Reality check: Who treats impacted canines?
Unfortunately, anyone. Of the 4 orthodontists we saw prior to starting treatment, no one shunned the prospect of dealing with impaction. They did imply that they could fail, it was not quite clear what would happen in that case. Nobody mentioned CBCT.
Unfortunately, anyone. Of the 4 orthodontists we saw prior to starting treatment, no one shunned the prospect of dealing with impaction. They did imply that they could fail, it was not quite clear what would happen in that case. Nobody mentioned CBCT.
Hope for the best, prepare for the worst
When it works, it works. But, what is the plan if the teeth do not erupt? If you think of possible failure from the outset, you probably prepare treatment better from the outset. Another saying that works for impacted canines is 'fools rush in, where angels fear to tread'.
This is an abstract by the head orthodontics and clinic for impacted canines at the Jerusalem
University Hospital, Dr. Stella Chaushu:
Maxillary canine impaction occurs in 1-3% of most Western populations and its orthodontic
treatment is difficult. Failure to resolve the impaction is not uncommon and may lead to
malpractice lawsuits. The information in the literature about the reasons for non-resolution of the
condition is sparse and unsubstantiated. This encourages the dispensing of inappropriate
treatment that may result in severe tooth, soft and hard tissue damage as well as a prolonged
treatment period. This review describes the epidemiology, pathogensis and the wide range of
reasons that may lead to failure to resolve the canine impaction. It shows a lack of appreciation
of anchorage demands and inaccurate positional diagnosis of the 3-D location and orientation of
impacted teeth are the major reasons for failure. In addition the review that invasive cervical
root resorption (ICRR) is a frequently undiagnosed or unrecognized cause of failure of
orthodontic resolution of impacted canines, and should be distinguished from replacement
resorption (ankylosis). Corrective measures which may lead to successful treatment are further
recommended. Special emphasis is placed on the pathology of impacted teeth and damage to
anchor teeth. The importance of teamwork in achieving the best treatment outcome is
stressed.(33)
When it works, it works. But, what is the plan if the teeth do not erupt? If you think of possible failure from the outset, you probably prepare treatment better from the outset. Another saying that works for impacted canines is 'fools rush in, where angels fear to tread'.
This is an abstract by the head orthodontics and clinic for impacted canines at the Jerusalem
University Hospital, Dr. Stella Chaushu:
Maxillary canine impaction occurs in 1-3% of most Western populations and its orthodontic
treatment is difficult. Failure to resolve the impaction is not uncommon and may lead to
malpractice lawsuits. The information in the literature about the reasons for non-resolution of the
condition is sparse and unsubstantiated. This encourages the dispensing of inappropriate
treatment that may result in severe tooth, soft and hard tissue damage as well as a prolonged
treatment period. This review describes the epidemiology, pathogensis and the wide range of
reasons that may lead to failure to resolve the canine impaction. It shows a lack of appreciation
of anchorage demands and inaccurate positional diagnosis of the 3-D location and orientation of
impacted teeth are the major reasons for failure. In addition the review that invasive cervical
root resorption (ICRR) is a frequently undiagnosed or unrecognized cause of failure of
orthodontic resolution of impacted canines, and should be distinguished from replacement
resorption (ankylosis). Corrective measures which may lead to successful treatment are further
recommended. Special emphasis is placed on the pathology of impacted teeth and damage to
anchor teeth. The importance of teamwork in achieving the best treatment outcome is
stressed.(33)
Bad scenarios
Dealing with an impacted is not just about saving that individual tooth or not, there is also
consequences for the neighboring teeth and the alveolar ridge, the bone that teeth are sitting in and
that prevents them from falling out.
Below is an article siting some problems with palatally impacted canines and the problems, and the risk for orthodontists getting sued:
First, the overall length of orthodontic treatment is increased when the patient has a palatal
impaction. Second there are often problems of alveolar bone loss around the adjacent lateral
incisor and premolars as well as the canine. Third, root resorption of the adjacent lateral incisor
is a common aftermath of treating a palatally impacted canine. Finally gingival recession on the
labial or palatal surfaces can accompany treatment of these teeth.(35)
The article above recommends early preorthodontic uncovering of palatally impacted canines, so for a 10 or 11 year-old. It is also recommended for treatment of adults. Interestingly, the article points out, in regards to adults:
A palatally displaced maxillary canine in a 35-year-old has been encased in bone for over 20 years. It is
highly likely that the tissue surrounding the root of that tooth will not be as responsive to autonomous
eruption immediately after uncovering as is typically seen in adolescents. This does not mean that the tooth
will not erupt. We believe that the surgical uncovering process signals the tissue surrounding the root to
gradually be transformed into a functioning periodontal ligament that will permit autonomous eruption with time. In fact, we have not encountered a tooth that would not erupt autonomously after uncovering,
even in adults.(35)
Dealing with an impacted is not just about saving that individual tooth or not, there is also
consequences for the neighboring teeth and the alveolar ridge, the bone that teeth are sitting in and
that prevents them from falling out.
Below is an article siting some problems with palatally impacted canines and the problems, and the risk for orthodontists getting sued:
First, the overall length of orthodontic treatment is increased when the patient has a palatal
impaction. Second there are often problems of alveolar bone loss around the adjacent lateral
incisor and premolars as well as the canine. Third, root resorption of the adjacent lateral incisor
is a common aftermath of treating a palatally impacted canine. Finally gingival recession on the
labial or palatal surfaces can accompany treatment of these teeth.(35)
The article above recommends early preorthodontic uncovering of palatally impacted canines, so for a 10 or 11 year-old. It is also recommended for treatment of adults. Interestingly, the article points out, in regards to adults:
A palatally displaced maxillary canine in a 35-year-old has been encased in bone for over 20 years. It is
highly likely that the tissue surrounding the root of that tooth will not be as responsive to autonomous
eruption immediately after uncovering as is typically seen in adolescents. This does not mean that the tooth
will not erupt. We believe that the surgical uncovering process signals the tissue surrounding the root to
gradually be transformed into a functioning periodontal ligament that will permit autonomous eruption with time. In fact, we have not encountered a tooth that would not erupt autonomously after uncovering,
even in adults.(35)
Required reading!? a novel idea?
My main discovery in the process of my research, as a parent, into impacted canines, is the the ignorance of dental professionals on the subject. It is both heart breaking and infuriating. How can anyone be allowed to treat impacted canines without reading a book on the subject, taking a course, taking a test, proving themselves qualified? If you venture through 'the very long version of Sam's case' you will see that Sam has passed through the hands of dentists, orthodontists, oral surgeons, several professors at the University of San Francisco...and I, the mom, has to diagnose the resorption that is complicating my son's impacted canines! When the professors of endodontics and oral surgery are confronted with the term of PEIR (pre-eruptive intra-coronal resorption) they
are flustered and in denial.
My main discovery in the process of my research, as a parent, into impacted canines, is the the ignorance of dental professionals on the subject. It is both heart breaking and infuriating. How can anyone be allowed to treat impacted canines without reading a book on the subject, taking a course, taking a test, proving themselves qualified? If you venture through 'the very long version of Sam's case' you will see that Sam has passed through the hands of dentists, orthodontists, oral surgeons, several professors at the University of San Francisco...and I, the mom, has to diagnose the resorption that is complicating my son's impacted canines! When the professors of endodontics and oral surgery are confronted with the term of PEIR (pre-eruptive intra-coronal resorption) they
are flustered and in denial.
|
There are books on the subject of impacted canines, with chapters on 'Invasive Cervical Root resorption' and everything that can complicate a successful outcome, including PEIR.
With any kind of curiosity, anyone can find recent case studies and research around the world on all the potential problems you come up against, when dealing with impacted canines. How can the standard be set so low that ignorance of the kind of knowledge that can be looked up in a textbook is acceptable at a University Clinic! If you don't care to know, you can't diagnose, and you can't treat your patients. |
|
In the preface to the first edition of my book which was published in 1998, I pointed out at the time that there were virtually no graduate/postgraduate orthodontic specialty programs that included tooth impaction in their curricula in any didactic or disciplined academic fashion. This situation has not changed in the 15 years since that time. The upshot is that there are few orthodontists out there in the big wide world who are proficient at treating them
Dr. Becker's January 2013 Bulletin
There is run-of-the-mill orthodontics and then there is Impacted Canines
Parents have to be aware that an orthodontist is not necessarily a specialist on the subject of impacted canines. It occurs in 1-3 %, so it will take some time to gain experience for the individual orthodontist, and if you do not have the interest and inclination, the risk is that the impacted canine will be treated as what I call 'a unicorn' (see Sam's very long version). The orthodontist will give it a go, not analyzing the complexities behind the cause of extraction. If pulling here and there is ineffective, they will declare it 'ankylosed!' (think Queen of Hearts and 'off with his head'), and the canine is history.
When impacted teeth get somewhere where there is interest enough to document, write case studies, and make
studies of outcome, the outlook for an impacted canine is relatively bright. An Irish study (30) showed that 96% of impacted canines with surgical intervention succeeded, another 2% succeeded with reoperation, and finally only 2% were lost. A Canadian study (38) had 54 patients with 82 maxillary canines, and all were successfully brought in occlusion, though 6 had to be rebonded in the course of treatment.
This is the real heart break: lots of teeth can be saved, saving patients lots of pain, suffering,
years in braces, high expense, implants... Failure to managed an impacted canine has to be analyzed and explained, it should be extremely unusual.
The problem of impacted canines, and definitely the 'non responders', is that they have not been treated with enough attention by the dental schools and orthodontists in general . This is how Dr. Adrian Becker concludes his article from 2010 on the 'Analysis of failure in the treatment of impacted canines':
From this platform, we issue a cri de coeur to encourage the teaching of this subject as a separate entity in
graduate orthodontic programs in which it is conspicuously absent at this time.(p 753) (1)
This is Dr. Becker in his January 2013 Bulletin:
In the preface to the first edition of my book which was published in 1998, I pointed out at the time that
there were virtually no graduate/postgraduate orthodontic specialty programs that included tooth impaction
in their curricula in any didactic or disciplined academic fashion. This situation has not changed in the 15
years since that time.
Bring Dr. Becker's article along as support when you interview orthodontists wanting your business! Dr. Becker is speaking as a Professor Emeritus of Orthodontics in Jerusalem, and he is an international speaker and textbook author on the specific subject of impacted teeth. I think his statement can stand as an international plea in the field of orthodontia.
Often with impaction there is oral surgery involved. There are different approaches and techniques. Oral surgeons mainly deal with extraction of wisdom teeth, so same as with orthodontists, an impacted canine is the odd duck.
Actually, I have the sense that orthodontists want to avoid oral surgeons if possible and go with the more delicate touches of periodontists if they can. 'Efficient Management of Unerupted Teeth: A Time-Tested Treatment Modality' describes:
increasingly frequent complications observed with unerupted teeth, especially canines. This phenomenon
of more frequent harmful sequelae may be attributed to the surgical technique used to uncover the
teeth. (p 212)(2)
The combined efforts of the orthodontist, oral surgeon and endodontist must be thought through carefully for a good result in the more than simplest cases. This is the essential springing point.
I could only wish that all orthodontists approached impacted teeth the way Dr. Becker does. This IS rocket science! It evidently is too hard for the average orthodontist, but is that an excuse for sacrificing 'impacted canines' when there are ways to deal with them. It is puzzling and very sad to realize that something that afflicts our children and teens, and will affect them their whole lives, is not taken seriously, even at Universities!
Parents have to be aware that an orthodontist is not necessarily a specialist on the subject of impacted canines. It occurs in 1-3 %, so it will take some time to gain experience for the individual orthodontist, and if you do not have the interest and inclination, the risk is that the impacted canine will be treated as what I call 'a unicorn' (see Sam's very long version). The orthodontist will give it a go, not analyzing the complexities behind the cause of extraction. If pulling here and there is ineffective, they will declare it 'ankylosed!' (think Queen of Hearts and 'off with his head'), and the canine is history.
When impacted teeth get somewhere where there is interest enough to document, write case studies, and make
studies of outcome, the outlook for an impacted canine is relatively bright. An Irish study (30) showed that 96% of impacted canines with surgical intervention succeeded, another 2% succeeded with reoperation, and finally only 2% were lost. A Canadian study (38) had 54 patients with 82 maxillary canines, and all were successfully brought in occlusion, though 6 had to be rebonded in the course of treatment.
This is the real heart break: lots of teeth can be saved, saving patients lots of pain, suffering,
years in braces, high expense, implants... Failure to managed an impacted canine has to be analyzed and explained, it should be extremely unusual.
The problem of impacted canines, and definitely the 'non responders', is that they have not been treated with enough attention by the dental schools and orthodontists in general . This is how Dr. Adrian Becker concludes his article from 2010 on the 'Analysis of failure in the treatment of impacted canines':
From this platform, we issue a cri de coeur to encourage the teaching of this subject as a separate entity in
graduate orthodontic programs in which it is conspicuously absent at this time.(p 753) (1)
This is Dr. Becker in his January 2013 Bulletin:
In the preface to the first edition of my book which was published in 1998, I pointed out at the time that
there were virtually no graduate/postgraduate orthodontic specialty programs that included tooth impaction
in their curricula in any didactic or disciplined academic fashion. This situation has not changed in the 15
years since that time.
Bring Dr. Becker's article along as support when you interview orthodontists wanting your business! Dr. Becker is speaking as a Professor Emeritus of Orthodontics in Jerusalem, and he is an international speaker and textbook author on the specific subject of impacted teeth. I think his statement can stand as an international plea in the field of orthodontia.
Often with impaction there is oral surgery involved. There are different approaches and techniques. Oral surgeons mainly deal with extraction of wisdom teeth, so same as with orthodontists, an impacted canine is the odd duck.
Actually, I have the sense that orthodontists want to avoid oral surgeons if possible and go with the more delicate touches of periodontists if they can. 'Efficient Management of Unerupted Teeth: A Time-Tested Treatment Modality' describes:
increasingly frequent complications observed with unerupted teeth, especially canines. This phenomenon
of more frequent harmful sequelae may be attributed to the surgical technique used to uncover the
teeth. (p 212)(2)
The combined efforts of the orthodontist, oral surgeon and endodontist must be thought through carefully for a good result in the more than simplest cases. This is the essential springing point.
I could only wish that all orthodontists approached impacted teeth the way Dr. Becker does. This IS rocket science! It evidently is too hard for the average orthodontist, but is that an excuse for sacrificing 'impacted canines' when there are ways to deal with them. It is puzzling and very sad to realize that something that afflicts our children and teens, and will affect them their whole lives, is not taken seriously, even at Universities!
Parents: Educate yourself! as early in the process as possible
The ultimate lesson, as with most things, is, if something is really important to you, make yourself an expert. You can delve into the finer aspects of orthodontia, but I think just a simple basic knowledge of the problems, the resources, and what kind of outcomes you could reasonably expect, can help you along. You might think that you are paying for a specialist to take care of things, but by being informed and asking questions you can better assure yourself that the specialist indeed is a specialist; and you can at least have a clue trying to judge if you are dealing with someone you want to let loose on you child's teeth, spending years and thousands of dollars. Don't wait for things to get to the point where you are handed a referral for extraction. If you start getting a sense that things are not heading in the right direction, get a second opinion.
Here is a paper to get into some basics of impacted teeth and their treatment: 'Surgical Management of the Impacted Canine and Second Molar' (29) by Dr. Pamela Alberto.
The ultimate lesson, as with most things, is, if something is really important to you, make yourself an expert. You can delve into the finer aspects of orthodontia, but I think just a simple basic knowledge of the problems, the resources, and what kind of outcomes you could reasonably expect, can help you along. You might think that you are paying for a specialist to take care of things, but by being informed and asking questions you can better assure yourself that the specialist indeed is a specialist; and you can at least have a clue trying to judge if you are dealing with someone you want to let loose on you child's teeth, spending years and thousands of dollars. Don't wait for things to get to the point where you are handed a referral for extraction. If you start getting a sense that things are not heading in the right direction, get a second opinion.
Here is a paper to get into some basics of impacted teeth and their treatment: 'Surgical Management of the Impacted Canine and Second Molar' (29) by Dr. Pamela Alberto.
When the standard procedure does not work, this is the point where your orthodontist has to show his colors. Does he/she:
a) have the experience and inclination to deal with it himself/herself? Does he/she work have a hand-in-glove-working-relationship with an oral surgeon.
b) refer you for 3D imaging and/or to someone specializing in impacted canines (I am not sure if there are anyone, at least they don't advertise), or
c) give up and end the whole thing by referring you to have the canine extracted
Several articles emphasize that the successful management of a severely impacted maxillary canine require close cooperation of an orthodontist, an oral surgeon, a radiologist, a periodontist, and, if necessary, a prosthodontist. Dr. Adrian Becker writes in his March Bulletin (28) :
The very fact that the tooth has not erupted should raise the suspicions of the orthodontist to find out why.
There is usually an obvious cause. There may be obstruction due to the presence of the root of an adjacent
tooth, or a supernumerary tooth, perhaps an enlarged dental follicle, or conversely, disappearance of the
dental follicle and ankylosis. Most of these factors can be identified ahead of time and should therefore not
come as a surprise, and certainly not after several fruitless years of applying traction – as we sometimes
see.
accurate positional diagnosis is often fraught with difficulty, and mistakes may be made
in locating the tooth - even by experts. As a result, a tooth in an intractable position may be
thought to have a good prognosis, and an inappropriate, ill-advised, and ill-fated course of
treatment will be prescribed.
...
An open surgical exposure of the impacted tooth may close over in the succeeding days and
weeks and make later attachment bonding unreliable or impossible to achieve. When bonding
is performed by the surgeon, as an integral task during an open or closed exposure, an
attachment may be placed in an inappropriate position on the tooth surface or the pigtail ligature
wire or gold chain may have been drawn through the tissues in the wrong direction for traction
to resolve impaction. Alternatively, the bond may fail, and, without further surgery, suitable
conditions for rebonding may be limited or unattainable...(p 261)(18)
These are the possible reasons for failure are, again, in the words of Dr. Becker:
1. Patient-dependent factors (abnormal morphology of the impacted tooth, age, pathology of the impacted
tooth, grossly ectopic tooth, resorption of the root of an adjacent tooth, and lack of compliance
(eg. missed appointments, inadequate oral hygiene).
2. Orthodontist-dependent factors: mistaken positional diagnosis and inappropriate directional force,
missed diagnosis of resorption of the root of an adjacent tooth,, poor anchorage, ineffiecient appliance,
and inadequate torque.
3. Surgeon-dependent factors: mistaken positional diagnosis, exposure of the wrong side, or rummaging
exposure; injury to the an adjacent tooth; soft-tissue damage; and surgery without orthodontic planning.
(p. 743-744). (14)
Different types of impacted canines and complications:
1. There is a distinction between palatally (on the palate side - 85% of impacted canines) and
labially (on the front, 'lip side', 15%) mislocated canines.
2. Another definition of location is 'the height of the impacted canine to the occlusal plane' (p 235)(23); that is
how high up the tooth is compared to where it is supposed to end up.
3. The angle of the tooth.
4. The degree of root formation.
5. An aggravating factor with impacted teeth is the possibility of resorption of the root of adjacent teeth just by
crowding each other.
6. Treating the impacted canines can negatively affect the other teeth. Usually you are trying to change the
whole bite as one piece
A factor that significantly influences the duration of treatment but is frequently ignored relates to
the additional period needed to correct deleterious effects created by canine eruption on the
adjacent teeth, ie, loss of anchorage...The anchor teeth must then be realigned, thus increasing
the treatment time...Long periods of orthodontic treatment may lead to damage to the enamel and
the appearance of white spots, decalcified areas, or even caries if good oral hygiene is not
maintained and to more severe root resorption. (pp 235-6)(23)
So, beware of the false ankylosis that only represents failure by the orthodontist to analyze and treat the problem. Even the 'true' ankylosis is a relative term. Teeth that don't respond to traction can be treated, if you happen to live where there are interested specialists, by transplantation and apictomy, see below.
a) have the experience and inclination to deal with it himself/herself? Does he/she work have a hand-in-glove-working-relationship with an oral surgeon.
b) refer you for 3D imaging and/or to someone specializing in impacted canines (I am not sure if there are anyone, at least they don't advertise), or
c) give up and end the whole thing by referring you to have the canine extracted
Several articles emphasize that the successful management of a severely impacted maxillary canine require close cooperation of an orthodontist, an oral surgeon, a radiologist, a periodontist, and, if necessary, a prosthodontist. Dr. Adrian Becker writes in his March Bulletin (28) :
The very fact that the tooth has not erupted should raise the suspicions of the orthodontist to find out why.
There is usually an obvious cause. There may be obstruction due to the presence of the root of an adjacent
tooth, or a supernumerary tooth, perhaps an enlarged dental follicle, or conversely, disappearance of the
dental follicle and ankylosis. Most of these factors can be identified ahead of time and should therefore not
come as a surprise, and certainly not after several fruitless years of applying traction – as we sometimes
see.
accurate positional diagnosis is often fraught with difficulty, and mistakes may be made
in locating the tooth - even by experts. As a result, a tooth in an intractable position may be
thought to have a good prognosis, and an inappropriate, ill-advised, and ill-fated course of
treatment will be prescribed.
...
An open surgical exposure of the impacted tooth may close over in the succeeding days and
weeks and make later attachment bonding unreliable or impossible to achieve. When bonding
is performed by the surgeon, as an integral task during an open or closed exposure, an
attachment may be placed in an inappropriate position on the tooth surface or the pigtail ligature
wire or gold chain may have been drawn through the tissues in the wrong direction for traction
to resolve impaction. Alternatively, the bond may fail, and, without further surgery, suitable
conditions for rebonding may be limited or unattainable...(p 261)(18)
These are the possible reasons for failure are, again, in the words of Dr. Becker:
1. Patient-dependent factors (abnormal morphology of the impacted tooth, age, pathology of the impacted
tooth, grossly ectopic tooth, resorption of the root of an adjacent tooth, and lack of compliance
(eg. missed appointments, inadequate oral hygiene).
2. Orthodontist-dependent factors: mistaken positional diagnosis and inappropriate directional force,
missed diagnosis of resorption of the root of an adjacent tooth,, poor anchorage, ineffiecient appliance,
and inadequate torque.
3. Surgeon-dependent factors: mistaken positional diagnosis, exposure of the wrong side, or rummaging
exposure; injury to the an adjacent tooth; soft-tissue damage; and surgery without orthodontic planning.
(p. 743-744). (14)
Different types of impacted canines and complications:
1. There is a distinction between palatally (on the palate side - 85% of impacted canines) and
labially (on the front, 'lip side', 15%) mislocated canines.
2. Another definition of location is 'the height of the impacted canine to the occlusal plane' (p 235)(23); that is
how high up the tooth is compared to where it is supposed to end up.
3. The angle of the tooth.
4. The degree of root formation.
5. An aggravating factor with impacted teeth is the possibility of resorption of the root of adjacent teeth just by
crowding each other.
6. Treating the impacted canines can negatively affect the other teeth. Usually you are trying to change the
whole bite as one piece
A factor that significantly influences the duration of treatment but is frequently ignored relates to
the additional period needed to correct deleterious effects created by canine eruption on the
adjacent teeth, ie, loss of anchorage...The anchor teeth must then be realigned, thus increasing
the treatment time...Long periods of orthodontic treatment may lead to damage to the enamel and
the appearance of white spots, decalcified areas, or even caries if good oral hygiene is not
maintained and to more severe root resorption. (pp 235-6)(23)
So, beware of the false ankylosis that only represents failure by the orthodontist to analyze and treat the problem. Even the 'true' ankylosis is a relative term. Teeth that don't respond to traction can be treated, if you happen to live where there are interested specialists, by transplantation and apictomy, see below.
What's new? Technology and techniques.
Extracting baby canines
It is standard procedure* to extract the baby canines, if the permanent canines are slow in responding. There are other procedures that can be added to this, in hope of making it easier for the permanent teeth to erupt:
- cervical pull headgear
- double extraction of the primary canine and the first molar
- a transpalatal arch (TPA)
- TPA combined with rapid maxillary epansion
(*'Standard procedure', but not actually scientifically proven, see below under 'good science, bad science, no science').
CBCT
The emergence of cone beam computer tomography (CBCT) around 2000, is going to be of major importance,and frankly, I don't understand why it is not a standard diagnostic tool right now, especially since the radiation now is comparable to a panoramic.
Actually, I suspect most orthodontists don't know what to do with CBCT. With technology, more training will be necessary. Orthodontists dealing with impacted teeth will have to be able to interpret the images, and generally know their way around. You need biomechanical knowledge, and a spatial imagination to solve a tangle of teeth in the tougher cases.
For the 3 D images, there are computer programs, like Anatomage (see anatomage.com) with software that allows you to create models that make molds obsolete. '3D imaging - the Light in the Attic' (8) describes a case where 'a potentially disastrous outcome was averted'. A patient with bilateral maxillary impacted canines, had the right canine on top of the incisor ('buccally'), but the left canine behind the incisor ('palataly') . Usually (95% of the time) the impacted teeth are both on the same side of the incisors. So in this case, following the 95% rule, and not knowing the real scenario,it would have been damaging to this patient's case.
With the Anatomage, and all the newer software programs that will developed, you can simulate different scenarios, to see what results you would get from different treatment plans, which sounds like a time saver.
suresmile.com. is something in the same vein I think. It can shorten treatment time (5), for an extra $ 1000 or so, but I don't know if it is useful for impacted teeth specifically; though it does rely on 3 D imaging, which can't hurt. There is very limited real information on the company website and not too many studies.
The 3D imaging quality and use is dependent of the software, and orthodontics are definitely going to be more and more high-tech. The problem seems more to be in how orthodontists are going to keep up with it and who
is going to be able to use technology to its fullest. For patients it will hopefully be the end of pulling here, then there, and trying things blindly. Here's an article I don't understand, but it gives a taste of what is to come:
http://www.dental-tribune.com/articles/specialities/orthodontics/11545_cbct_in_orthodontics.html
There are biomechanical techniques that are useful in some cases, but have to be mastered, such as skeletal anchorage (6). Instead of using anchor teeth that are used as attachments for pulling on the canine, a fixed implant is put into bone. That way you don't risk negative consequences on the neighboring teeth and the arch
when pulling on the canines. The principle is Newton's third law: For every action there is an equal and opposite
re-action. Pulling on a canine, might instead pull on the anchor teeth.
(skeletal anchorage instead of dental) are invaluable in assessing the prognosis of canine movement
before appliance placement. They allow the orthodontist to plan treatment that may have been previously
unpredictable or even impossible with tradtional mechanics...
...less reactive forces are applied to the adjacent teeth, and the danger of negative deleterious side
effects, such as root resorption or uncontrolled movement of anchor teeth is significantly decreased.
Treatment of the impaction may be performed separately before or even simultaneously with treatment
of the remainder of the dentition, as 2 distinct force systems.(pp 239-40)(6)
Grafting:
When you operate you can do it 'closed', covering the tooth with a tissue flap, or 'open' ,
it would seem that surgical exposure with careful attention to the periodontal tissues and orthodontic
alignment without intentional closing over with soft tissue could provide a more predictable result for
patients who require interdisciplinary management of ectopically positioned teeth. The value of grafting
is similar to going from a two-dimensional radiograph to a 3-dimensioinal cone beam tomography
imaging for localization of ectopically positioned teeth. (p 221)(2)
Auto transplantation:
Extracting baby canines
It is standard procedure* to extract the baby canines, if the permanent canines are slow in responding. There are other procedures that can be added to this, in hope of making it easier for the permanent teeth to erupt:
- cervical pull headgear
- double extraction of the primary canine and the first molar
- a transpalatal arch (TPA)
- TPA combined with rapid maxillary epansion
(*'Standard procedure', but not actually scientifically proven, see below under 'good science, bad science, no science').
CBCT
The emergence of cone beam computer tomography (CBCT) around 2000, is going to be of major importance,and frankly, I don't understand why it is not a standard diagnostic tool right now, especially since the radiation now is comparable to a panoramic.
Actually, I suspect most orthodontists don't know what to do with CBCT. With technology, more training will be necessary. Orthodontists dealing with impacted teeth will have to be able to interpret the images, and generally know their way around. You need biomechanical knowledge, and a spatial imagination to solve a tangle of teeth in the tougher cases.
For the 3 D images, there are computer programs, like Anatomage (see anatomage.com) with software that allows you to create models that make molds obsolete. '3D imaging - the Light in the Attic' (8) describes a case where 'a potentially disastrous outcome was averted'. A patient with bilateral maxillary impacted canines, had the right canine on top of the incisor ('buccally'), but the left canine behind the incisor ('palataly') . Usually (95% of the time) the impacted teeth are both on the same side of the incisors. So in this case, following the 95% rule, and not knowing the real scenario,it would have been damaging to this patient's case.
With the Anatomage, and all the newer software programs that will developed, you can simulate different scenarios, to see what results you would get from different treatment plans, which sounds like a time saver.
suresmile.com. is something in the same vein I think. It can shorten treatment time (5), for an extra $ 1000 or so, but I don't know if it is useful for impacted teeth specifically; though it does rely on 3 D imaging, which can't hurt. There is very limited real information on the company website and not too many studies.
The 3D imaging quality and use is dependent of the software, and orthodontics are definitely going to be more and more high-tech. The problem seems more to be in how orthodontists are going to keep up with it and who
is going to be able to use technology to its fullest. For patients it will hopefully be the end of pulling here, then there, and trying things blindly. Here's an article I don't understand, but it gives a taste of what is to come:
http://www.dental-tribune.com/articles/specialities/orthodontics/11545_cbct_in_orthodontics.html
There are biomechanical techniques that are useful in some cases, but have to be mastered, such as skeletal anchorage (6). Instead of using anchor teeth that are used as attachments for pulling on the canine, a fixed implant is put into bone. That way you don't risk negative consequences on the neighboring teeth and the arch
when pulling on the canines. The principle is Newton's third law: For every action there is an equal and opposite
re-action. Pulling on a canine, might instead pull on the anchor teeth.
(skeletal anchorage instead of dental) are invaluable in assessing the prognosis of canine movement
before appliance placement. They allow the orthodontist to plan treatment that may have been previously
unpredictable or even impossible with tradtional mechanics...
...less reactive forces are applied to the adjacent teeth, and the danger of negative deleterious side
effects, such as root resorption or uncontrolled movement of anchor teeth is significantly decreased.
Treatment of the impaction may be performed separately before or even simultaneously with treatment
of the remainder of the dentition, as 2 distinct force systems.(pp 239-40)(6)
Grafting:
When you operate you can do it 'closed', covering the tooth with a tissue flap, or 'open' ,
it would seem that surgical exposure with careful attention to the periodontal tissues and orthodontic
alignment without intentional closing over with soft tissue could provide a more predictable result for
patients who require interdisciplinary management of ectopically positioned teeth. The value of grafting
is similar to going from a two-dimensional radiograph to a 3-dimensioinal cone beam tomography
imaging for localization of ectopically positioned teeth. (p 221)(2)
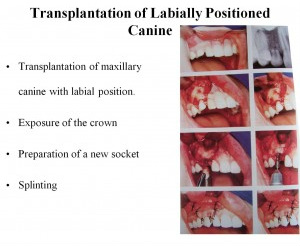
Auto transplantation:
|
Moving a tooth surgically to a new position. The root has to be between 50 and 75% formed (29) according to one author, Dr. Pamela L. Alberto, but that more ideally, if you hope the tooth will revascularize.
An expert on dental tranpslantation is Dr. Jens O. Andreasen an oral surgeon in Copenhagen. He is mainly a specialist in trauma and has a wonderful website: dentaltraumaguide.org. Dr. Heithersay, an endodontist in Adelaide, Australia, describes two cases of transplantation in patients with PEIR, if you look under 'Sam's case'. |
http://www.intelligentdental.com/2012/01/18/impacted-teeth-part-2/
|
Here's a quote from the chapter 'Autotransplantation of Teeth (Lars Andersson, Mitsuhiro Tsukiboshi, and Jens O Andreasen) in 'Oral and Maxillofacial Surgery' (31):
Teeth with roots under the development are easier to extract and have better prognosis. Developing teeth
can revascularize while fully developed teeth do not revascularize and have to be endodontically treated. It
is also important to take into consideration the development and growth status of the individual and an
interdisciplinary approach is important when planning. (281)
...
In young growing patients implant treatment is contraindicated in the anterior maxillary region becuse it
stops the vertical growth of the alveolar process and it can be difficult to achieve a good esthetic final result
if an implant is placed before growth is completed. To support the development of normal tissue in the
trauma area and to secure growth and development of the alveolar process in an individua who is still
growing, tranplantation of the tooth is an excellent form of treatment. (p 283)
I approached Dr Heithersay, an endodontist in Australia, and he described how they had treated two impacted
teeth with PEIR with autotransplantation, and it looked like a success two years post transplantation: click.
Teeth with roots under the development are easier to extract and have better prognosis. Developing teeth
can revascularize while fully developed teeth do not revascularize and have to be endodontically treated. It
is also important to take into consideration the development and growth status of the individual and an
interdisciplinary approach is important when planning. (281)
...
In young growing patients implant treatment is contraindicated in the anterior maxillary region becuse it
stops the vertical growth of the alveolar process and it can be difficult to achieve a good esthetic final result
if an implant is placed before growth is completed. To support the development of normal tissue in the
trauma area and to secure growth and development of the alveolar process in an individua who is still
growing, tranplantation of the tooth is an excellent form of treatment. (p 283)
I approached Dr Heithersay, an endodontist in Australia, and he described how they had treated two impacted
teeth with PEIR with autotransplantation, and it looked like a success two years post transplantation: click.
Apicotomy of dilacerated roots: see dilacerated root
Even ankylosis is a relative term. If the apex, tip, of the tooth is stuck, it can be broken off, and the tooth can
be moved. This is the restorative version of apicotomy, not the one associated with root filling! This is a technique
by Dr Edela Puricelli.
Partial maxillary osteotomy
This is also a technique that Dr Puricelli has 'invented'.
Even ankylosis is a relative term. If the apex, tip, of the tooth is stuck, it can be broken off, and the tooth can
be moved. This is the restorative version of apicotomy, not the one associated with root filling! This is a technique
by Dr Edela Puricelli.
Partial maxillary osteotomy
This is also a technique that Dr Puricelli has 'invented'.
Old discarded techniques
I thought it was interesting to find this older article from 1981: 'Treatment of Impacted Cuspids -The Hazard Lasso' (sic! not even the 'hazard of'(37)). The authors warn against a 'long used' technique of putting a wire all around the impacted canine instead of the, at the time, the newer technique of bonding some kind of bracket to pull on. The lasso method often caused ankylosis.
Additionally, the movement of an impacted tooth involves risks of discoloration, devitalization, root
resorption, loss of cervical bone and long clinical crown with lack of attached gingivae. The patient and/or
parents should be fully aware of these risk factors.
I thought it was interesting to find this older article from 1981: 'Treatment of Impacted Cuspids -The Hazard Lasso' (sic! not even the 'hazard of'(37)). The authors warn against a 'long used' technique of putting a wire all around the impacted canine instead of the, at the time, the newer technique of bonding some kind of bracket to pull on. The lasso method often caused ankylosis.
Additionally, the movement of an impacted tooth involves risks of discoloration, devitalization, root
resorption, loss of cervical bone and long clinical crown with lack of attached gingivae. The patient and/or
parents should be fully aware of these risk factors.
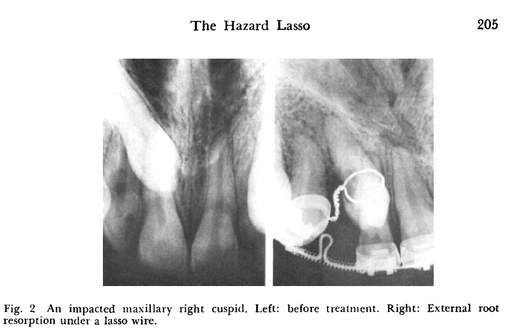
In the cases presented in the article, the lasso cause surface resorption that seemed to continue even after the lasso was removed, that killed two teeth, in another case the surgery to put the lasso on, fractured the root of the adjacent tooth.
Advancement in dentistry is something humankind is very appreciative of. With the internet, and international collaboration, all kind of advancements can and should be much accelerated.
Advancement in dentistry is something humankind is very appreciative of. With the internet, and international collaboration, all kind of advancements can and should be much accelerated.
Options and opinions
Even though impacted teeth seem common enough that there should be enough collective experience to make more intelligent decisions about how to go about the treatment, medicine often fails collecting and analyze all data that would be available if you could have everyone report cases, treatment and outcomes. I have a feeling that the orthodontists out there are their own islands. I don't think there is any reporting of good/bad outcomes that can identify who are the 'impact competent' orthodontists.
I've now looked at enough pictures and read plenty of case descriptions, where the authors describe dilemmas, technical manipulations and solutions, that I can see the art of it. Sadly, in reality, all orthodontist are not a Michelangelo.
As one study points out, 'the strategy for managing unerupted teeth has been debated for more than half a century' (2). Looking at the back cover of Dr. Adrian Becker's 2nd edition of 'On the Treatment of Impacted Teeth', 2007 (3), there can also be controversy between orthodontists and oral surgeons:
Impacted teeth present an ongoing challenge to the dental profession, and several of its
specialities have offered treatment strategies in widely differing styles. In the long term, it has come to
be recognized that superior results are obtainable through the orthodontic/surgical modality. There is,
however, a considerable difference of opinion between these two specialities as to which procedures
should be carried out first and to what lengths each should be pursued. There are controversies, too,
within the two disciplines regarding what is good practice and what is bad.
So, do you feel lucky...?
Even though impacted teeth seem common enough that there should be enough collective experience to make more intelligent decisions about how to go about the treatment, medicine often fails collecting and analyze all data that would be available if you could have everyone report cases, treatment and outcomes. I have a feeling that the orthodontists out there are their own islands. I don't think there is any reporting of good/bad outcomes that can identify who are the 'impact competent' orthodontists.
I've now looked at enough pictures and read plenty of case descriptions, where the authors describe dilemmas, technical manipulations and solutions, that I can see the art of it. Sadly, in reality, all orthodontist are not a Michelangelo.
As one study points out, 'the strategy for managing unerupted teeth has been debated for more than half a century' (2). Looking at the back cover of Dr. Adrian Becker's 2nd edition of 'On the Treatment of Impacted Teeth', 2007 (3), there can also be controversy between orthodontists and oral surgeons:
Impacted teeth present an ongoing challenge to the dental profession, and several of its
specialities have offered treatment strategies in widely differing styles. In the long term, it has come to
be recognized that superior results are obtainable through the orthodontic/surgical modality. There is,
however, a considerable difference of opinion between these two specialities as to which procedures
should be carried out first and to what lengths each should be pursued. There are controversies, too,
within the two disciplines regarding what is good practice and what is bad.
So, do you feel lucky...?
Good Science - Bad Science - No Science
I came across this paper: 'Extraction of primary (baby) teeth for unerupted palatally displaced permanent canine teeth in children (Review)' by the Cochrane Collaboration. According to Wikipedia this is an "independent nonprofit organization consisting of a group of more that 31,000 volunteers in more than 120 countries...formed to organize medical research information in a systemic way to facilitate the choices that health professionals, patients, policy makers and others face in health interventions according to the principles of evidence-based medicine. The group conducts systemic reviews of randomized controlled trials of health-care interventions, which it publishes in the Cochrane Library." (For more on this group, see cochrane.org).
The article published in 2009 found that a lot of the published articles and studies on the subject of whether it helps the permanent canines if the baby canines are extracted at age 10-13, found that the studies available were flawed and could not confirm this. The practice is mainly based on a trial in 1988 where 'the major flaw...was the absence of a control group'. The Cochrane review team came to the same conclusion in 2012. An article on 'open versus closed surgical exposure of canine teeth that are displaced in the roof' 2008 said there was a lack of high quality studies to make any recommendations. It is up to the orthodontist/oral surgeon's judgement what technique is chosen.
As relates to impacted canines, I do wonder on what evidence-based science treatments* are used: Why is it that
you should wait 1-2 weeks before applying traction after expose & bond according to most oral surgery/orthodontist websites: while Dr. Becker says that being present at surgery and applying immediate traction gives him an advantage? Why does one orthodontist have 2 weeks in between visits and UCSF 5 weeks?
A continued education test (36) describes how after a platal impacted canine has been exposed there should be 'light orthodontic force (not to exceed 60g or 2 oz)". Is that a fact that has been scientifically proven?
The science is obviously missing in a lot of instances. Data is not collected, there is no way to know the success rate of different strategies and individual professionals.
When you are dealing with something like 'impacted canines' that occurs in about 1-2% of the population, you are dealing with something that is frequent enough that all orthodontists will encounter it, but it is not frequent enough that you will get good at it, unless you actually read about it and learn about it actively.
I came across this paper: 'Extraction of primary (baby) teeth for unerupted palatally displaced permanent canine teeth in children (Review)' by the Cochrane Collaboration. According to Wikipedia this is an "independent nonprofit organization consisting of a group of more that 31,000 volunteers in more than 120 countries...formed to organize medical research information in a systemic way to facilitate the choices that health professionals, patients, policy makers and others face in health interventions according to the principles of evidence-based medicine. The group conducts systemic reviews of randomized controlled trials of health-care interventions, which it publishes in the Cochrane Library." (For more on this group, see cochrane.org).
The article published in 2009 found that a lot of the published articles and studies on the subject of whether it helps the permanent canines if the baby canines are extracted at age 10-13, found that the studies available were flawed and could not confirm this. The practice is mainly based on a trial in 1988 where 'the major flaw...was the absence of a control group'. The Cochrane review team came to the same conclusion in 2012. An article on 'open versus closed surgical exposure of canine teeth that are displaced in the roof' 2008 said there was a lack of high quality studies to make any recommendations. It is up to the orthodontist/oral surgeon's judgement what technique is chosen.
As relates to impacted canines, I do wonder on what evidence-based science treatments* are used: Why is it that
you should wait 1-2 weeks before applying traction after expose & bond according to most oral surgery/orthodontist websites: while Dr. Becker says that being present at surgery and applying immediate traction gives him an advantage? Why does one orthodontist have 2 weeks in between visits and UCSF 5 weeks?
A continued education test (36) describes how after a platal impacted canine has been exposed there should be 'light orthodontic force (not to exceed 60g or 2 oz)". Is that a fact that has been scientifically proven?
The science is obviously missing in a lot of instances. Data is not collected, there is no way to know the success rate of different strategies and individual professionals.
When you are dealing with something like 'impacted canines' that occurs in about 1-2% of the population, you are dealing with something that is frequent enough that all orthodontists will encounter it, but it is not frequent enough that you will get good at it, unless you actually read about it and learn about it actively.
Studies of outcome:
- A study at University of Toronto, Canada (16), 1998, with 82 impacted maxillary canines in 54 patients, 12 to 16 years old, had all canines erupt successfully with exposure and bonding. Complications consisted of: failure of initial bond, at the time of surgery, which required rebonding; premature debonding at the time of pack removal and; debonding of brackets during orthodontic eruption. There was no infection, eruption failure, ankylosis, resorption or periodontal defect (pocket greater than 3 mm) associated with any of the exposed teeth. They did recommend that patients were treated before the age of 20 to ensure success.
- One study (2) with 80 patients (age 12-24, average 16) treated surgically and orthodontically, for
146 palatally bone impacted canines (so it seems the majority of patients had bilaterally impacted
maxillary canines) had the following outcome: 70, 54% were successful, 43 canines (29 %) had
to be extracted because of ankylosis.
- A study by Dr. Becker (3) of 19 adults (age 20-47, mean age 28.8) with 23 impacted maxillary canines was compared to a younger control group (age 12-16, mean age 13.7) with similar degree of difficulty. The success rate among the adults was 69.5% compared to 100% in the younger group. The failed canines were all in patients older than 30.
- 'Analysis of failure in the treatment of impacted maxillary canines' by Dr. Becker, a study
with 28 patients (age 17.4 +/- 4.3 years) and 37 teeth that were referred, showed that revised treatments had a success rate of 71.4%. (4). As for the reasons of initial failure the conclusion was:
Inaccurate 3-dimensional diagnosis of location and orientation of impacted teeth and failure to appreciate
anchorage demands were the major reasons for failure in the treatment of impacted canines. (p 743)(14)
This study proves to me that if an orthodontist is stumped, it is of the utmost importance that there is somewhere to refer patients, somewhere where a level of expertise and scientific curiosity is concentrated.
- 'Failure after closed traction of an unerupted maxillary permanent canine: Diagnosis and treatment planning' (17), shows again the importance of taking a second look at a case. A 13-year-old-girl had no effect of 6 months of traction, at renewed surgery,the chain appeared to be osseointegrated. With a new chain and 16 months of traction there was success.
- CT study' (19), relates the cases of 9 patients. 4 canines had to be extracted due to ankyolsis, some kind of blockage, or horizontal positioning. One failure was attributed to the formation of a 'periapical granuloma' where the authors speculated about its origin:
The cause of inflammation and the external resorption which were not present at the X-ray image
could be caused by indelicate surgical intervention and subsequent complicated healing, or that
the periapical granuolma is of nasal origin. (p.167)
They had 5 cases with success after intervention. One case sacrificed an incisor, moved the roots of adjacent teeth and made more space through varying degrees of manipulation.
Last recourse (you should hope), extraction!
Pulling out any permanent tooth is not trivial. It is something where your parental knee-jerk reaction is horror, unless it is a wisdom tooth. A canine is a very important part of the dental arch, the corner 'stones'; they have the longest, most massive roots. To lose them is not an easy thing to make up for. This is another quote from Dr. Becker, on the scenario of pulling out a maxillary canine or incisor:
The space may be held open for a future implant which, in a 12-year-old child, may not be for 6
or 8 years. During this time a temporary replacement needs to be made, with all the negative
implications. During this time we will also see a gradually diminishing alveolar bone ridge in this
small edentulous area and the deficiency will be even greater in the months and years after
extraction of the aberrant tooth. When the patient reaches 18 years of age, the implantologist
will be faced with daunting prospect of a severely defective ridge and a questionable prognosis for
the implant.(p 223) (21)
Sadly, there are cases when the best alternative is extraction, the canine is no good for some reason,
it is hurting the surrounding teeth, or it is irreversibly stuck = ankylosed. However, science and research are at work in different parts of the world, so for example the 'dilaceration' quoted below, can be treated in Brasil with
apicotomy or transplantation. In time 'ankylosed' is something that can be overcome.
Extraction indications according to Bishara (16) are:
1. ankylosis and impossible tooth transplantation
2. severe root dilaceration
3. severe retention (lodged between lateral and incisor roots, horizontal placement), in which
surgical uncovering and orthodontic extrusion will hold risks
4. first premolar is in the position of the canine, there is good occlusion and well aligned teeth
5. pathological changes around the tooth (cysts etc.) and the patient is unwilling to be
orthodontically treated (p 121)(17?)
The same article goes on:
Complications related to the extraction of palatally impacted canines are numerous (5):
huge bone defects, damage of adjacent teeth (luxation, comprised parodontium, root fractures)
involvement of maxillary sinus, neuropathies. That is why similar kind of intervention is
usually a last clinical approach to ectopic upper canines. Carried out properly and in close
collaboration with a radiologist, a surgeon, and an orthodontist, it leads to satisfactory results.
(p.121)(17?)
My conclusions:
From the outset: Chose your orthodontist wisely. Likewise your oral surgeon.
If you get to the point where your orthodontist gives up on a tooth and talks of extraction, you would want him to tell you why. Not in general terms of age, localization, or degree of root formation; but rather more specifically related to your case. It also seems that extraction is something that the orthodontist would need to discuss with the oral surgeon. Be suspicious if you are handed a referral that just says 'extraction please'. In some instances only renewed surgery can disclose a reason (see the case above of the 13-year-old girl where the chain got stuck (17)).
You have to keep an open mind with impaction. Make sure you are comfortable with decisions made or get a second opinion. And if your orthodontist doesn't mention CBCT...run!
From the outset: Chose your orthodontist wisely. Likewise your oral surgeon.
If you get to the point where your orthodontist gives up on a tooth and talks of extraction, you would want him to tell you why. Not in general terms of age, localization, or degree of root formation; but rather more specifically related to your case. It also seems that extraction is something that the orthodontist would need to discuss with the oral surgeon. Be suspicious if you are handed a referral that just says 'extraction please'. In some instances only renewed surgery can disclose a reason (see the case above of the 13-year-old girl where the chain got stuck (17)).
You have to keep an open mind with impaction. Make sure you are comfortable with decisions made or get a second opinion. And if your orthodontist doesn't mention CBCT...run!
One silver lining on this whole ordeal has been reading Dr. Adrian Becker's work. He is not only good with impacted teeth, he is good with words! His description of cases reads like a detective story, and the knowledge and thoughtfulness he displays when dealing with a problem tooth is amazing. Who thought orthodontics could be entertaining?!
These cases are the failed, partially failed or eeked-out-result cases and they deserve to be analysed as to what went wrong, why it went wrong, what was done to turn the case around and to what degree the outcome was compromised. It will be seen that there are such a large number and range of operative variables involved, from both the orthodontic and surgical aspects, that evidence-based recommendations are hard to come by and clinical experience and common sense must reign supreme. Nevertheless, cases of this type provide much material for discussion for what we may learn from their management and from a study of the clinical decisions that were made during the treatment. (Dr. Beckers Newsletter December 2011)
Also, other people at the cutting-edge of treatment and research around the world are very accessible and not only shows an academic interest, but a personal interest and concern for the individual patient. Some articles that I couldn't access in full, have been sent to me, and my questions have been answered by Dr. Heithersay in Australia, Dr Al-Batayneh in Jordan and Dr. Araújo in Brazil.
(1) Becker A, Chaushu G, Chaushu S. Analysis of failure in the treatment of impacted
canines, Am J Orthod Dentofacial Orthop. 2010 Jun; 137(6): 743-54.
(2) Robert L., Vanarsdall Jr., Efficient Management of Unerupted Teeth: A Time-Tested
Treatment Modality, Seminars in Orthodontics, Vol 16, No 3 (September), 2010:pp
2122-221.
(3) Dr. Adrian Becker is Clinical Associate Professor, Department of Orthodontics, Hebrew
University-Hadassah School of Dental Medicine, Jerusalem, Israel.
The third edition of his "On the Treatment of Impacted Teeth' came out in the spring of
2012.
http://www.dr-adrianbecker.com/page.php?pageId=281&nlid=9
Dr. Becker gives online clinical consultations for a small fee!
(5) Timothy J. Alford, W. Eugene Roberts, James K. Hartsfield Jr, George J. Eckert, and
Ronald J. Snyder (2011) Clinical outcomes for patients finished with the SureSmile™
method compared with conventional fixed orthodontic therapy.
The Angle Orthodontist: May 2011, Vol. 81, No. 3, pp. 383-388.doi:
http://dx.doi.org/ 10.2319/071810-413.1
(6) Chaushu S, Chaushu G. Skeletal Implant Anchorage in the Treatment of Impacted Teeth -
A Review of the State of the Art. Seminars in Orthodontics, Vol 16, No 3 (September),
2010: pp 234-241.
(7) 'The average treatment duration for a case with impacted teeth is at least 2 years for the
unilateral-impacted group and almost 3 years for the bilateral-impacted canine group.'
(p. 235)(6)
(8) Quintero J-C.'3-D imaging; the light in the attic', Ortho Tribune',
(9) http://www.grortho.gr/hor/2006v09i1/05%20kalavritinos.pdf
(11) http://www.dr-adrianbecker.com/page.php?pageId=281&nlid=9
Dr. Becker gives online consultations, for orthodontists or patients, for a small fee!
(12) Motamedi et al. Assessement of radiographic factors affecting surgical exposure an orthodontic alignement
of impacted canines of the palate; a 15-year retrospective study. Oral Surg Oral Med Pathol Oral Radiol
Endod 2009 Jun;107(6):772-5. 2009 Feb 8. from the Dental College of Teheran, Iran.
(13) Becker A., Chaushu S. Success rate and duration of orthodontic treatment for adult patients with palatally
impacted maxillary canines. American Journal of Orthodontics & Dentofacial Orthopedics;Volume 124
Issue 5, Pages 509-514, November 2009
(14) Becker A, Chaushu G, Chaushu S. Analysis of failure in the treatment of impacted canines, Am J Orthod
Dentofacial Orthop.2010 Jun; 137(6): 743-54.
(15) Yordanova et al., JofIMAB;Issue 2011,vol. 17, book 2/ from the Faculty of Dental Medicine, Medical
University - Plodiv,Bulgaria.
(16) Bishara SE. Clinical management of impacted maxillary canines. Semin Orthod 1998 Jun;4(2):87-98
(17) Frank Ch. Treatment options for impacted teeth. J Am Dent Assoc. 2007;131: 623-632.
(18) Bonetti et al. Failure after closed traction of an unerupted maxillary permanent canine: Diagnosis and
treatment. Am J Orthod Dentofacial Orthop 2011 Jul;140(1):121-5
(19) Dr. Adrian Becker is Clinical Associate Professor, Department of Orthodontics, Hebrew University-Hadassah
School of Dental Medicine, Jerusalem, Israel. website: www.dr-adrianbecker.com.
The third edition of his "On the Treatment of Impacted Teeth' came out in the spring of 2012
(20) Cernochova P, Krupa P. Analysis of the causes for failure of the surgical - orthodontic treatment of
impacted permanent canines - CT study. Scripta Medica (BRNO) -78(3):161-170, August 2005. from
Faculty of Medicine, Masaryk University,Brno,Czeck Republic.
(21) Becker, A. Extreme Tooth Impaction and its Resolution. Seminars in Orthodontics, Vol 16, No 3
(September), 2010:pp 223.
(23) Chaushu S, Chaushu G. Skeletal Implant Anchorage in the Treatment of Impacted Teeth - A Review of the
State of the Art. Seminars in Orthodontics, Vol 16, No 3 (September), 2010: pp 234-241.
(24) http://www.ortho-tribune.com/articles/content/id/574/scope/specialities/region/usa
(25) On the subject of whether to create space for the impacted teeth first, usually the best solution, or to to
operate and apply traction first, see Dr. Adrian Becker's website, September 2011 newsletter: 'Should we
always create space in the dental arch for an impacted canine,before it is exposed? (1))
(26) http://www.ncbi.nlm.nih.gov/pubmed/9785687
(27) http://ajodoblog.blogspot.com/2012/07/letter-attempted-traction-of-impacted.html. American Journal of
Orthodontics and Dentofacial Orthopedics, July 31, 2012. Comment by DMD MSD Ron Parsons, Duluth, GA.
Commented on: http://www.ajodo.org/article/S0889-5406(12)00357-5/abstract
American Journal of Orthodontics & Dentofacial Orthopedics Volume 142, Issue 1 , Pages 106-114, July
2012, "Attempted traction of impacted and ankylosed maxillary canines" by Vinícius de Oliveira and
Matheus Melo Pithon Abstract The aim of this article is to report the clinical orthodontic treatment of an
adult patient with 2 impacted maxillary canines. Traction was applied to the impacted teeth; however,
after 7 months, the teeth were found to be ankylosed and
were extracted. The extraction spaces were closed by moving the posterior teeth mesially with mini-
implant anchorage. The
results were satisfactory, with the premolars in the functional position of the canines.
(28) http://www.dr-adrianbecker.com/page.php?pageId=281&nlid=54
(29) Selected Readings OMS: http://selectedreadingsoms.com/wp-content/uploads/2012/03/Alberto19.3.pdf
(30) http://www.dentist.ie/_fileupload/2009%2055%20No_%205%20-%20Oct%20Nov.pdf
(31) Oral and Maxillofacial Surgery. edited by Lars Andersson, Karl-Erik Kahnberg, Anthony Pogrel. 2010
(33) Chaushu S, Abramovitz I, Becker A. Failure in the orthodontic treatment of impacted maxillary canines.
Refuat Hapeh Vehashiinayim, 2013 Apr;30(2): 42-52,81.
(34) Osorio et al. Apicotomy as treatment for failure of orthodontic traction. Pubmed Case Rep Dent.
2013.:168232)
(35) David P. Mathews, Vincent G. Kokich. Palatally impacted canines: The case for preorthodontic uncovering
and autonomous eruption. AJO-DO April 2013. Vol 143. Issue 4.
(36) dentalCEtoday.com
(37) Shapira Y, Kuftinec M. Treatment of Impacted Cuspids - The Hazard Lasso. The Angle. Vol. 51, No. 3,
July 1981.
(38) Caminiti et al. Outcomes of the surgical exposure, bonding and eruption of 82 impacted maxillary canines.
Journal of the Canadian Dental Association. Vol 64, issue 8.
* Interesting npr story on Koch, Pasteur, Arthur Conan Doyle and tb in "The Remedy" by Thomas Goetz.
At the time, around 1875, 'medical science' started getting used as a term as opposed to 'plain' medicine.
The term of our time and age is evidently 'evidence-based' science, as opposed to 'plain' science.