionals who bother about diagnosis, thinking about the biomechanics, traction, etc.
I found this article: Enamel drilling for canine traction: advantaged, disadvantages, description of surgical technique and biomechanics, by Brazilian authors from 2011. (1) The article holds that in order to create the space for the canine
orthopedic maxillary expansion seems unquestionable with this protocol - a sine qua non condition for a real
increase in bone mass by adding bone to the midpalatal suture - creating space and enabling a better
eruption pathway, often avoiding surgical approaches and orthodontic traction
Below, an image from the article, where they use a 'palatal bar' for increased anchorage
(1) Filho L, Consolaro A, Almeida Cardoso, Siqueira D. Enamel drilling for canine traction: advantages,
disadvantages, description of surgical technique and biomechanics.Dental Press Journalk of Orthodontics. vol
16 no 5 Maringá Sept./Oct. 2011.
(2) Dr. Mohammed Almuzian, University of Glasgow. Biomechanics in orthodontics. 1/1 2013.
(3) Nilesh V. Joshi. POeriodontal Status Following Treatment of Impacted Maxillary Canines by Closed Eruption
Technique: An Overview and Case REport. J Orthod 2014 Mar;41(1): 13-8.
disadvantages, description of surgical technique and biomechanics.Dental Press Journalk of Orthodontics. vol
16 no 5 Maringá Sept./Oct. 2011.
(2) Dr. Mohammed Almuzian, University of Glasgow. Biomechanics in orthodontics. 1/1 2013.
(3) Nilesh V. Joshi. POeriodontal Status Following Treatment of Impacted Maxillary Canines by Closed Eruption
Technique: An Overview and Case REport. J Orthod 2014 Mar;41(1): 13-8.